The incidence of metastatic prostate cancer at diagnosis ranges from ~5-50%, with significant geographic differences as previously described.2 Such patients are defined as having de novo or synchronous mHSPC. Additionally, there exits a subset of men initially diagnosed with non-metastatic disease, many of whom have received prior definitive local treatment, who will have progression to a metastatic state prior to development of castration resistance. This is known as metachronous mHSPC. This distinction between synchronous (i.e. de novo) and metachronous presentations is of utmost clinical importance given the known differences in underlying genomic mutational profiles and prognoses, influencing the subsequent choice of treatment intensification.3,4 These two cohorts can be further subdivided based on the volume of metastatic disease at presentation: low and high volumes. The CHAARTED high-volume criteria have been widely adopted in clinical practice, with high volume patients defined as follows: presence of visceral metastases or ≥4 bone lesions with ≥1 beyond the vertebral bodies and pelvis.5
As such four distinct subgroups become clinically relevant (median overall survival per CHAARTED and GETUG-15 among men receiving ADT alone, ie. the control groups in these trials):
- Synchronous and high volume: 3 years
- Synchronous and low volume: 4.5 year
- Metachronous and high volume: 4.5 years
- Metachronous and low volume: ~8 years
Index Patient 3: Metachronous High Volume mHSPC
Case Presentation: A 65-year-old previously healthy male with an ECOG performance status of 1 presents to his urologist to re-establish care for his prostate cancer. The patient had been previously diagnosed with prostate cancer Gleason Score 8 (4+4) in 4/16 cores five years prior and had received conventionally fractionated external beam radiotherapy with concurrent androgen deprivation therapy for 18 months. At the time of diagnosis, staging work up with conventional imaging (CT abdomen/pelvis and bone scan) were both negative, and his serum PSA had nadired from 7.90 ng/ml to 0.86 ng/ml. The patient was subsequently lost to follow-up as he had moved across the country and had lost his insurance coverage. At the time of re-presenting, the patient was found to have a PSA of 48.1 and was complaining of mid/lower back pain. A staging work up with a CT and bone scan demonstrated evidence of three lumbar (L2-L4) and a left femoral osteoblastic lesion. The remaining work up demonstrated evidence of anemia (Hgb: 10.1 g/dL), otherwise unremarkable.Doublet Therapy: ARAT + ADT
When considering patients with mHSPC along a risk continuum, from good risk (metachronous low volume: 8-year median overall survival with ADT alone) to poor risk (synchronous high volume: 3-year median overall survival with ADT alone), patients with synchronous low volume and metachronous high volume (median overall survival: 4.5 years with ADT alone) mHSPC may both be considered as intermediate risk disease. As such, the clinical treatment approach for these two subgroups has significant overlap - ARATs + ADT have similarly served as the backbone for treatment of these patients. Patients with metachronous, high volume mHSPC have historically accounted for only a small proportion of patients in the published phase III trials, and as such, post-hoc analyses have been underpowered for evaluating this subgroup. Results from the ARCHES trial have demonstrated a 23% decreased hazard of overall mortality in this subgroup with addition of enzalutamide to ADT (HR: 0.77; 95% CI: 0.39 to 1.50).12
Doublet Therapy: Docetaxel + ADT
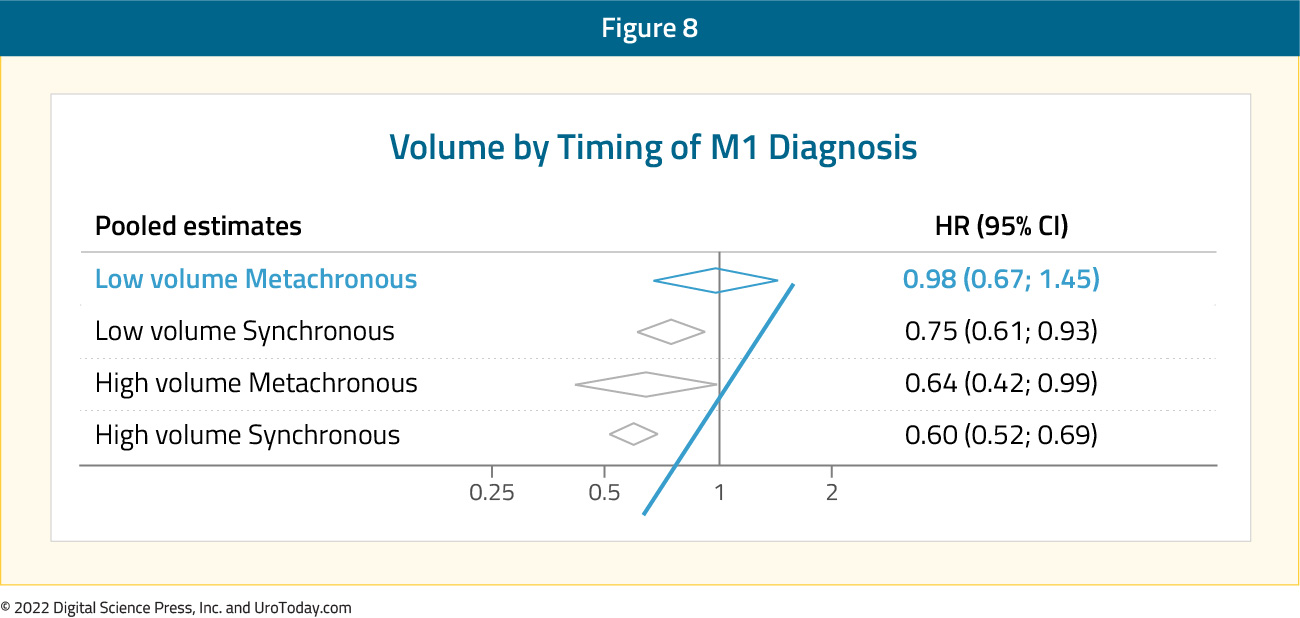
Results from the STOPCAP M1 collaborative meta-analysis of individual patient data from GETUG-15, STAMPEDE, and CHAARTED demonstrated that docetaxel addition to ADT in patients with metachronous, high volume prostate cancer is associated with significant improvements in overall survival (HR: 0.64, 95% CI: 0.42 to 0.99).
Triplet Therapy: Docetaxel + ARAT + ADT
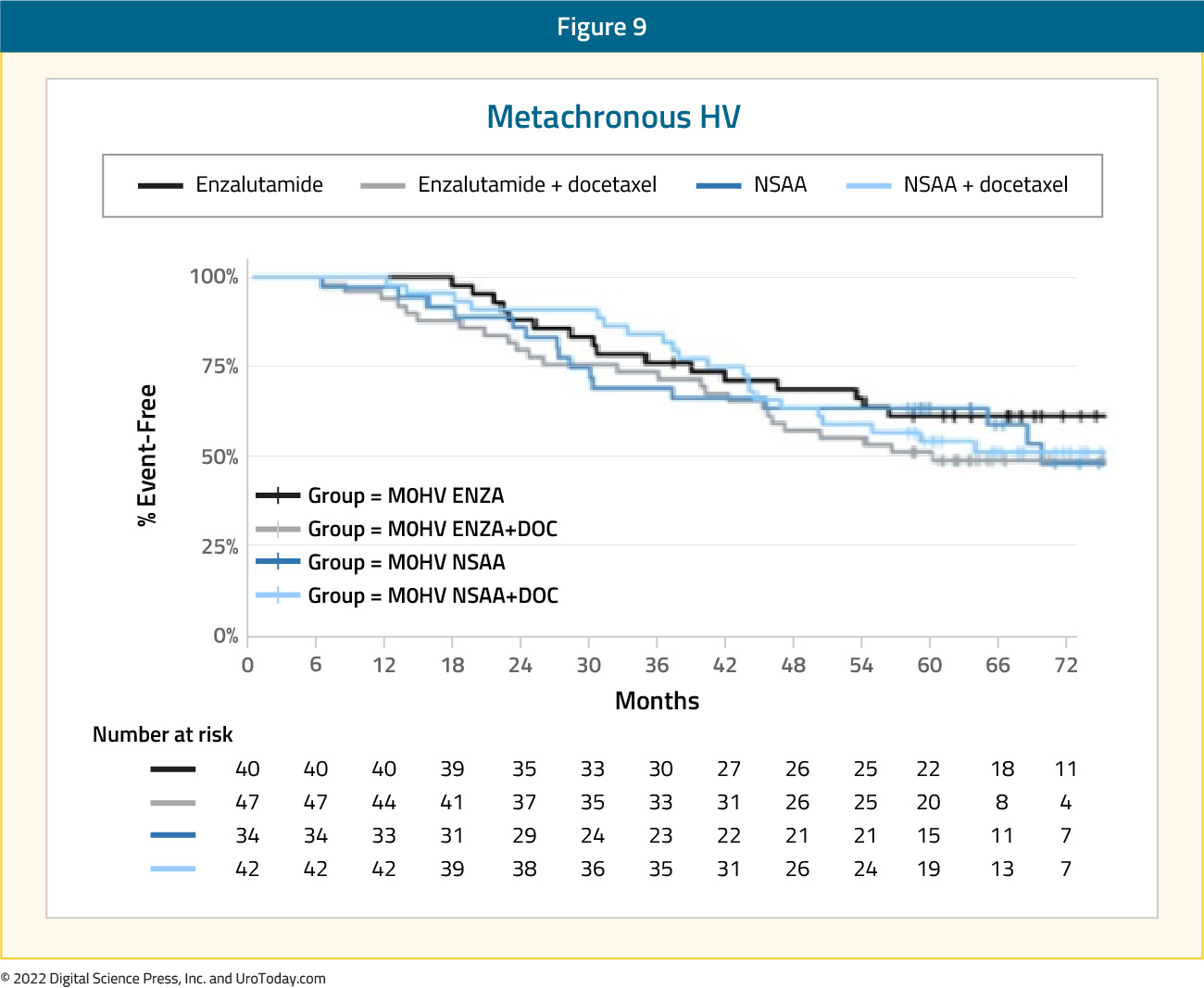
Do these patients benefit from further treatment intensification with both docetaxel and an ARAT? Given that the PEACE-1 trial included patients with de novo mHSPC only, and ARASENS, to date, has no subgroup analyses by CHAARTED risk group criteria, the only available data to assess the benefit of triplet therapy in this mHSPC subgroup is from the ENZAMET updated analysis presented at ASCO 2022. As demonstrated in the Kaplan Meier analysis below, there does not appear to be a benefit to treatment intensification with both docetaxel and ARAT in this subgroup.
Given the relative increased toxicity with taxanes, along with a subset of patients being “chemotherapy unfit”, it appears that doublet therapy with an ARAT + ADT is the favored treatment approach in patients with metachronous high volume disease, with docetaxel reserved for select patients with higher volume of disease.
Written by:
- Rashid K. Sayyid, MD, MSc, University of Toronto, Toronto, Ontario
- Zachary Klaassen, MD, MSc, Medical College of Georgia, Augusta, Georgia, USA