First Published April 2, 2020
The ongoing pandemic involving severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) and its resulting coronavirus disease 2019 (COVID-19) has caused widespread infection worldwide, with over 660,000 confirmed cases as of March 28, 2020 and nearly 31,000 deaths.1 Data from the Italian National Institute of Health (Istituto Superiore di Sanità [ISS]) where fatalities are thus far the highest suggest a fatality rate of 7.2%, significantly higher than that which has been observed in other countries.2 Elderly patients are at greatest risk of mortality from COVID-19, and approximately 23% of the Italian populace is aged 65 years or older, making the country particularly vulnerable.2
Emerging data has also suggested that patients with cancer are at a higher risk of contracting COVID-19 and having poorer outcomes following infection. Researchers from the National Clinical Research Center for Respiratory Disease in China found in an analysis of 1590 cases from 575 hospitals that the incidence of COVID-19 was higher in cancer patients relative to the overall incidence of cancer in China (1% vs 0.29%, respectively).3 More concerningly, patients with cancer were found to have a higher risk of requiring ventilatory support and death. Furthermore, patients who underwent chemotherapy or surgery in the month prior to infection were at greater risk for adverse outcomes, even when adjusting for age and smoking history, with cancer history conferring the highest risk.3 Strategies to mitigate infection, as well as disease morbidity and mortality, are therefore urgently needed.
Bacillus Calmette-Guérin (BCG) vaccination is widely used to prevent tuberculosis. In addition to being the mainstay of management for patients with high-risk non-muscle invasive bladder cancer (though delivered intravesically in this context), other non-tuberculosis benefits of BCG have been demonstrated, including a 50% reduction in neonatal mortality in developing countries, with vaccinated infants having fewer cases of respiratory infection.4,5 Interestingly, BCG vaccination has also been shown to augment antibody responses to the 2009 pandemic influenza A (H1N1) vaccine.6 These non-specific effects of BCG may be due to genome-wide epigenetic reprogramming of monocytes caused by the vaccine, resulting in increased production of proinflammatory cytokines, conferring innate (trained) immunity and protection against viral infections even up to a year after BCG vaccination.6,7
Building on these findings, a Dutch research group led by S.J.C.F.M. Moorlag, Jaap ten Oever, and M.J.M. Bonten have initiated a multi-center, randomized controlled trial to study the effects of BCG vaccination on reducing the incidence of adverse events related to SARS-CoV-2 in patients 60 years of age or older. Given the uncertainty surrounding the dynamics of the ongoing pandemic, the study employs a design in which follow-up continues until a pre-defined number of endpoints are reached. Participants will be randomized to either an intradermal BCG vaccine (Danish strain 1331, SSI, Denmark) or placebo, in a 1:1 ratio (Figure 1). Participants will be blinded and followed using a mobile research follow-up app, which will track clinical symptoms, hospital admissions, and visits to general practitioners. In Australia, researchers from the Murdoch Children’s Research Institute have opened the BCG Vaccination to Protect Healthcare Workers Against COVID-19 (BRACE) trial (NCT04327206), a similar project but focused on healthcare workers. In this study, over 4,000 healthcare workers in Australia will be randomized to receive either a single dose of BCG vaccination (Danish strain 1331) or no vaccine, with subsequent follow-up over 12 months to determine the incidence of any COVID-19 disease or severe COVID-19 incidence Groups in the US, including ours in Houston (at MD Anderson Cancer Center (PI: Kamat) and Baylor College of Medicine (PI: DiNardo) as well as in Boston (Harvard Medical School, PI: Murray), are also in the process of initiating a trial studying BCG vaccination to protect healthcare workers against COVID-19, the ‘BADAS Trial’.
Figure 1. The BADAS Study: (BCG vaccination As Defense Against SarsCov2: A randomized controlled trial to protect health care workers by enhanced trained immune responses) in the US, will follow a scheme similar to that below, but be focused on high-risk health care workers 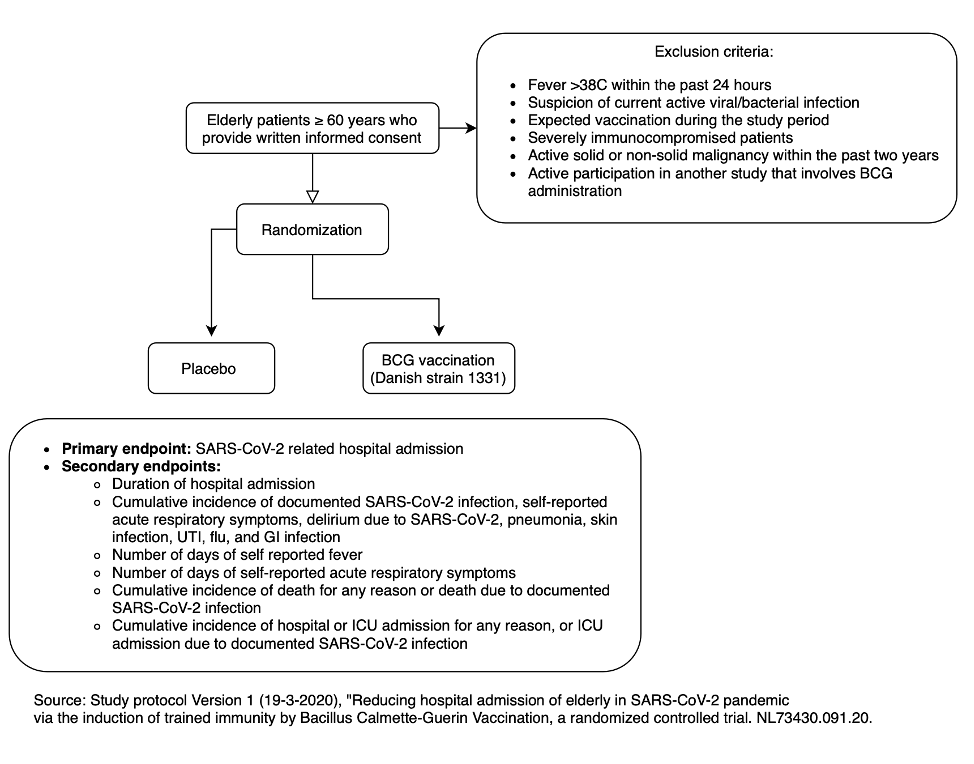
Intriguingly, Hegarty and colleagues describe in an upcoming editorial in European Urology Oncology the observation that when comparing crude case fatality rates (CFR) of COVID-19 between countries with active BCG vaccination programs to those that do not routinely vaccinate, differences exist between incidence of disease and CFR.8 For instance, the daily incidence of COVID-19 was 0.8/million in countries with a BCG vaccination program compared to 34.8/million in countries without such a program as of March 22, 2020.8 Additionally, based on rough estimates and available data, CFR was estimated to be 4.1% in countries with a BCG vaccination program compared to 5.1% in those without.8 Furthermore, the map of countries most affected with COVID-19 in Europe shows considerable overlap with the map of countries without a national program of BCG vaccination as per BCG World Atlas (Figure 2).8
Figure 2. (a) Map displaying BCG vaccination policy in Europe by country. Red denotes a country without a current BCG vaccination program. Data courtesy of the BCG World Atlas. (b) Screenshot of heat map of COVID-19 cases in Europe, available on the European Centre for Disease Prevention Control website, accessed March 28, 2020.8

Although multiple confounders exist in these analyses including heterogeneity in testing, lack of confirmation of true BCG vaccination status, and a likely underestimation of asymptomatic cases, they highlight the need for further study. A more detailed analysis has also been performed and submitted for peer review and will be shared once we are able.
These and similar efforts our attention as we work to support the efforts of our colleagues on the frontlines, both for their potential to mitigate the virulence of SARS-CoV-2 and for the additional knowledge such studies will likely yield in understanding the broader immunological mechanisms that underlie the efficacy of BCG. Clearly, with shortages already limiting access to intravesical BCG for our bladder cancer patients, this is not a project we would embark on without considerable thought. However, based on discussions with the largest bladder cancer patient advocacy group, BCAN (Bethesda, MD), it is evident that COVID-19 has already led to a negative impact on the bladder cancer community, both directly at the patient level and indirectly via the institutions which serve them. For example, COVID-19-related issues have reduced the ability and willingness of patients to receive intravesical BCG treatments, with many institutions canceling maintenance regimens or patients unwilling to risk travel due to COVID-19 restrictions. BCG demand may, as a result, lessen as we attempt to flatten the curve. However, good stewardship of these resources must still remain a priority. We anticipate that one vial of BCG, normally used for a single bladder cancer patient, could vaccinate up to 300 - 500 healthcare workers. If the healthcare worker trial and others are positive, BCG vaccination could create a safer environment for providers, the patients they serve including bladder cancer survivors receiving treatment, and the general population.
Thus, provided we manage our resources well the diversion of BCG from bladder cancer to fight COVID-19 would be a relatively small investment in exchange for potentially huge implications.
Authors: Vikram M. Narayan1, Paul Hegarty2, Gianluca Giannarini3, Rick Bangs4, Stephanie Chisolm5, Ashish M. Kamat1
1. Department of Urology, University of Texas MD Anderson Cancer Center, Houston, TX, USA
2. Department of Urology, Mater Misericordiae University Hospital, Dublin, Ireland
3. Urology Unit, Academic Medical Centre “Santa Maria della Misericordia”, Udine, Italy
4. Patient Advocate, SWOG, San Antonio, TX, USA
5. Bladder Cancer Advocacy Network (BCAN), Bethesda, MD, USA
Related Content:
Listen: The BADAS Trial: BCG Vaccination Against SARS-CoV-2 to Protect Health Care Workers by Enhanced Trained Immune Responses - Ashish Kamat
Read: Video Transcript: Is BCG Effective Effective Against Coronavirus? Dr. Ashish Kamat Speaks To Rajdeep | News Today
Read: The BADAS Study: BCG As Defense Against SARS-CoV-2: A Randomized Multicenter Trial