ASCO GU 2020
ASCO GU 2020
Randomized phase 2 study of sipuleucel-T (Sip-T) with or without radium-233 (Ra-223) in men with bone metastatic castration-resistant prostate cancer - Poster
- Details
View poster as PDF
Related Content:
ASCO 2020: Results of the Randomized Phase II Study of Sipuleucel-T +/- Radium-223 in Men with Bone-Metastatic Castration-Resistant Prostate Cancer
Changing the Mechanism of Action in The Treatment of Metastatic Castration-Resistant Prostate Cancer (mCRPC) - Phillip Koo
ASCO GU 2020: Results from BLASST-1 - Nivolumab, Gemcitabine, and Cisplatin in Muscle Invasive Bladder Cancer (MIBC) Undergoing Cystectomy.
- Details
ASCO GU 2020: Combining Chemotherapy with Novel Agents, Opportunities, and Challenges.
- Details
ASCO GU 2020: Best of Journals: Renal Cell Carcinoma - The Surgeon’s Perspective
- Details
ASCO GU 2020: Best of Journals: Renal Cell Carcinoma - The Pathologists Perspective
- Details
ASCO GU 2020: Efficacy of Olaparib by Prior Taxane Use in Patients with Metastatic Castration-Resistant Prostate Cancer and Homologous Recombination Repair Gene Alterations: The PROfound Trial
- Details
Prior taxane chemotherapy was allowed and was a stratification factor in the study.
Multiple therapy options now exist for patients with mCRPC, yet there is a paucity of data on optimal sequence of therapies. In this analysis, the investigators performed a pre-planned analysis to evaluate the efficacy of olaparib in men with HRR-deficient mCRPC based on whether or not they received prior taxane chemotherapy.
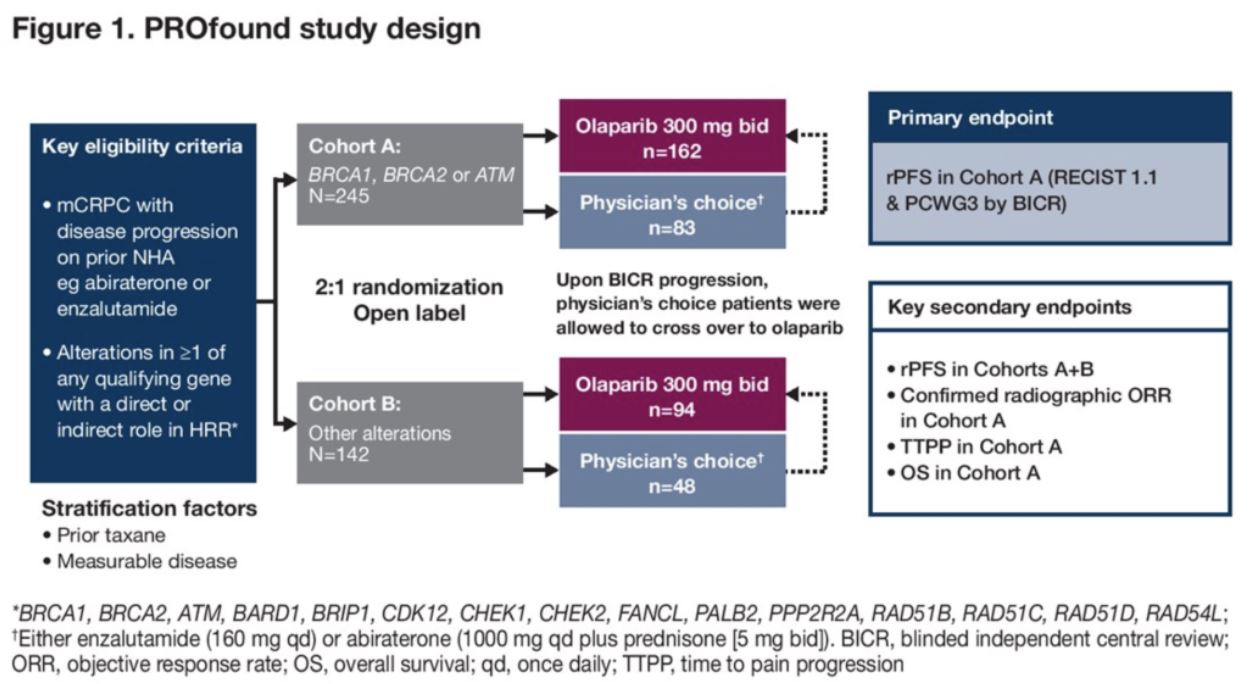
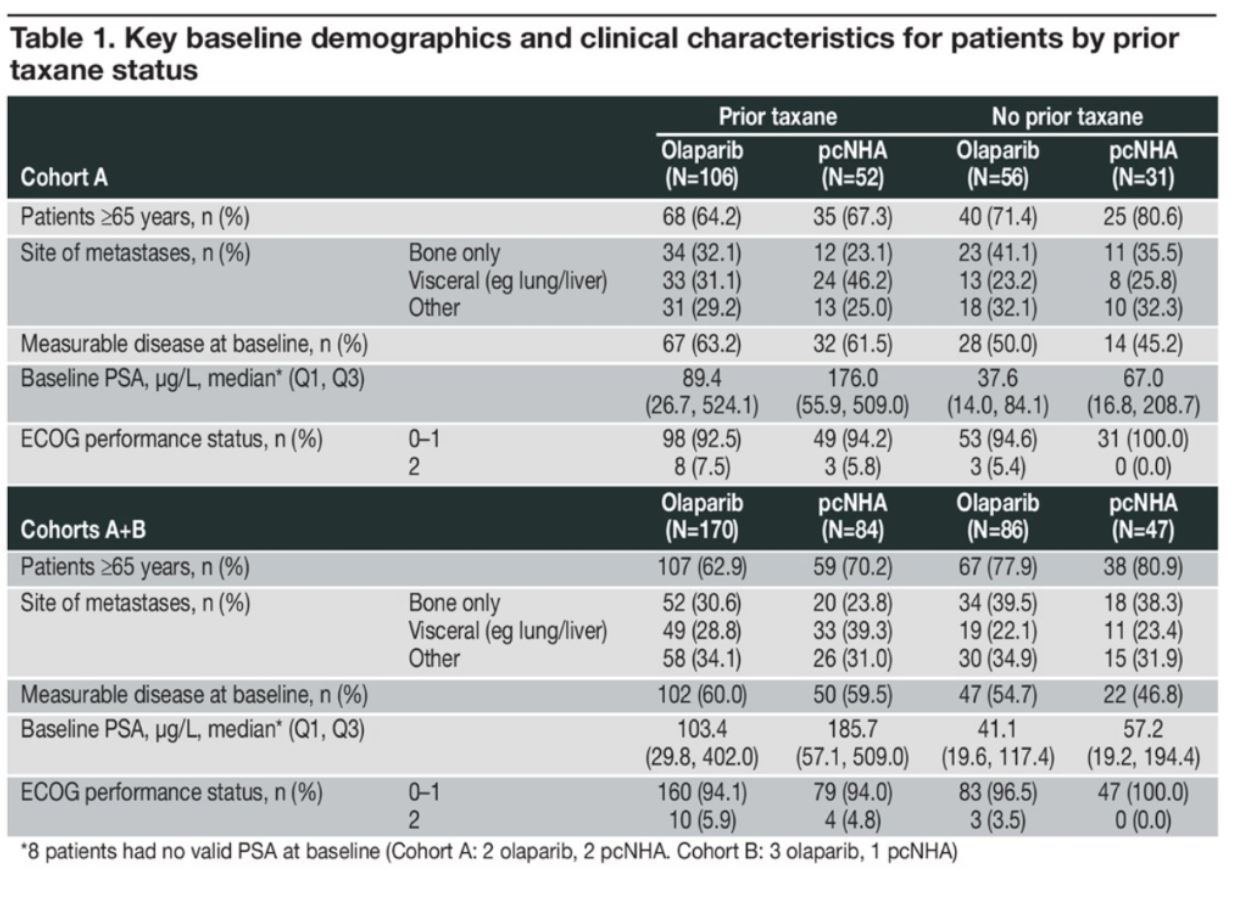
Approximately two-thirds of patients on both the olaparib and NHA treatment arms and across both Cohort A (alterations in BRCA1, BRCA2, or ATM) and Cohort A+B (alterations in any of the 15 HRR genes) received taxane chemotherapy prior to treatment in the PROfound Study. Key baseline demographics and clinical characteristics for the cohort are shown in Table 1 (below) broken down by prior taxane chemotherapy in the two treatment arms. In both arms, patients who received prior taxane therapy were younger, had slightly higher rates of visceral disease and measurable disease, and had higher PSA levels.
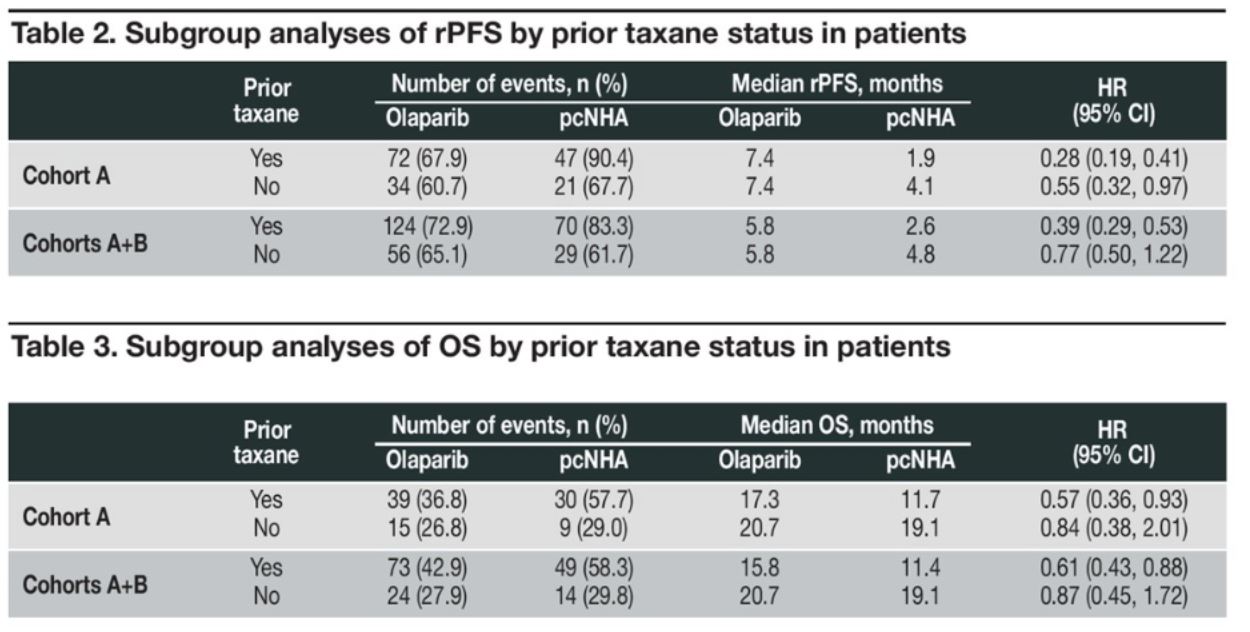
Subgroup analyses of rPFS (below) favored olaparib over NHA regardless of prior taxane chemotherapy in Cohort A and Cohort A+B. This rPFS benefit reached statistical significance (p < 0.05) in all subgroups except Cohort A+B patients who did not receive prior taxane chemotherapy. Subgroup analysis of overall survival (OS) also favored olaparib over NHA, reaching statistical significance in Cohort A and Cohort A+B patients who received prior taxane chemotherapy, but not in those who didn’t. Two important factors must be considered, however in the OS analysis. First, 82% of patients randomized to the NHA arm crossed over to olaparib at the time of rPFS, which may have confounded the OS analysis. Second, the OS data is only modestly mature with only 41% of events at the time of analysis.
In an exploratory analysis, the investigators evaluated outcomes by gene subgroup. Patients with BRCA1/2 or CDK12 alterations both showed improved rPFS and OS for olaparib over NHA with or without prior taxane chemotherapy. Better outcomes for olaparib compared to NHA were also observed in patients with ATM alterations who received prior taxane chemotherapy, but not in those who had not. Of note, these results should be interpreted with caution due to small patient numbers and wide confidence intervals.
The investigators concluded by highlighting that although there are many effective systemic therapies in men with mCRPC, there is a paucity of data regarding optimal sequencing of therapies to guide treatment selection. In the Phase 3 PROfound Study, the benefit of olaparib over NHA was independent of prior taxane use in men with mCRPC with BRCA1, BRCA2, and/or ATM (Cohort A) and in the overall cohort of men with alterations in any of the 15 pre-specified HRR genes (Cohort A+B). These results provide insight into the benefit of olaparib for mCRPC patients regardless of prior taxane chemotherapy.
Presented by: Johann De Bono, MD, PhD, Regius Professor of Cancer Research at the Institute for Cancer Research and the Royal Marsden Hospital, London, United Kingdom
Written by: Jacob Berchuck, MD, Medical Oncology Fellow at the Dana-Farber Cancer Institute (Twitter: @jberchuck) at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California
ASCO GU 2020: Can Advanced Seminoma be Managed with a Risk Stratified Approach?
- Details
ASCO GU 2020: A Phase II Study of Talazoparib in Men with DNA Damage Repair Mutations and Metastatic Castration-Resistant Prostate Cancer
- Details
San Francisco, CA (UroToday.com) Multiple clinical trials are investigating the efficacy of PARP inhibitors in men with metastatic castration-resistant prostate cancer (mCRPC) with somatic and/or germline (DNA damage repair) DDR alterations. Talazoparib is a PARP inhibitor that both inhibits and traps the PARP enzyme with in vitro studies demonstrating that talazoparib has greater PARP-trapping activity than other PARP inhibitors. Talazoparib is FDA approved for women with breast cancer with a germline BRCA1/2 mutation.
ASCO GU 2020: (NEO-BLADE) Phase II Randomized Placebo-Controlled Neoadjuvant Trial of Nintedanib or Placebo with Gemcitabine and Cisplatin in Locally Advanced Muscle Invasive Bladder Cancer
- Details
San Francisco, CA (UroToday.com) Neoadjuvant chemotherapy in resectable muscle invasive bladder cancer (MIBC) results in approximately 30% pathological complete response rates and is associated with improved patient survival. In this presentation, Dr. Syed Hussain presented results from the NEO-BLADE study, which adds the tyrosine kinase inhibitor nintedanib (antagonizes PDGFR, FGFR-1, VEGFR-2) to standard of care gemcitabine and cisplatin. Prior trials with other TKIs such as sunitinib have been hampered by toxicity issues.
ASCO GU 2020: Assessment of Inherited DNA Repair Defects in African-American and Caucasian Men with Prostate Cancer
- Details
San Francisco, CA (UroToday.com) Pathogenic loss-of-function alterations in DNA damage repair (DDR) genes, especially BRCA2, are associated with more aggressive disease and are associated with response to PARP inhibitors in men with prostate cancer. Numerous studies have reported rates of inherited germline DDR (gDDR) alterations in men with prostate cancer, however, these studies are comprised mostly of men of European descent. Comparative data in men of African ancestry is lacking. In this study, investigators utilized germline data from Invitae (a company that provides commercially-available genetic testing services) to compare rates of gDDR (pathogenic and likely pathogenic) alterations in African-American (AA; n = 213) men and Caucasian American (CA; n = 2,488) men. 14 well-annotated DDR genes were evaluated, although not all men were assessed for each of the 14 genes.
ASCO GU 2020: Comparing Nivolumab versus Everolimus with >5 years of Follow-up in Patients with Advanced Renal Cell Carcinoma: A Final Analysis of the CheckMate 025 Trial
- Details
San Francisco, California (UroToday.com) Recent years have seen rapid advancements in the therapy for advanced clear cell renal cell carcinoma (accRCC) with the introduction of first-line combination immunotherapy and immunotherapy/targeted therapy approached. The CheckMate 025 study, previously reported in the New England Journal of Medicine by Dr. Robert Motzer and colleagues in 2015, was a pivotal 2nd-line study of patients with accRCC who had progressed after prior anti-angiogenic therapy. This study firmly established nivolumab as a standard 2nd-line therapy in this patient population. In the Rapid Abstract Session, Dr. Motzer presented the final analysis of CheckMate 025 with over five years of follow-up.
ASCO GU 2020: Results from ATLAS, a Phase 2, Open-Label Trial: Rucaparib for Recurrent, Locally Advanced or Metastatic Urothelial Carcinoma
- Details
San Francisco, California (UroToday.com) The treatment of recurrent/refractory advanced urothelial cancer (UC) remains a challenge. Recent practice-changing studies have firmly established checkpoint inhibitor (CPI) immunotherapy as an option for patients who have progressed after chemotherapy. Furthermore, there has been increasing emphasis to identify patient subsets that may benefit from targeted therapies, such as poly (ADP-ribose) polymerase (PARP) inhibitors for tumors with evidence of DNA repair deficiency. In the Rapid Abstract Session, Dr. Petros Grivas from Seattle Cancer Care Alliance presented findings from ATLAS: a Phase II, open-label trial of rucaparib for locally recurrent or metastatic UC.
ASCO GU 2020: Phase Ib Study of Niraparib plus Androgen Receptor-Targeted Therapy in Patients with Metastatic Castration-Resistant Prostate Cancer
- Details
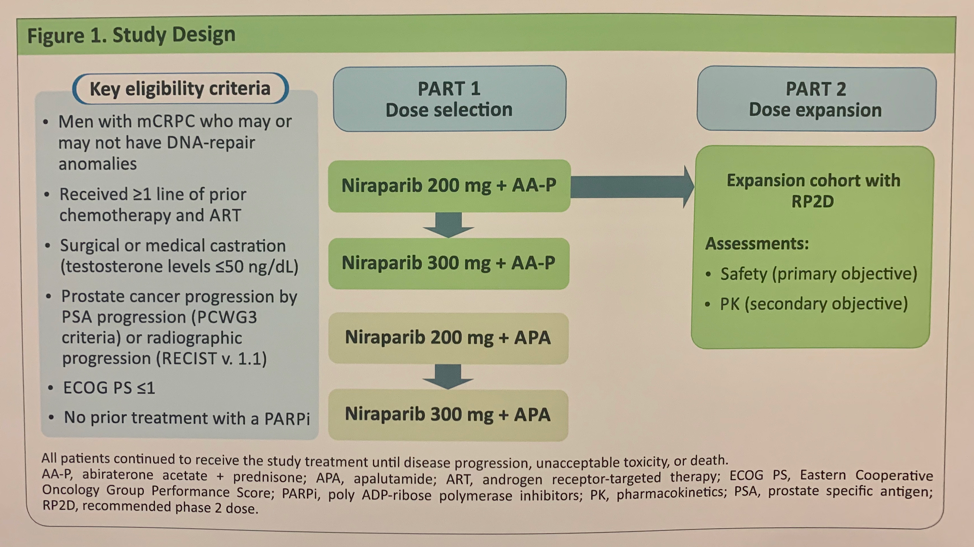
San Francisco, CA (UroToday.com) The combination of PARP inhibitor and androgen receptor-targeted therapy (ART) may induce enhanced therapeutic sensitivity and in patients with metastatic castration-resistant prostate cancer (mCRPC). A subset of mCRPC patients harbor mutations in DNA damage repair (DDR) genes, including BRCA1/2, conferring sensitivity to PARP inhibitors via synthetic lethality. Niraparib is a highly selective PARP inhibitor with potent activity against PARP-1 and PARP-2 enzymes that has demonstrated clinical benefit in second-line mCRPC (GALAHAD study). This phase 1b study, BEDIVERE (NCT02924766), is a multi-center, open-label study of niraparib plus ART, either apalutamide (APA) or abiraterone acetate plus prednisone (AA-P), comprising a dose selection phase (Part 1) with assessment of pharmacokinetics and dose-limit toxicities (DLT) and a dose expansion phase (Part 2). Eligible patients had mCRPC with or without DDR alterations who had received at least 1 line of prior chemotherapy or ART and no prior treatment with PARP inhibitor.
Results of the pharmacokinetic and DLT assessment of the niraparib plus APA combination demonstrated that at a dose of niraparib 200 mg, drug-drug interaction with APA led to low plasma drug levels. At a dose of niraparib 300 mg plus APA, 2 of 3 patients experienced a DLT, one with Grade 4 thrombocytopenia, the other with Grade 3 fatigue and hypertension. Given the pharmacokinetic and DLT results, the niraparib plus APA combination was discontinued.
The niraparib plus AA-P results were more promising. Four patients were treated with niraparib 200 mg plus AA-P with no DLTs. Three of 8 patients treated with niraparib 300 mg plus AA-P experienced DLTs: one with Grade 3 fatigue and Grade 4 elevated GGT, two with neutropenia. Thus, niraparib 200 mg was the recommended Phase 2 dose for combination with AA-P. This dose combination was evaluated in an additional 15 patients in Part 2. The median dose intensity for niraparib was 94.6% in the niraparib 200 mg cohort despite 14 of 19 patients experiencing at least 1 treatment-emergent adverse event (TEAE) leading to a dose interruption or reduction. Five of 19 patients in the niraparib 200 mg plus AA-P combination arm experienced at least one TEAE leading to discontinuation of study agents – these included nausea, vomiting, increased GGT, thrombocytopenia, and congestive heart failure. A summary of dose adjustments is outlined in the table below.
Below is a summary of the pharmacokinetics of niraparib after administration of 200 mg or 300 mg in combination with AA-P:

The authors concluded with the following take-home points:
- The combination of niraparib plus APA was not considered for further development due to DLTs associated with 300 mg and drug-drug interactions resulting in reduced exposure of niraparib
- Pharmacokinetic data suggest no drug-drug interactions between niraparib and AA-P
- The recommended Phase 2 dose for niraparib was 200 mg; no patients at this dose level experienced a DLT
- Niraparib 200 mg plus AA-P was well tolerated in a dose expansion cohort
- Based on the findings from this BEDIVERE study, the efficacy and safety of niraparib plus AA-P are being evaluated in the ongoing Phase 3 MAGNITUDE Study (NCT03748461)
Presented by: Fred Saad, MD, FRCS, Professor, Chief of Urology, and Director of GU Oncology, at the University of Montreal Hospital Center (CHUM), Montreal, Quebec, Canada
Written by: Jacob Berchuck, MD, Medical Oncology Fellow at the Dana-Farber Cancer Institute (Twitter: @jberchuck), at the 2020 ASCO Genitourinary Cancers Symposium (#GU20), February 13th to 15th, 2020, San Francisco, CA.
ASCO GU 2020: The Efficacy of Two Cycles of Neoadjuvant Chemotherapy for Upper Tract Urothelial Carcinoma Patients.
- Details
San Francisco, CA (UroToday.com) Upper tract urothelial carcinoma (UTUC) is frequently upstaged after surgery and is associated with poor prognosis. There is retrospective data showing that neoadjuvant chemotherapy induced pathological downstaging and at times, pathological complete response with improved clinical outcomes. Most of these studies reported using 4 or more cycles of neoadjuvant chemotherapy. In this presented poster, the authors evaluated whether 2 cycles of neoadjuvant chemotherapy are sufficient and can improve survival of UTUC patients.
A total of 167 patients underwent radical nephroureterectomy between 2005 and 2018 and were retrospect analysed. The study population eventually included 114 patients who underwent radical nephroureterectomy who received neoadjuvant chemotherapy followed by surgery. The control group consisted of 53 patients who underwent surgery without neoadjuvant chemotherapy. The study design is shown in Figure 1 and patient characteristics are demonstrated in Table 1.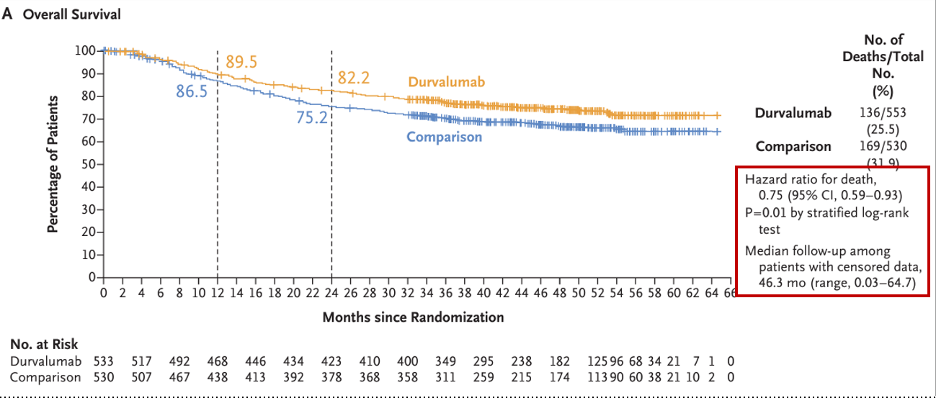
Figure 1. Study design
Table 1. Patient characteristics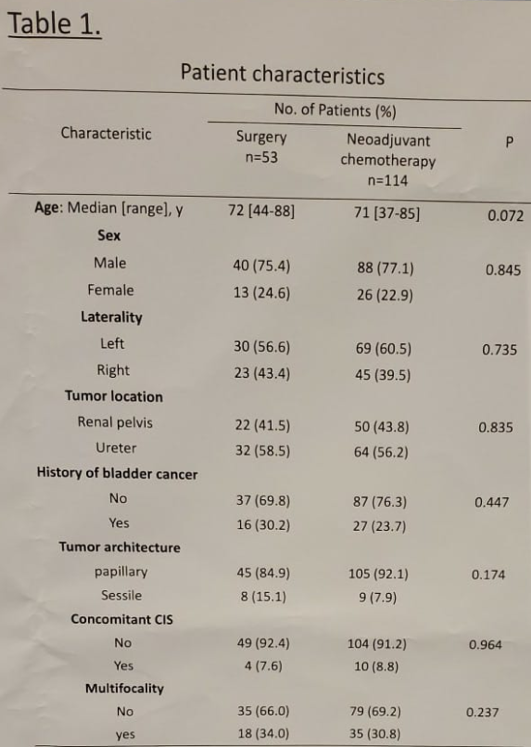
Table 2 demonstrates the clinical and pathological tumor characteristics and Table 4 shows the neoadjuvant chemotherapy regimens that were administered.
Table 2 — Clinical and Pathological Tumor Characteristics: 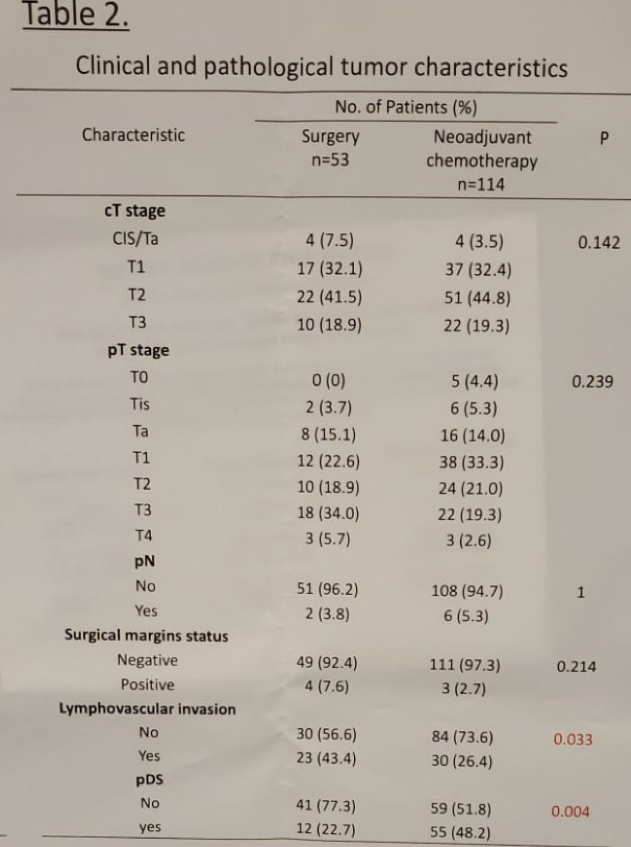
Table 4 — Neoadjuvant Chemotherapy Regimens: 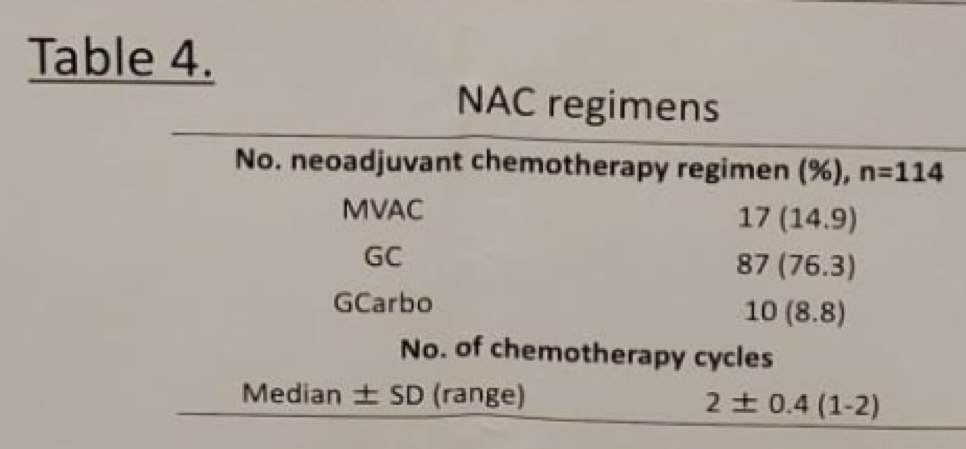
Table 5 shows the multivariable Cox model for overall survival. Figure 1-6 demonstrate the Kaplan Meier curves for overall survival (OS), cancer specific survival (CSS) and recurrence free survival (RFS).
Table 5 — Multivariable Cox Model for OS: 
Figures 1-6 — Kaplan Meier Curves for OS, CSS, RFS: 
Based on these results, the authors concluded the two cycles of neoadjuvant chemotherapy can potentially improve survival of UTUC patients. The usage of 2 instead of 4 cycles of neoadjuvant chemotherapy may offer additional clinical benefits which include low chemotherapy associated toxicity, appropriate surgery without delay in cases of chemo resistant disease, and enough cancer regression.
However, further prospective studies are needed to identify the clinical benefit of neoadjuvant chemotherapy and the optimal number of the cycles required in UTUC.
Presented by: Kenji Zennami, MD, PhD, Fujita Health University, Tokyo, Japan
Written By: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, NY, USA, Twitter: @GoldbergHanan, at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California.
ASCO GU 2020: Challenging Clinical Scenarios in the Management of Renal Cell Carcinoma - From the Perspective of a Radiologist
- Details
ASCO GU 2020: The Prevalence and Landscape of Actionable Genomic Alterations in Renal Cell Carcinoma
- Details
San Francisco, CA (UroToday.com) In parallel to the rapidly-shifting landscape of novel and combination therapies for advanced renal cell carcinoma, we have learned much about the landscape of genomic alterations that underpin this disease. Most notably from large sequencing efforts such as the Cancer Genome Atlas, and clinically-annotated cohorts such as MSK-IMPACT, our understanding of recurrent putative drivers has increased considerable in recent years. However, there has been ever increasing emphasis on study of tumor alterations that predict treatment benefit (e.g. PBRM1 alterations and immunotherapy benefit) or serve as possible actionable targets for new treatment approached. In the Renal Cell Carcinoma Rapid Abstract Session, Kyrollis Attalla, MD, from Memorial Sloan Kettering Cancer Center highlighted findings of a study describing the landscape of actionable alterations as well the corresponding evidence supporting prediction of response to therapy in renal cell carcinoma (RCC).
With this goal, the study team queried the institutional clinical sequencing database (MSK-IMPACT) to include tumor samples across all cancers. Furthermore, actionable alterations in clinical or biological evidence supporting response to targeted therapy were stratified by level of evidence using oncoKB – an oncology knowledge database.
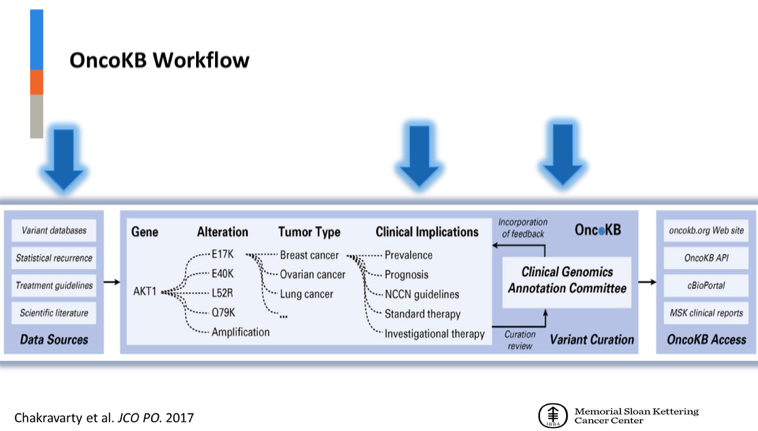
In turn, OncoKB allows for designation of therapeutic levels of evidence from 1 (FDA-recognized biomarker predictive of response to an FDA-approved drug for this indication) to 4 (compelling biological evidence supports the biomarker as predictive of response to a drug).
38,468 tumors in the MSK-IMPACT cohort were queried to refine down to 53 cases of renal cell carcinoma. 63.3% samples were from primary site and 36.% from metastases. Of the subtypes represented, clear cell was the most common (59.7%). With respect to clinical stage, most were metastatic (36.7%), 26.1% were primary lesions from patients with metastatic disease and 17% were primary lesions in non-metastatic RCC.
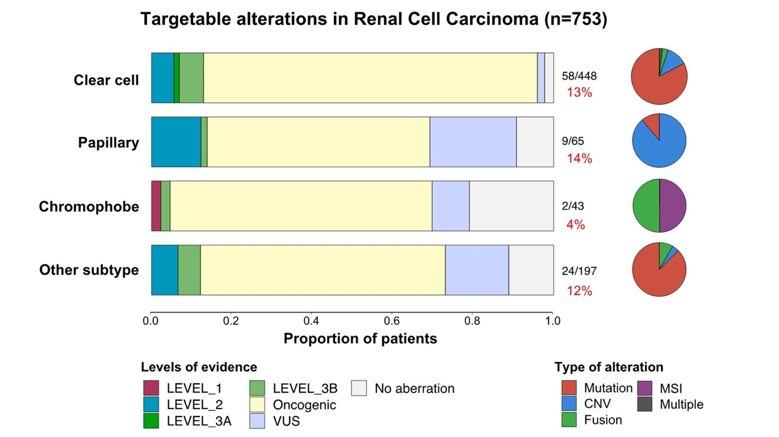
In total, there was a 12% prevalence of actionable alterations in RCC. 13% of clear cell cancer had evidence of targetable alterations. Other subtypes included papillary (14%), chromophobe (4%) and other (12%). Leading altered genes included TSC1 mutation, PIK3CA mutation and MET amplification.
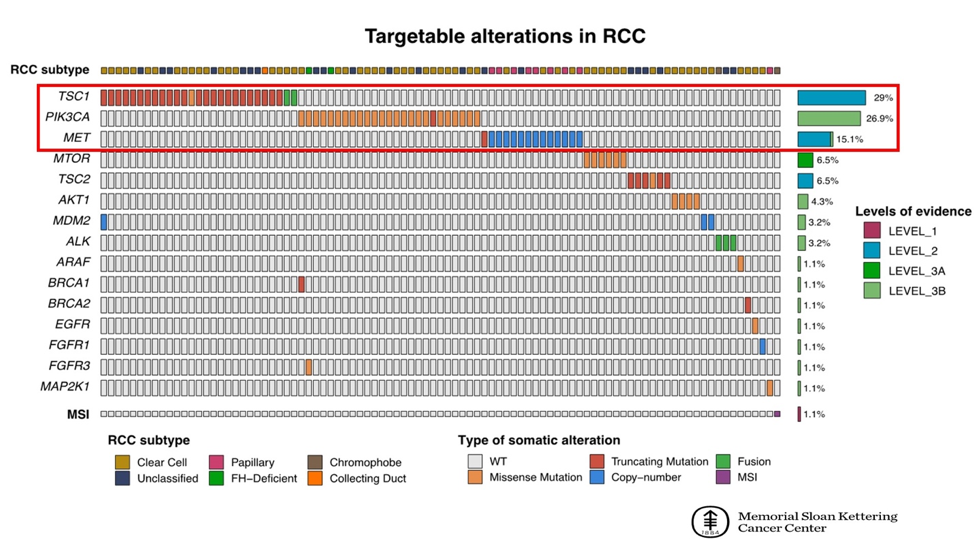
Dr. Attalla highlighted the variation of types of alterations by histologic subtype, with clear cell associated with acquired somatic mutations and papillary RCC classically associated with MET amplification. Further work is being performed to assess the clonality of alterations and validate these findings in independent cohort.
These data help establish a landscape of potentially actionable alterations in RCC and are informative for the clinical use of next-generation sequencing to inform precision treatments approaches in RCC.
Presented by: Kyrollis Attalla, MD, Urologic Oncology Fellow, Memorial Sloan Kettering Cancer Center, New York, NY
Written by: Anis Hamid, MBBS, Medical Oncology Research Fellow at Dana-Farber Cancer Institute and Medical Oncologist, PhD candidate, University of Melbourne, Australia (Twitter: @anis_a_hamid) at the 2020 ASCO Genitourinary Cancers Symposium (#ASCO # GU20), February 13th to 15th, 2020, San Francisco, CA, at the 2020 Genitourinary Cancers Symposium, ASCO GU #GU20, February 13-15, 2020, San Francisco, California.
ASCO GU 2020: A Phase I/II Study of Sitravatinib Combined with Nivolumab in Patients with Advanced Clear Cell Renal Cancer that Progressed on Prior Anti-Angiogenic Therapy
- Details
Sitravatinib is an orally-available small molecule, multi-targeted TKI. Inhibition of targets such as TAM family, Split family and c-MET is thought to enhance anti-tumor activity through depletion of immunosuppressive cell populations (for example, MDSCs and regulatory T cells) and increasing T cell priming. In a RCC expansion cohort from a phase IB trial of single-agent sitravatinib, a promising 25% conformed objective response rate was observed with 94% achieving clinical benefit and durable responses noted.
The hypothesis of this study was that sitravatinib could augment nivolumab responses in accRCC. To this end, the study’s primary endpoint was both safety and efficacy (absence of progression within 6 weeks). The patient population included a similar eligibility criteria to CheckMate 025, histologically-confirmed clear cell TCC with disease progression after 1-2 prior lines of TKI therapy and measurable disease. Dose-finding was performed using the sequentially adaptive phase I-II late-onset EffTox strategy. Of note, numerous correlative studies were built into the study design.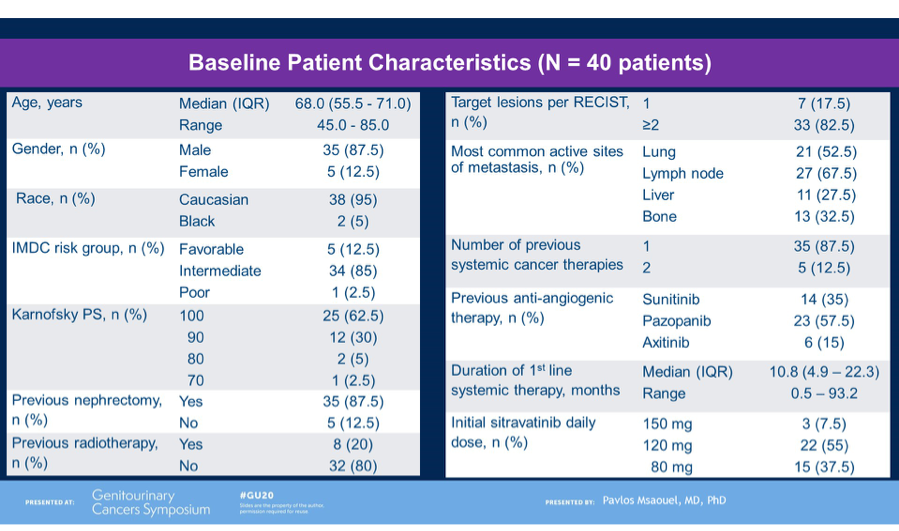
Dr. Msaouel detailed the study cohort of 40 patients, who were predominantly male and intermediate-risk for IMDC criteria. Of note, most patients had 1 prior line of cancer therapy (mostly sunitinib or pazopanib).
Nivolumab plus sitravatinib showed promising efficacy, with 15/38 (39%) achieving a confirmed objective response and 35/38 (92%) achieving clinical benefit (stable disease or partial response or completed response). Put into historical context, this is promising anti-tumor activity compared to the rate of response of single agents in this setting, such as nivolumab (35%), cabozantinib (17-21%). Furthermore, at a median follow-up of 17.7 months, median overall survival had not been reached with 79% of patients alive. Median duration of treatment (10.3m) compared favorably to historical report of nivolumab alone (4.6 months).
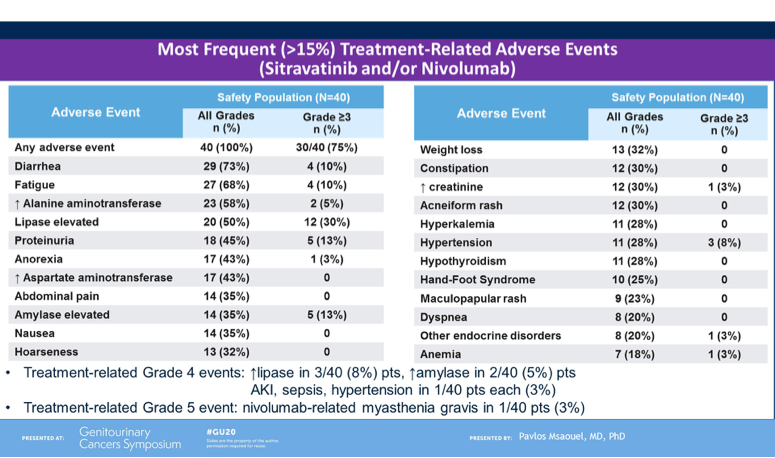
Lastly, Dr. Msaouel noted the safety profile of the combination. Most frequent adverse events included diarrhea, fatigue, liver function test derangement, lipase elevation and proteinuria. The most common high-grade toxicities included lipase/amylase elevation, proteinuria and fatigue. In total 4/40 (10%) patients discontinue treatment due to adverse events. Approximately half the cohort required dose-reduction of sitravatinib due to toxicity, and this occurred mostly in the first 12 weeks. A dose of 120mg is now being explored in other tumor types in combination with nivolumab.
In summary, this phase I/II study of sitravatinib, a multi-targeted oral TKI, in combination with nivolumab in pre-treated accRCC, showed higher objective response rate and longer PFS than historically reported single-agent nivolumab in this setting. Further studies, including patient-reported outcomes and biological correlatives are underway. This combination represents a promising strategy, however, given that PD-1 inhibition (in combination) is standard 1st-line treatment for this patient population, the role of the combination of sitravatinib plus nivolumab after progression on prior PD-1 inhibitor therapy remains less clear and more data is required.
Presented by: Pavlos Msaouel, MD, PhD, Medical Oncologist, MD Anderson Cancer Center, Houston, TX
Written by: Anis Hamid, MBBS, Medical Oncology Research Fellow at Dana-Farber Cancer Institute and Medical Oncologist, PhD candidate, University of Melbourne, Australia (Twitter: @anis_a_hamid) at the 2020 ASCO Genitourinary Cancers Symposium (#GU20), February 13th to 15th, 2020, San Francisco, CA.
ASCO GU 2020: Overall Survival Results for Durvalumab and Savolitinib in Metastatic Papillary Renal Cancer — CALYPSO trial
- Details
San Francisco, CA (UroToday.com The optimal management of advanced non-clear cell renal cell carcinoma (RCC) remains an ongoing challenge. Most of the major therapy changes in RCC in recent years have stemmed from large randomized clinical trials of advanced clear cell RCC, where combination checkpoint inhibitor (CPI) and CPI/targeted therapy approached are now firmly established in the first-line. Indeed, much of our knowledge of the treatment of non-clear cell disease is extrapolated from data in the clear cell RCC space (such as VEGF tyrosine kinase inhibition or CPI). Papillary RCC, one of the major non-clear cell subtypes, is known to harbor unique genomic features – namely MET alterations. On behalf of first author Cristina Suarez Rodriguez, MD, Thomas Powles, MBBS, presented the results of the papillary RCC arm of CALYPSO, a study of durvalumab plus savolitinib in metastatic RCC.
Durvalumab (a PD-L1 inhibitor) and savolitinib (a small molecular MET tyrosine kinase inhibitor) both hold strong rationale for the treatment of advanced papillary RCC. The papillary cohort of CALYPSO enrolled patients who were either VEGF tyrosine kinase inhibitor naïve or refractory. All patients received savolitinib 600mg daily and durvalumab 1500mg commencing on day 29. Treatment was continued until progression or loss of clinical benefit. The primary endpoint of the trial was objective response rate. Secondary endpoints included progression-free survival (PFS), overall survival (OS), duration of response and safety.
In total, 41 patients were enrolled and received treatment and the results presented by Dr Powles was after a cohort median follow-up of 14.3 months. Median age of patients was 62 years, with 29%, 62% and 7% categorized as good, intermediate and poor risk per IMD criteria, respectively. 85% had prior nephrectomy and 66% had not received any prior systemic anti-cancer therapy. 24% had received one previous line of therapy.
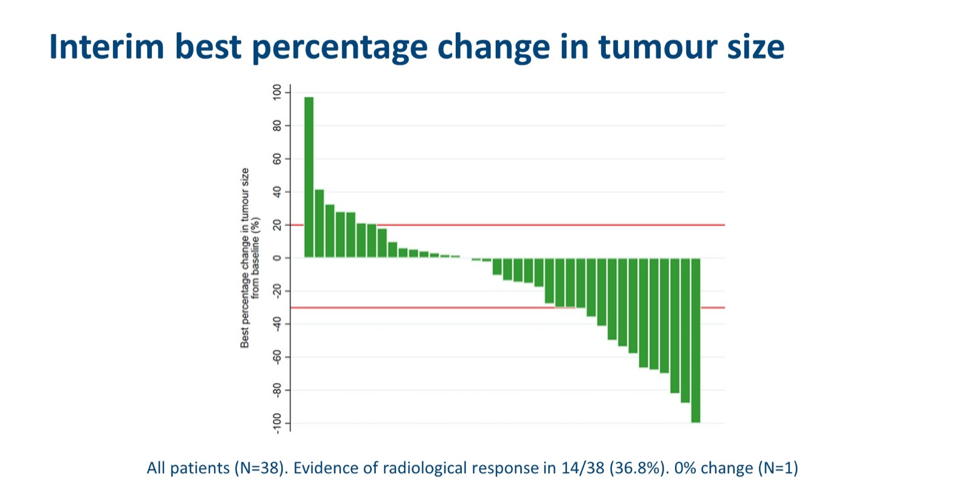
With respect to the primary endpoint, 11 (27%) patients had a confirmed objective response to therapy. The response rates in PD-L1+ and MET+ subgroups were 25% and 40%, respectively. In treatment-naïve patients, a 33% response rate was observed. In total, there was evidence of radiological response in 14/38 (36.8%) patients.
Interim PFS and OS results were presented. The median PSA was 4.9 months, with a 12-months PFS rate of 31.3% overall, 28.6% in PD-L1+ subgroup and 30.5% in MET+ subgroup. The median OS was 12.3 months, with a 12-month OS rate of 52.1% overall, 50% in PD-L1 subgroup and 45.7% in MET+ subgroup. Put together, these data indicate that neither PD-L1 nor MET expression were associated with different PFS and OS compared to the overall cohort.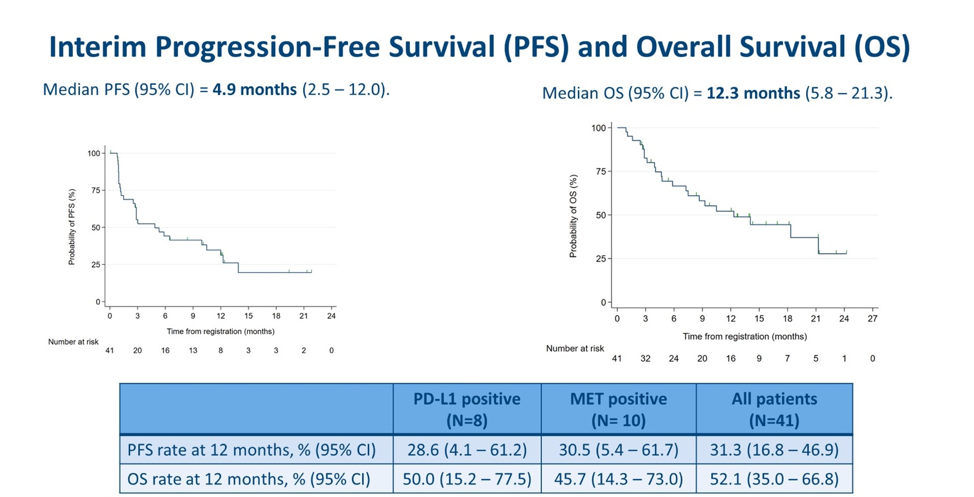
Several durable responses greater than 6-9 months were observed and notably, were seen in PD-L1+, MET+ and PD-L1-/MET- subgroups, suggesting these do not appear to be discriminatory biomarkers with respect to durable response, as with progression and survival time.
To conclude, Dr Powles noted that CALYPSO is the first trial of CPI with MET-targeted therapy in papillary RCC and the results presented are encouraging, in particular the overall response rate, PFS and OS compared to historical studies in this patient population and stage of therapy exposure. He noted that long responses were observed in a subset of patients, however a biomarker has not been identified in this setting. Though safety data was not shown during this presentation, Dr Powles noted that tolerability remained within expectation of the combination and there are plans to extend the study to further explore his promising combination treatment for papillary RCC.
Presented by: Thomas Powles, MBBS, Professor of Genitourinary Oncology and Lead for Solid Tumor Research at Barts Cancer Institute, Director of Barts Cancer Centre, London, United Kingdom
Written by: Anis Hamid, MBBS, Medical Oncology Research Fellow at Dana-Farber Cancer Institute and Medical Oncologist, PhD candidate, University of Melbourne, Australia, Twitter: @anis_a_hamid, at the 2020 ASCO Genitourinary Cancers Symposium (#GU20), February 13th to 15th, 2020, San Francisco, CA.
ASCO GU 2020: Phase II Study of Cabazitaxel plus Enzalutamide in Metastatic Castration-Resistant Prostate Cancer
- Details
San Francisco, CA (UroToday.com) Chemo-hormonal therapy has shown positive results in both the STAMPEDE and CHAARTED clinical trials and is now used for metastatic castrate sensitive prostate cancer. To date, there is no indication to combine any of the therapies currently available for castration resistant prostate cancer.
ASCO GU 2020: Novel Drugs for Clear Cell Renal Cell Carcinoma
- Details
San Francisco, CA (UroToday.com) The first two studies presented in the Renal Cell Carcinoma (RCC) Oral Abstract Session at ASCO GU 2020 were a clear introduction to the theme of novel therapies and combinations for clear cell RCC. In his discussion, Daniel Geynisman, MD, from Fox Chase Cancer Center summarized the “30,000 foot view” of advanced clear cell RCC (accRCC) — putting the abstracts of Toni K. Choueiri, MD, (Abstract 611) and Pavlos Msaouel, MD, PhD (Abstract 612) in context for clinicians and patients.
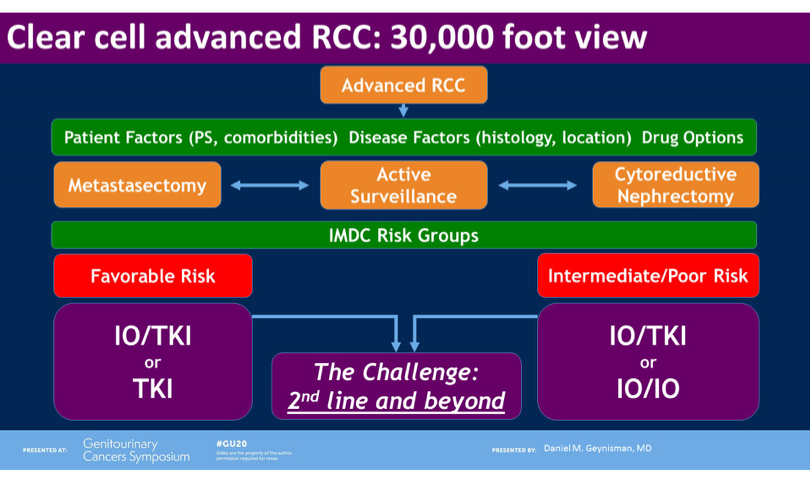
Firstly, it was noted that the therapy landscape of accRCC has rapidly changed in recent years on the back of the shift of first-line therapy to ipilimumab plus nivolumab or pembrolizumab plus axitinib, on the basis of large randomized phase II studies. This in turn has highlighted an ever-present challenge: the optimal therapy for 2nd-line and beyond. Indeed there are several existing options in this setting, most notably including nivolumab, cabozantinib and lenvatinib/everolimus. Focusing on 2nd-line nivolumab specifically, Dr. Geynisman highlighted the rationale of improving responses and time to progression of patients who had previously received a tyrosine kinase inhibitor (TKI).
Reviewing Abstract 612, a phase I/II study of sitravatinib combined with nivolumab in patients with accRCC that progressed on prior anti-angiogenic therapy, it was noted that the biological rationale of sitravatinib was to ultimately sensitize tumors to checkpoint inhibitor therapy with nivolumab. Sitravatinib is an orally-available small molecule, multi-targeted TKI. Inhibition of targets such as TAM family, Split family and c-MET is thought to enhance anti-tumor activity through depletion of immunosuppressive cell populations (for example, MDSCs and regulatory T cells) and increasing T cell priming.
The overall response rate (ORR) of 39% and disease-control rate of 92% for sitravatinib plus nivolumab was noted as very promising, and the progression-free survival of 10.3 months prolonged compared to historical studies of 2nd-line therapy for accRCC. Dr. Geynisman noted, however, that that it is unclear whether the tumor microenvironment is being modulated or whether the combinations may be merely active due to patients being previously untreated with an immune checkpoint inhibitor. The combination was noted to be safe and in need of further follow-up. Furthermore, he highlighted the need for data in patients previously treated with an immune checkpoint inhibitor given this is at the frontline of therapy for accRCC in 2020.
Abstract 611, a phase I/II study of the oral HIF-2 α inhibitor MK-6482 in patients with accRCC, was then discussed with a note on the Nobel Prize-winning effort to understand tumor hypoxia that has led to development of HIF inhibitors. It was noted that in this study population, 67% of patients had received both anti-PD1 and anti-VEGF therapies, and most were intermediate- or poor-risk per IMDC criteria. Dr. Geynisman noted the very promising efficacy data in this heavily-treated cohort, with 69% showing some degree of tumor shrinkage, a 24% overall response rate and 80% disease-control rate. These findings seem to be consistent in prior phase I and phase II studies of HIF-2a inhibitors across over 100 patients.
Furthermore, the toxicity profile of MK-6482 was very favorable with only 2/55 discontinuing therapy due to treatment-related adverse events. Generally, the cases of anemia and hypoxia observed were low-grade in nature. MK-6482 appears to not be associated with many of the adverse effects typically observed with VEGF TKI therapy.

In summarizing, Dr. Geynisman noted that given the encouraging safety and efficacy data, a phase II randomized trial of MK-6482 versus everolimus for accRCC is underway, including patients have not received more than 3 lines of prior therapy. Results are eagerly awaited.
Presented by: Daniel M. Geynisman, MD, Medical Oncologist, Fox Chase Cancer Center, Philadelphia, PA
Written by: Anis Hamid, MBBS, Medical Oncology Research Fellow at Dana-Farber Cancer Institute and Medical Oncologist, PhD candidate, University of Melbourne, Australia (Twitter: @anis_a_hamid) at the 2020 ASCO Genitourinary Cancers Symposium (#ASCO # GU20), February 13th to 15th, 2020, San Francisco, CA