Diagnosis:
Clinical PresentationThere are no reliable screening tests available for detecting bladder cancer; hence the diagnosis is usually made based on clinical signs and symptoms. Painless hematuria – microscopic or gross – is the most common presentation and a hematuria investigation in an otherwise asymptomatic patient detects bladder neoplasm in roughly 20% of gross and 5% of microscopic cases.1,2 Irritative voiding (frequency, urgency, and/or dysuria) is usually ascribed to benign urinary tract disorders but has been associated with carcinoma in situ. Other symptoms are often a signal of more advanced disease, such as flank pain caused by ureteral obstruction or pelvic pain from extravesical invasion of surrounding structures.
Cystoscopy
Cystoscopy is a mainstay for the diagnosis and treatment of bladder cancer, allowing for direct access to a tumor for biopsy, fulguration, and/or resection. Low grade (LG), papillary (Ta) tumors can be reliably eradicated with one treatment but more advanced disease (high grade and/or T1) often requires repeat resection for complete eradication. Following an initial diagnosis of HG Ta or T1, between 40% and 78% of re-TUR specimens may contain residual disease, with muscle invasion present in 2% and 14%, respectively.3-6 Hence the AUA and EAU guidelines recommend repeat TURBT within 6 weeks from the index procedure to confirm tumor stage, ensure complete visual tumor clearance, and optimize response to subsequent intravesical therapy.7,8
Recent technological advances promise improved detection over white light cystoscopy (WLC) alone, theoretically allowing for a more complete endoscopic tumor removal. Blue light cystoscopy (BLC) has been approved for over a decade in Europe and the US based on numerous studies showing improvement in detection of bladder tumors as well as lengthening the time to recurrence by as much as 7 months (9.4 months vs 16.4 months). The improvement in tumor detection estimated to be 20% greater with BLC compared to WLC, and up to 40% specifically for CIS, however, the beneficial effect on disease recurrence and/or progression has not been universally reported in all studies.9-12 Narrow band imaging (NBI) also offers better detection than WLC but does not require a pre-operative medication instillation like BLC. Specialized optical equipment emits light in two specific wavelengths (415 nm and 540 nm) that are more readily absorbed by hemoglobin, thereby enhancing submucosal vascularity associated with malignancy.13 In a recent systematic review of five RCTs comparing WLC to NBI, the authors found statistically significant reduction in NMIBC recurrence at 3 months (RR 0.39), 1 year (RR 0.52), and 2 years (RR 0.60).14 No matter the technique, enhanced cystoscopy improves detection but whether the added time and expense translate into improved patient outcomes is still not entirely clear.
Urinary Markers
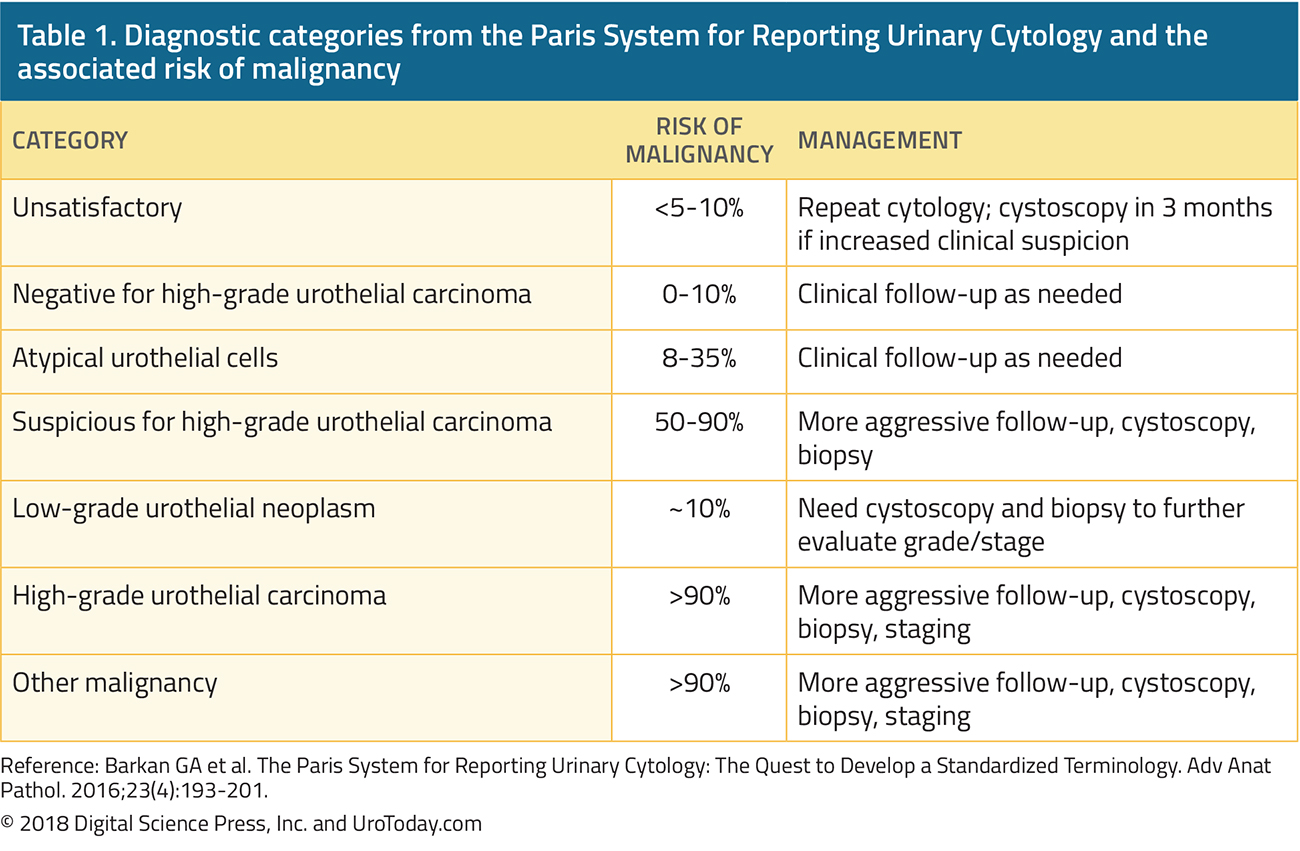
The urothelium is particularly well suited anatomically for assessment of potential biomarkers that can be obtained with little to no need for invasive procedures. Cells and cellular molecules (proteins, RNA, etc.) shed into the urine as it passes through the upper and lower urinary tract; they can be collected and purified from voided or catheterized specimens. The information gathered can then be used for screening, diagnosis, treatment response, and/or surveillance. The most well-known and widely used technique is urinary cytology, by which the cellular component of a urine specimen is microscopically assessed for features typically associated with high-grade malignancy (mitotic figures, condensed chromatin, enlarged nucleoli, etc.). Interpretation and reporting by cytopathologists has contributed to confusion surrounding urinary cytology with the use of terms like “suspicious, atypical, or indeterminate. The Paris Reporting System for Urinary Cytology has standardized the cytopathologic nomenclature while providing an estimated risk of malignancy based on associated literature (Table 1).15 While specificity has historically been very high (>99%), the poor sensitivity of urinary cytology, especially for papillary tumors (4-31%), make it far from ideal for either screening or surveillance.16-19 More contemporary data has been less robust, placing specificity at a more modest 82-88% and highlighting the need for more advanced markers.20
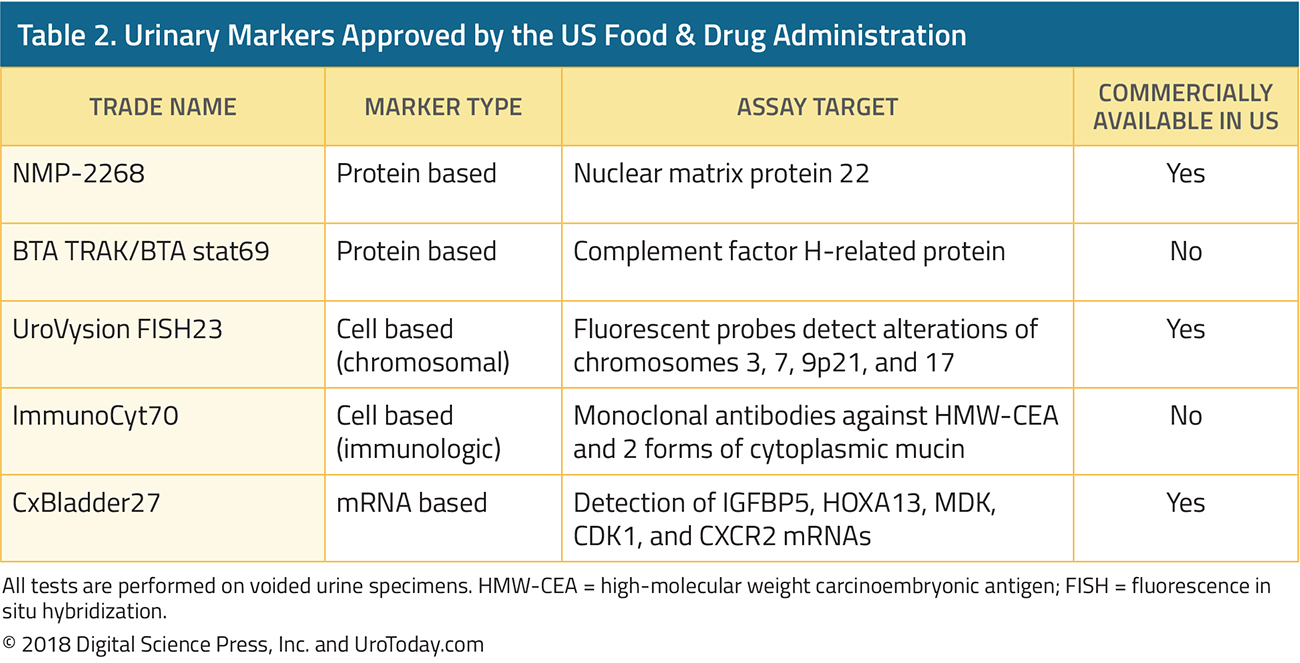
There are now five FDA-approved tests available (Table 2) in addition to many more potential biomarkers (i.e. DNA methylation, cell free DNA, histone modification) in various stages of development.21,22 The UroVysion test uses fluorescence in situ hybridization (FISH) to detect common chromosomal aberrations associated with bladder cancer and outperforms urinary cytology in terms of sensitivity, though this is almost entirely attributable to better detection of Ta tumors.23 The ImmunoCyt (uCyt+) assay was designed to complement cytology and increases the sensitivity to 59% for grade 1 tumors and up to 90% for grade 3 by using monoclonal antibodies directed against common urothelial surface markers.24 Nuclear matrix protein-22 (NMP-22) is involved in normal chromatin maintenance during mitosis but is greatly overexpressed in bladder carcinoma cells. Despite a reported sensitivity of 73% and specificity of 80%, the test has not gained widespread acceptance due to variability in accuracy between institutions and a high rate of false positive tests.25,26 The newest test to gain FDA-approval is the RNA based CxBladder test which measures the relative levels of 5 different mRNA transcripts within the urine (4 associated with malignancy and 1 with benign conditions) to produce an impressive combination of sensitivity and specificity at 82% and 85%, respectively.27,28
To date, none of the available data supports the use of urinary biomarkers as the sole method of bladder cancer detection, diagnosis, or follow-up, as stated by both the EAU and AUA in their respective NMIBC guidelines, however, they may offer useful information when assessing treatment response and during long-term surveillance as an adjunct to cystoscopy.7,8 Initial enthusiasm for these tests in the early to mid-2000s has waned, whereas use of urinary cytology has remained constant despite its shortcomings.29 The use of markers in prognostication and prediction of response to therapy is discussed in the next section on management of NMIBC.
Imaging
A complete diagnostic evaluation includes imaging of the entire urinary tract to assess for abnormalities of the urothelium normally out of view from cystoscopy. Upper tract urothelial tumors are uncommon, present in only 1.5% of patients with NMIBC, but certain features (multifocality, trigonal lesions, and/or CIS) raise this risk to more than 7%.30,31 The best combination of sensitivity (67-100%) and specificity (93-99%) is offered by computed tomographic urography (CTU) because of high soft tissue special resolution and contrast enhanced assessment of the urothelial surfaces and this has replaced intravenous urography in most centers in North America.32-35 Magnetic resonance imaging can be used as a substitute for CTU if the patient has an allergy to iodinated contrast or low GFR.36 In an effort to standardize MRI reporting and improve diagnostic accuracy, the multiparametric MRI based Vesical Imaging-Reporting and Data System (VI-RADS) was introduced in early 2018 with a 5 tiered system designed to predict likelihood of finding muscle invasion on TURBT, though it has not been validated in the clinical setting as of yet.37 Ultrasonography with retrograde pyelography is reserved for circumstances where both CT and MRI cannot be performed.
Pathology:
Urothelial carcinoma is the most common bladder cancer histology (~90%) diagnosed in the US, followed by squamous (2-5%), adenocarcinoma (2%), neuroendocrine (1%), and other rare tumors (<1%).38 The urothelium is the epithelial lining of the urinary tract and has a thickness in the bladder of approximately 5 to 7 cell layers overlying the lamina propria. Tumors that are confined to the bladder and do not invade the muscularis propria are considered non-muscle invasive bladder cancer (NMIBC) comprised of stages Ta, T1, and carcinoma in situ (CIS). Invasion of the muscularis propria – so called muscle invasive bladder cancer (MIBC,T2)“ represents an advanced stage with life threatening consequences requiring surgical management (i.e. radical cystectomy).Tumor Grading
Tumor grade is an important prognostic feature of bladder cancer but there is a lack of consensus internationally regarding the classification system. The extreme ends of the spectrum (highly aggressive and low malignant potential) are easy to identify but the middle ground has proved more elusive. In the World Health Organization 1973 grading system, there are 3 tiers of tumor grade (1, 2, and 3), though a majority of tumors end up as the intermediate grade 2 as a diagnosis of exclusion. The International Society of Urologic Pathologists (ISUP)/WHO 2004 grading system includes only high or low grade and exhibits better prognostic ability over the WHO 1973 system, at the expense of upward stage migration.39,40 Enrichment of the grade 3 group via inclusion of borderline grade 2 cases only leaves more indolent disease in the LG category and exposes those patients to overtreatment. The final version released as the ISUP/WHO 2004 grading system (now updated with minor revisions as the 2016 system) has been adopted throughout North America but the 1973 version is still in widespread use across Europe (Figure 1).41

Divergent Differentiation and Histologic Variants
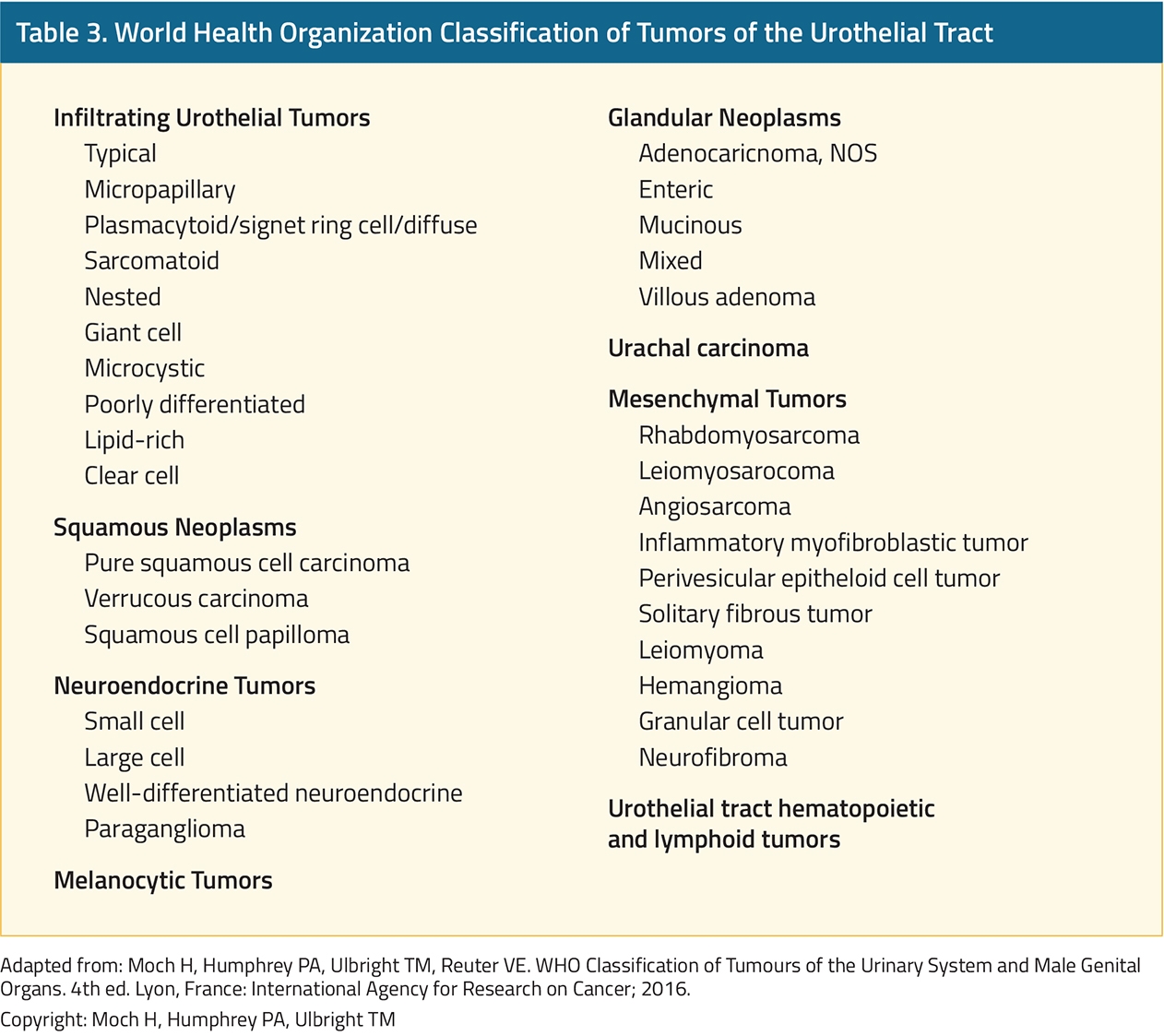
The ability of the urothelium to exhibit divergent differentiation is well known and may occur in a pure or mixed form (Table 3).42,43 When certain subtypes are present without elements of usual urothelial carcinoma, the tumor is referred to in terms of its pure histology (i.e. squamous cell carcinoma [SCC] of the bladder, adenocarcinoma of the bladder), in contrast to variant histology discussed below.41 Adenocarcinoma has a typical glandular (intestinal) appearance and tends to be more aggressive than UC.44 As such, complete early resection with radical cystectomy is advocated, even for T1 tumors, to achieve the best clinical outcomes.45 Pure SCC is more common in regions with endemic Bilhazrial infections and has been associated with a favorable clinical course, however, the non-infectious form is a distinct entity with a worse prognosis warranting similar management as adenocarcinoma.46 Small cell carcinoma is a neuroendocrine tumor with a very high propensity for distant spread at presentation and should be treated with upfront chemotherapy followed by surgery if free of detectable metastasis.47
The impact of mixed histologic variants is less clear owing to multiple factors including low recognition historically among pathologists and tumor under-sampling during resection.48,49 In one study, repeat pathologic review of more than 1,200 bladder cancers diagnosed as pure UC between 1980 and 2005 found that 1/3rd actually contained a variant component.50 The sarcomatoid subtype is characterized by a mesenchymal and spindle-cell like appearance and exhibits a propensity for aggressive growth.51 These tumors present with extravesical invasion (T3-4) in about 1/3rd of cases.52 Micropapillary histologic architecture has been described in other malignancies and is typically associated with poor prognosis.53 Higher stage on presentation and increased likelihood for bladder invasion have been noted when even small regions of micropapillary differentiation are present (~10%), but the optimal treatment approach (neoadjuvant chemotherapy versus immediate RC) is still a topic for debate.54,55 Plasmacytoid variant is locally aggressive and frequently under-staged as evidenced by an 80% upstaging rate of clinical T1 to pathologic after cystectomy.56,57 The pattern of spread of plasmacytoid is particularly unusual for bladder cancer given its predilection for peritoneal implantation.58 The histologic appearance of nested subtype is similar to von Brunn nests, but unlike the benign nature of the latter, nested variant carries significant probability of muscle invasion (70%) and/or lymph node positivity (67%).59 Squamous and glandular differentiation are associated with a higher stage at initial diagnosis, however, clinical outcomes are no different than conventional urothelial carcinoma and standard treatment pathways should be sufficient.60,61 The AUA NMIBC guidelines direct the clinician to consider upfront radical cystectomy in T1 patients with any variant histology, citing the association of variant histology with a high rate of under-staging, however, the EAU guidelines limit their recommendation to only micropapillary histology.7,8,55,62
Molecular Classification
The accumulation of DNA damage necessary to produce bladder cancer requires several decades to occur, and as a result, MIBC exhibits a very high mutational burden and chromosomal instability. Concurrent genomic studies from several international research groups produced a range of intrinsic MIBC molecular subtypes with similar expressional profiles but different nomenclature. It is generally accepted that there are 2 major subtypes, luminal and basal, with better prognosis among the former. These tumors tend to be enriched for FGFR3 mutations associated with hyperproliferation and found at high frequency in non-invasive tumor. Despite the poor prognosis of the basal subtype, characterized by p53 mutations and alterations of DNA-damage repair pathways, these tumors are more responsive to platinum-based neoadjuvant chemotherapy than any other group.63 Low-grade tumors are genetically far more stable than MIBC, with highly conserved alterations in FGFR3 (79%), KDM6A (53%), and PIK3CA (52%).64,65 NMIBC has also been classified according to a molecular profiling schema, though it is less robust than what is available for MIBC. The major take-home point from this work thus far is the similarity between HG NMIBC and MIBC, pointing to a common pathway for progression.64,66,67
Published Date: April 16th, 2019