Introduction
Immune checkpoint inhibitors have emerged as a guideline-recommended first line treatment option for patients with cisplatin-ineligible, metastatic urothelial carcinoma of the bladder and as second line therapy for patients with metastatic disease progressing during, or after, platinum-based combination chemotherapy.1 Pembrolizumab, a Programmed Death-1 (PD-1) inhibitor, has been recently approved by the US Food and Drug Administration for the treatment of patients with Bacillus Calmette Guerin (BCG)-resistant non-muscle invasive bladder cancer (NMIBC), based on the results of the KEYNOTE-057 trial.2,3
Given that patients with NMIBC receiving adjuvant BCG post-TURBT have estimated risks of disease recurrence and progression of 40% and 10%, respectively,4 the BCG naïve NMIBC space may provide an opportunity to move these agents up even further along the bladder cancer disease spectrum. In this Center of Excellence article, we will summarize the current state of the evidence for ongoing trials evaluating immune check point inhibitors and other immune priming interventions in combination with BCG for the treatment of BCG naïve NMIBC.
Pembrolizumab + BCG
Previous studies have demonstrated that programmed cell death ligand 1 (PD-L1) expression is significantly increased in BCG-induced bladder granulomata of patients with BCG unresponsive disease.5 As such, it has been hypothesized that the addition of a PD-1 inhibitor, such as pembrolizumab, may overcome this potential underlying mechanism of resistance.
The combination of pembrolizumab + BCG has previously been evaluated in the setting of a phase I trial for patients with BCG unresponsive NMIBC. This combination was determined to be relatively safe, and the 13 evaluable patients had a 3-month complete response rate of 69%.6
KEYNOTE-676 is a randomized, comparator-controlled trial evaluating the efficacy and safety of pembrolizumab + BCG in patients with high-risk NMIBC (T1, CIS, high grade Ta) who underwent cystoscopy/transurethral resection of bladder tumor ≤12 weeks before randomization and had not received BCG within the preceding two years. Patients will be randomly assigned 1:1:1 to receive:
- Pembrolizumab 400 mg IV every 6 weeks + BCG reduced maintenance (≤ 6 months)
- Pembrolizumab 400 mg IV every 6 weeks + BCG full maintenance (≤ 18 months)
- BCG monotherapy with BCG full maintenance
The trial schema for KEYNOTE-676 cohort B is as follows:
The primary endpoint for this trial is event-free survival, defined as the time from random assignment to the first occurrence of any of the following:
- High-grade Ta, CIS, or any T1 disease of the bladder
- High-risk disease (high-grade Ta, CIS, or ≥T1) of the urethra or upper tract
- Locally advanced/metastatic disease determined by blinded independent central review
- Death from any cause
The secondary endpoints will include complete response rate by blinded independent central review, duration of response, disease-specific survival, time to cystectomy, overall survival, and safety.7 As follows is a geographical representation of the countries currently enrolling patients in KEYNOTE-676:
Additionally, a single arm, phase II trial (NCT03504163) from the Memorial Sloan Kettering Cancer Center is evaluating the combination of BCG + pembrolizumab in patients with high-risk T1 bladder cancer, with an additional exploratory cohort of patients with upper tract disease. This study will plan to enroll 37 patients, who will receive pembrolizumab 400 mg IV at 6-week intervals (total 9 doses), with BCG (TICE strain, 50 mg) administered once weekly for 6 weeks as induction, followed by maintenance consistent with standard clinical practice. BCG will be started on week 3 after the first infusion of pembrolizumab to allow for the initial priming of T cells to further enhance the effects of BCG treatment. The primary outcome is the proportion of patients who remain free of high-grade disease recurrences at 6 months post-treatment initiation.8
Atezolizumab + BCG
BladderGATEBladderGATE (NCT04134000) is a phase Ib-II trial evaluating the safety and efficacy of atezolizumab (anti-PD-L1) + BCG in patients with high-risk NMIBC, who are either BCG-naïve or had not received BCG in the preceding two years. Patients in this trial will receive either:
- Induction BCG with 1 instillation every week + IV atezolizumab 1,200 mg every 3 weeks (Dose level 0)
- Induction BCG with ½ instillation every week + IV atezolizumab 1,200 mg every 3 weeks (Dose level -1)
Following induction, BCG will be administered at weeks 13-15, 25-27, and 49-51, with atezolizumab concurrently administered for up to 1 year. Patients were accrued to each dose level in cohorts of 10 patients until the maximum tolerated dose is achieved (dose at which < 4 out of 10 patients experience dose-limiting toxicity). The interim safety results were recently presented at ASCO 2023. This analysis included 34 patients, with no dose-limiting toxicities reported in the first 10 patients included at dose level 0. The most frequent grade 3-4 adverse events were:
- Asthenia (9%)
- Myocarditis (3%)
- Immune-mediated hepatitis (3%)
- Hyponatremia (3%)
- Encephalopathy (3%)
- Guillain-Barre syndrome (3%)
Two patients discontinued the study treatment due to immune-mediated Grade 3 hepatitis and pneumonitis, respectively.9
ALBANALBAN (AFU-GETUG 37; NCT03799835) is a phase III trial across 30 centers in France evaluating the efficacy and safety of atezolizumab given in combination with BCG versus BCG alone in patients with BCG naïve, high-risk NMIBC (T1, high-grade, and/or CIS). Eligible patients will be randomized 1:1 to:
- Arm A: BCG alone with six weeks induction followed by three weekly maintenance instillations at 3, 6, and 12 months
- Arm B: BCG + atezolizumab (1,200 mg IV every 3 weeks for up to 1 year)
The primary endpoint is recurrence-free survival in the intent-to-treat population, with secondary efficacy endpoints of overall survival, progression-free survival, complete response, disease worsening, quality of life, and safety outcomes. Study enrollment began in December 2018 with a target of 614 patients.10
Durvalumab + BCG
POTOMAC (NCT03528694) is an open label, multicenter, randomized trial evaluating the combination of durvalumab (anti-PD-L1) and BCG in BCG-naïve patients with high-risk NMIBC (any high-grade disease, T1, CIS, LG Ta if >3 cm, recurrent, and multifocal). This trial will randomize 1,018 patients to:
- BCG induction + maintenance for 24 months
- BCG induction + maintenance + durvalumab (1,500 mg every 4 weeks for 13 cycles)
- BCG induction only (no maintenance) + durvalumab
The study design is as follows: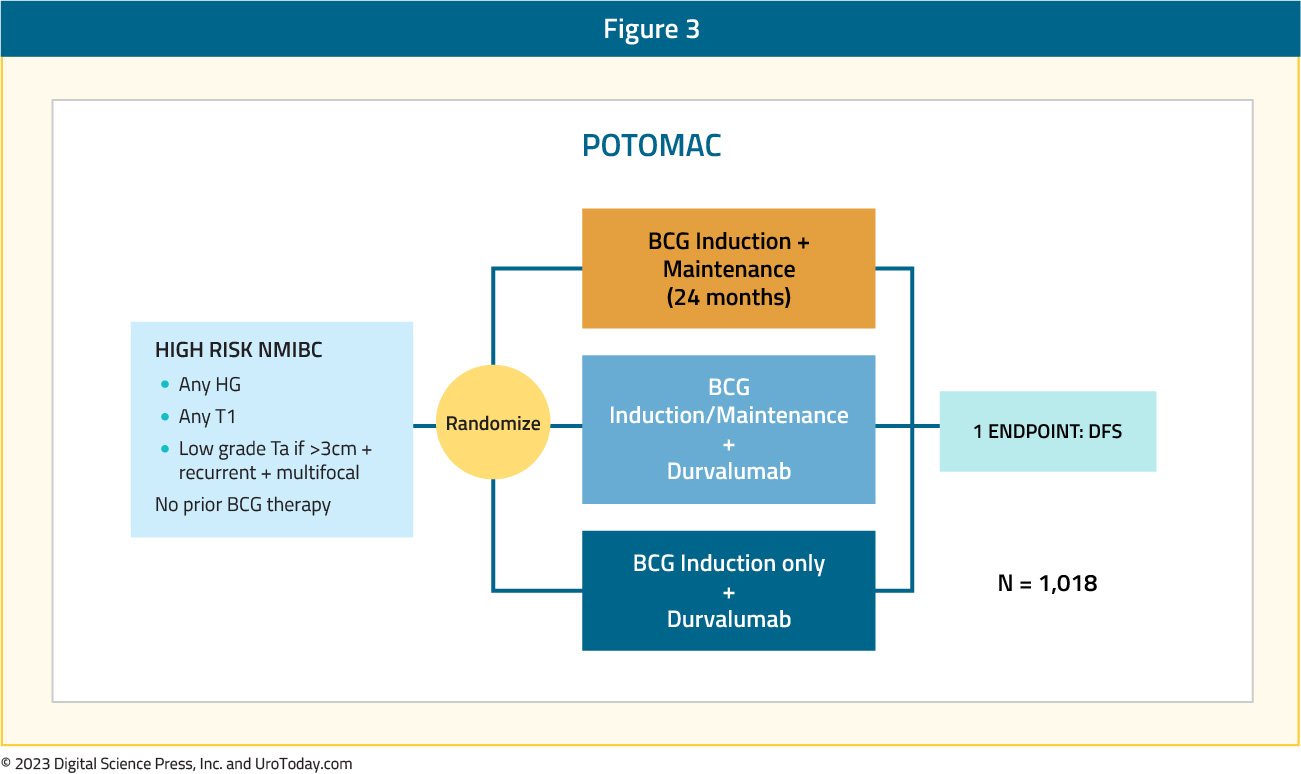
The primary study endpoint is disease-free survival, with secondary endpoints including the proportion of patients alive and disease-free at 24 months, 5-year overall survival, pharmacokinetics, immunogenicity, safety, tolerability, and health-related quality of life.11
Sasanlimab + BCG
Sasanlimab is an anti-PD-1 monoclonal antibody that has demonstrated an acceptable safety profile and promising clinical activity in patients with locally advanced or metastatic urothelial carcinoma, within the context of a phase 1 trial.12 The phase 3 CREST study (NCT04165317) Cohort A will evaluate subcutaneous injection sasanlimab in patients with BCG naive NMIBC. Patients in this cohort will be randomized to one of three arms:
- Arm A: Sasanlimab + BCG induction + maintenance
- Arm B: Sasanlimab + BCG induction only
- Arm C: BCG induction + maintenance
This trial will assess for between-arm differences in event-free, disease-specific, and overall survivals, complete response rate, adverse events/safety profile, and health-related quality of life.13 Of note, On August 31, 2022, the Sponsor announced the discontinuation of enrollment to Part B (Cohort B), which enrolled participants with BCG unresponsive NMIBC. The decision to discontinue enrollment to Part B (Cohort B) was not made for safety reasons.14
Immune Priming: Intradermal BCG
The PRIME trial (SWOG S1612) is evaluating whether intradermal BCG inoculation may potentiate the immune effects of subsequent intravesical BCG instillations. This hypothesis was recently tested in a single arm trial that demonstrated that percutaneous BCG administered 21 days prior to intravesical instillation in patients with high-risk NMIBC boosted BCG-specific immunity at 3 months and increased the activation status of in vitro expanded circulating NK and γδ T cells and their cytotoxicity against bladder cancer cells.15
In the PRIME trial, the Tokyo BCG strain is being used for both intradermal inoculation and intravesical instillation in a three-arm design with TICE strain BCG also used as a standard of care comparator. This study was designed to test:
- The comparitive superiority between intravesical Tokyo strain BCG when combined with intradermal inoculation as compared to intravesical alone (arms 2 and 3)
- The non-inferiority of intravesical Toyko strain alone to intravesical TICE strain (arms 1 and 2).
- TICE strain is currently the only strain that is FDA approved and in production in the USA (Armond-Frappier and Connaught are also FDA approved, but not currently in production). As such, if the Tokyo strain is found to be non-inferior to TICE, this may facilitate its subsequent FDA approval and increased the availability of additional BCG strains during the current shortage
The study design is as follows:
This trial has now fully accrued and is awaiting readout in the nearby future.
Conclusions
Numerous ongoing trials are evaluating the combination of BCG and an immune checkpoint inhibitor for patients with BCG naïve NMIBC. By inhibiting the PD-1/PD-L1 axis, it is hypothesized that these agents may help overcome underlying mechanisms of resistance inherent to BCG-resistant strains, and thus improve on the historic recurrence and progression rates observed with BCG treatment alone. Many of these trials have completed accrual, and we await the results of these combinatory trials in the upcoming years.