Endoscopic Surgical Management
Cystoscopic ResectionNMIBC is usually diagnosed with cystoscopic evaluation. Upon diagnosis, the location, number, and morphology of the tumors are recorded. Urinary cytology is sent and upper tract imaging performed to assess for extravesical urothelial tumors and staging purposes.
Transurethral resection of bladder tumor (TURBT) is the initial treatment. Bimanual exam under anesthesia should be performed to complete clinical staging. It is imperative that deeper resections are obtained to ensure adequate muscle sampling and en bloc resection or at least sending the base separately can help pathologists make the best diagnosis. Resecting tumors within a bladder diverticulum may be easily complicated by bladder perforation. Invasion beyond the lamina propria in diverticula should be categorized as cT3a disease. When resecting near the ureteral orifice caution is advised and using pure cutting current is important to minimize scarring which may lead to ureteral obstruction. Alternatively, small tumors may be resected using the cold-cup biopsy forceps.
To improve the quality of TUR and reporting, a 10-item checklist designed to encompass both the description of tumor characteristics associated with oncologic outcomes (e.g. tumor number, size, and characteristics) and steps ensuring adequate tumor evaluation and treatment (e.g. bimanual exam, visually complete resection) has been proposed. The implementation of this checklist enhanced surgeon attention to the critical aspects of the procedure, improving surgical quality.1
Expected side effects of TURBT include minor bleeding and irritative symptoms. Excessive bleeding and bladder perforation are uncommon (<5% of cases). Fortunately, in cases of perforation, the risk of tumor seeding appears to be low.2 Extraperitoneal perforations can usually be managed with prolonged catheterization, while intraperitoneal rupture often requires surgical repair. TUR syndrome may occur due to the absorption of hypotonic fluid if due diligence is not observed.3 As long as minimal energy is applied to the ureteral orifice, the incidence of scarring is low.4
Additional Strategies
Concurrent with resection of the tumor, any suspicious area within the lower urinary tract should be sampled, either with formal resection or with cold cup biopsy. Prostatic urethral biopsies are recommended in patients with a multifocal tumor or visible abnormalities. Repeat TUR within 2-4 weeks is recommended when primary resection is incomplete or in the presence of high-grade T1 tumors.5
Laser therapy is sometimes used, not only for tumor coagulation but also for en bloc resection. In a recent meta-analysis of en bloc resection series, 96% of the cases demonstrated the presence of detrusor muscle within the specimen and residual disease was present on re-TUR in only 1/119 cases.6 Treatment should be under direct visualization and discontinued as soon as a coagulative effect is observed around the tumor base.7
Narrowband imaging (NBI) and blue light cystoscopy (BLC) has been used to enhance visualization of bladder tumors. BLC is a technique that identifies cancer through the selective accumulation of photosensitizing drugs (5-aminolevulinic acid and hexyl-aminolevulinate) in the malignant cells. When used in conjunction with white light cystoscopy, BLC provides enhanced detection rates of non-muscle invasive lesions.8-10 In a meta-analysis consisting of 12 randomized controlled trials with a total 2258 patients, a lower recurrence rate (OR 0.5; p<0.0001) with a delayed time to the first occurrence (by 7.39 weeks, p<0.0001) was seen with BLC.11 As a result, recommendations for its use have been incorporated into the NCCN guidelines. Recently, flexible blue light cystoscopy was also demonstrated to detect additional malignant lesions in 63% of the patients with recurrence after primary therapy and in 21% of the patients with lesions not otherwise seen on white light cystoscopy.12
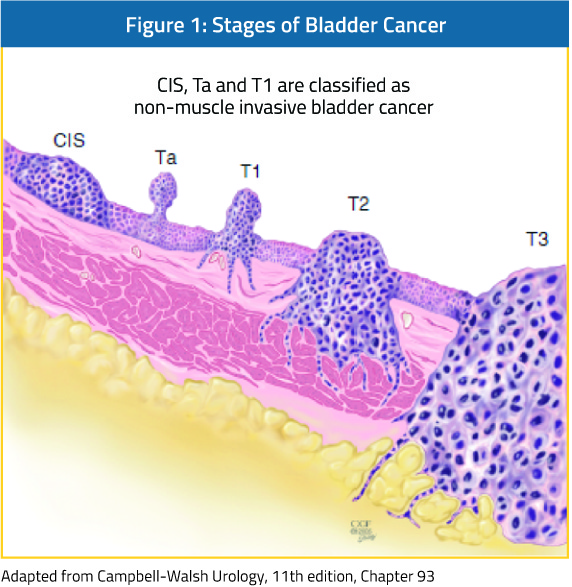
In NMIBC, the most important prognostic factor for progression is grade.13 While high-grade tumors often appear sessile and broad-based, low-grade tumors typically exhibit papillary architecture on a thin stalk. In conjunction, LG tumors’ low likelihood of progression and favorable morphology lend themselves to biopsy and fulgurations that can be accomplished in the outpatient setting.14 Adopting this strategy can significantly reduce the therapeutic burden associated with bladder cancer treatment.
Perioperative Intravesical Chemotherapy
The most widely studied agent has been Mitomycin C (MMC), used as a single dose immediately after TURBT. Although MMC was shown to reduce the risk of recurrence by 35% (HR: 0.65; 95% CI, 0.58-0.74; p<0.001), it was not efficacious in patients with a prior recurrence rate of more than one per year or in patients with EORTC recurrence score 5.15 A recent prospective randomized trial using perioperative infusion of gemcitabine demonstrated a reduction of recurrence from 47% to 35% (p<0.001). Corroborating the findings in a previous meta-analysis of perioperative instillation of Mitomycin C, among the target population with low-grade, non-muscle invasive cancer, the reduction was even more dramatic (from 54% to 34%, p-0.001). There were also minimal complications (2.4% ≥Grade 3).16Adjuvant Intravesical Therapy
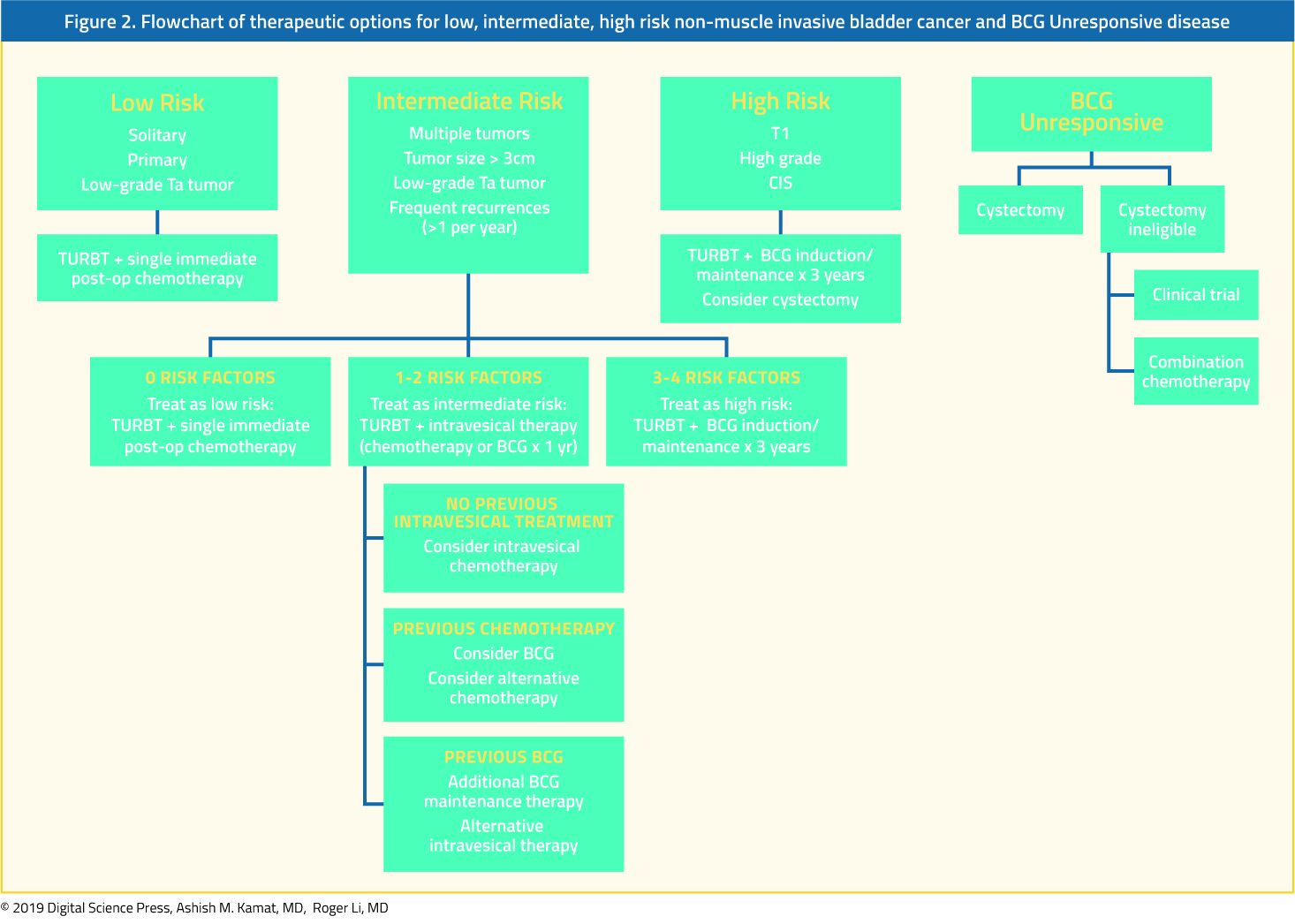
ImmunotherapyBacillus Calmette-Guerin is an attenuated mycobacterium with proven efficacy in reducing recurrences, progression and death from  NMIBC.17 Therapy is usually started 2-4 weeks after tumor resection.18 Therapeutic protocol includes induction with 6 weeks followed by maintenance therapy (3 weekly maintenances at 3mo, 6mo, 12mo, 18mo, 24mo, 30mo, and 36mo). This is now accepted as standard of care in patients with high-risk disease, with one year maintenance as an alternative for intermediate risk patients (Figure 2).19 If tumor recurrence is found after induction therapy, an additional induction course may be attempted.
Although side-effects are usually temporary and self-limited, significant morbidity can occur with fevers, lung infections, and sepsis. While most can be treated with symptomatic therapy, in the case of severe infections or BCG-osis, addition of steroids should be considered in addition to anti-tuberculosis therapy. In a randomized study by the EORTC, reduced dose was compared to full dose BCG, and 1 compared to 3 years. While full dose for 3 years was associated with the best reduction in recurrences, there was no significant difference with regards to progression.20 Interestingly, there was no difference in local or systemic side effects between low dose or full dose BCG.20 Â Nonetheless in clinical practice, reduction of dose for cause - i.e. when side effects are reported - Â has been noted to allow patients to continue on therapy and finish the duration of maintenance.
A number of other immunogenic agents have been tested for the treatment of NMIBC, some in the setting of BCG failure. These include keyhole limpet hemocyanin (KLH), mycobacterial cell wall DNA extract (MCNA), IL-2, and IFN-α. None of these, however, proved to be as effective as treatment with BCG.
Chemotherapy
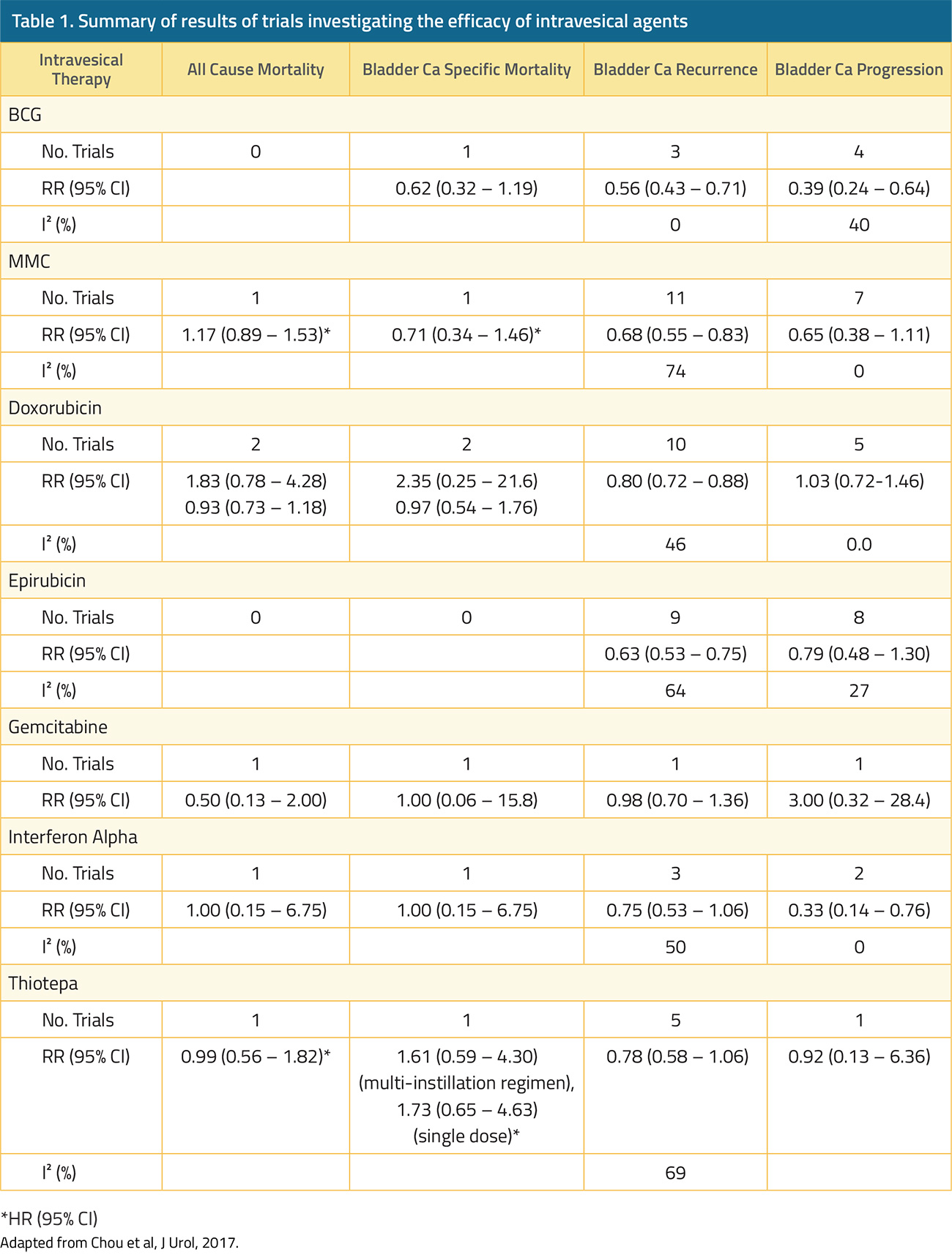
In general, intravesical chemotherapy may improve recurrence-free rates, but these are not as effective as BCG in preventing progression (Table 1). They are, however, better tolerated. MMC, the most extensively studied intravesical chemotherapy agent, was associated with 9. 4% progression rate, compared to 7.7% after BCG.21 Â Strategies such as electromotive therapy have been seeking to enhance the efficacy of MMC, although results have been mixed thus far. In studies limited to high-risk NMIBC, recurrence-free rates following chemohyperthermia ranged from 29-71%.22 Gemcitabine and the taxanes paclitaxel and docetaxel may be used in combination, even in the treatment of BCG-Unresponsive disease (Figure 2).
BCG Unresponsive Disease
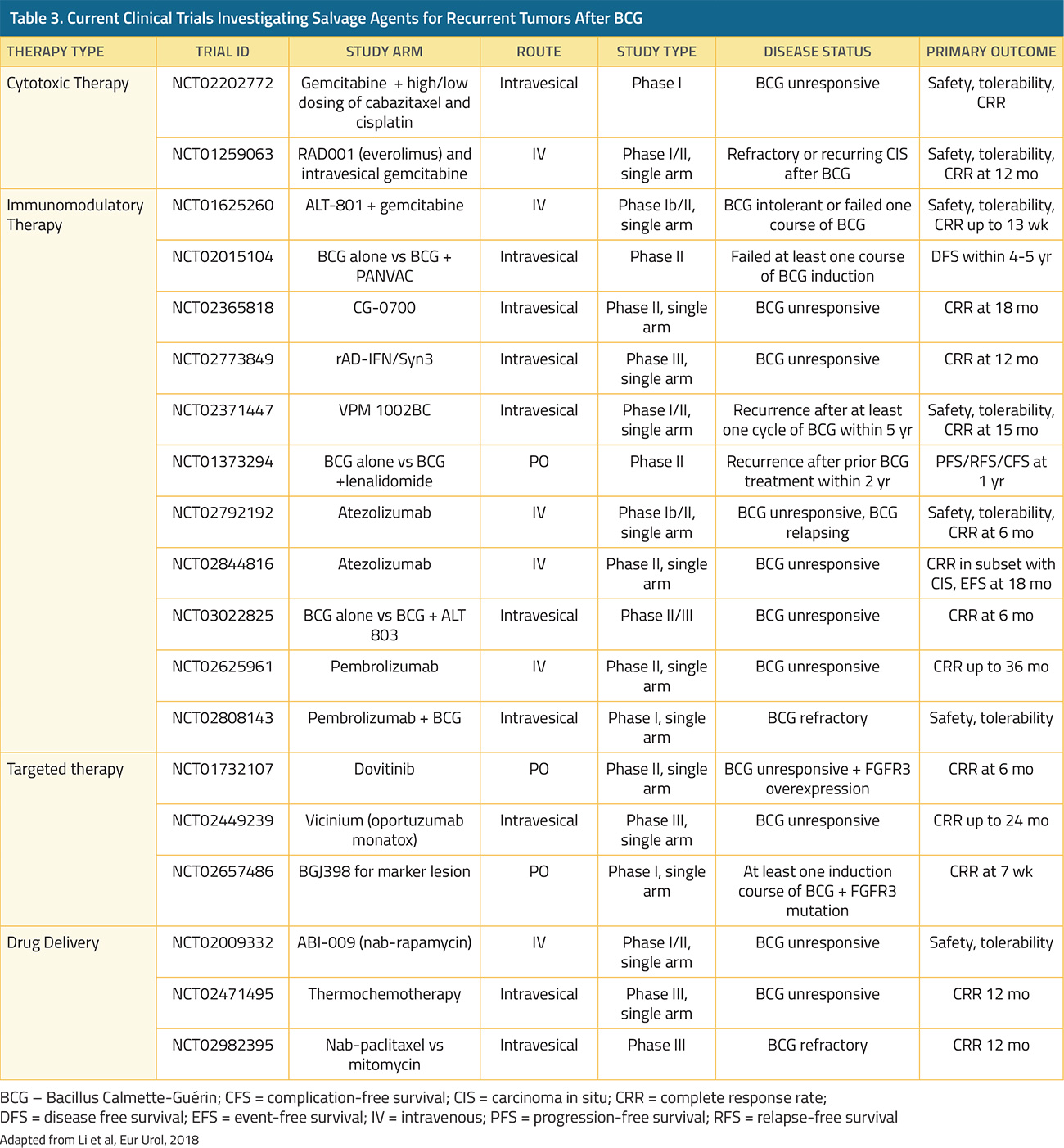
Recurrent tumors after intravesical BCG treatment confer a high risk of progression and salvage radical cystectomy is recommended.23  In practice, many patients may need to resort to less radical treatment options due to their physical frailty or rejection of complete bladder removal. Alternate options for these patients remain scarce. Valrubicin, the only approved agent for recurrent CIS after intravesical BCG treatment, has only an 8% complete response rate at 30-month follow-up.24 Alternative options include other intravesical chemotherapies including gemcitabine, docetaxel and sequential or combination therapy (Table 2). Gene therapies options include the use of Instiladrin®, an IFN-α expressing recombinant adenoviral vector, which has recently achieved 35% 12-month relapse-free survival in a cohort of high risk, BCG-Unresponsive NMIBC patients (Figure 2).25 Ongoing trials in this space are listed in Table 3.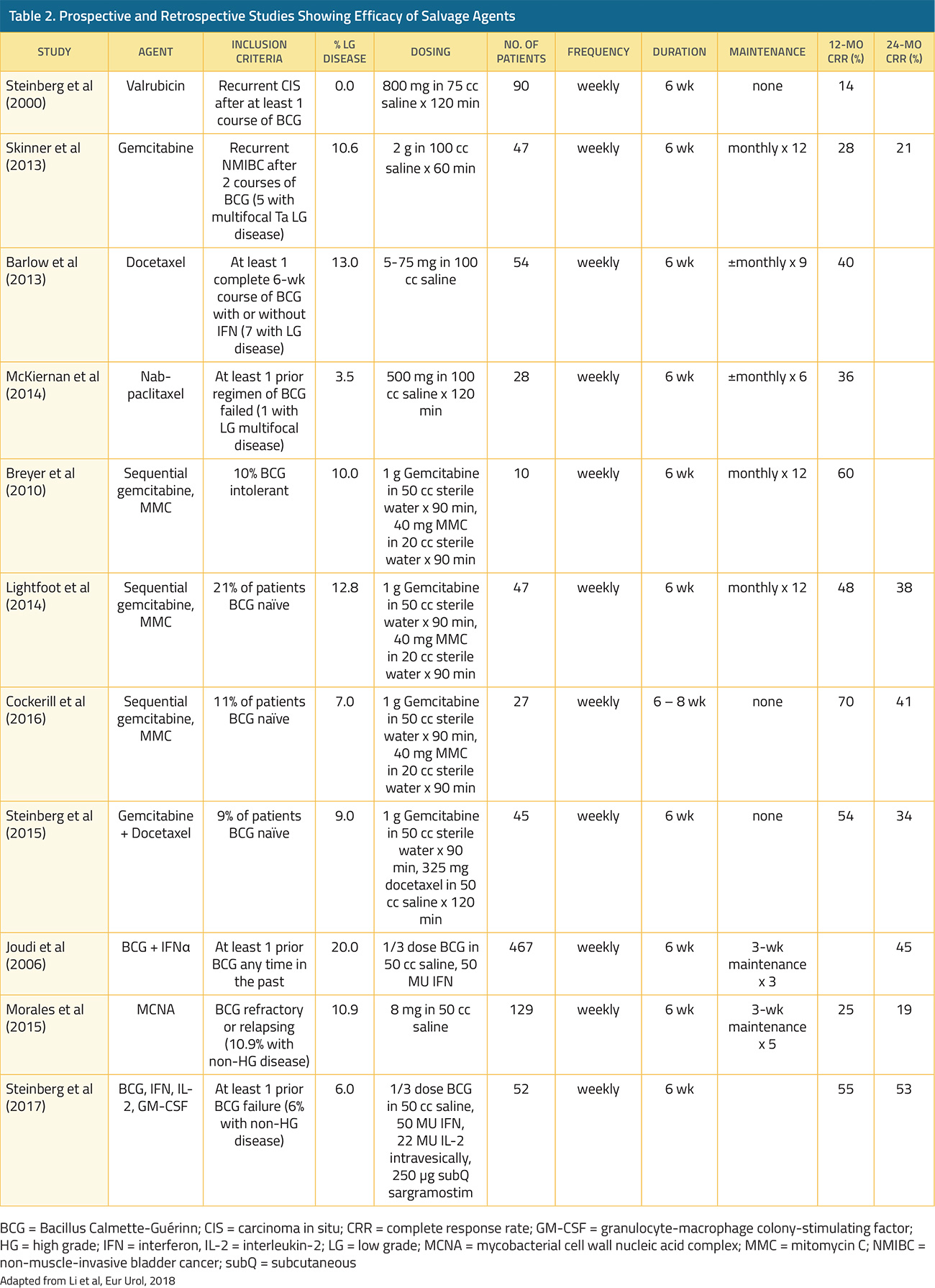
Strategies for Surveillance
Due to its high recurrence rate and the need for vigilant cystoscopic surveillance, the management of bladder cancer is the most costly amongst all cancers in the US; $2.2 billion was spent in 2003.26  Surveillance relies on cystoscopy and urine cytology, with most recommending this every 3 months up to 24 months after initial diagnosis, followed by every 6 months up to 5 years.19Although generally regarded as the urinary test of choice, urine cytology has very low sensitivity (48%), especially in detecting a low-grade tumor (16%).27 Recent studies have also demonstrated the decreased performance of cytology for high-grade tumors – for example in a recent multicenter study, as many as 40% of CIS were not detected by cytology. Thus, caution must be exercised when relying on cytology alone.28  Other urinary markers available today include BTA stat and BTA TRAK (detect human complement factor H-related protein), ImmunoCyt (fluorescent-labeled monoclonal antibodies), NMP22 (detection of nuclear matrix protein 22), UroVysion (FISH of DNA probes specific for bladder cancer aneuploidy) and Cxbladder (measures the expression of 5 biomarkers). However, none are recommended for use in the management guidelines other than potential use of Urovysion FISH in clarifying atypical cytology or in predicting response to BCG. A positive FISH result after BCG induction confers an increased risk of recurrence (3-5 fold) and progression (5-13 fold), depending on the timing of FISH positivity.  For example in one study; at the 3-month time point, patients with a positive FISH result had a 58% risk of recurrence compared to 15% with a negative result (p < 0.001). For disease progression, the incidence was 25% with a positive FISH compared to 7% with a negative result (p < 0.013).29 Since many patients who have a positive FISH test have no visible tumor at the time of assessment but subsequently develop recurrence in 6-24 months, this phenomenon has been categorized as a molecular failure and such patients can be considered for clinical trials for salvage therapies.30
In addition, cytokines and biomarkers have been assessed to predict response to BCG. However, due to the complexity of the immune response to BCG, no single marker is likely to definitively predict a positive or negative response. We have prospectively tested the hypothesis that a panel of urinary cytokines can accurately assess the multifaceted immune response generated by intravesical BCG.31 A nomogram (CyPRIT, Cytokine Panel for Response to Intravesical Therapy) using a panel of 9 cytokines (IL-2, IL-6, IL-8, IL-18, IL-1ra, TRAIL, IFN-g, IL-12[p70], and TNF-a) was found to have an accuracy of 85.5% in predicting response to BCG (95% CI 77.9–93.1%). Efforts to validate the use of CyPRIT are currently underway.
Published Date: April 16th, 2019