High-risk NMIBC treated with BCG induction and maintenance carries an approximately 40% rate of recurrence or progression at 2 years. No prior phase 3 trial had demonstrated that adding an immune checkpoint inhibitor to BCG improves EFS in this setting.
CREST is a global, phase 3, randomized trial enrolling patients with BCG-naive, high-risk NMIBC. Patients were assigned 1:1:1 to subcutaneous sasanlimab (anti-PD-1) combined with BCG induction and maintenance (Arm A; N=352), sasanlimab combined with BCG induction only (Arm B; N=352), or BCG induction and maintenance alone (Arm C; N=351). The primary endpoint was investigator-assessed EFS for Arm A versus Arm C; key secondary endpoints included EFS for Arm B versus Arm C and overall survival (NCT04165317).
Arm A met the primary endpoint: HR 0.68 (95% CI 0.49–0.94; one-sided P=0.0095). Estimated EFS at 36 months was 82.1% for Arm A versus 74.8% for Arm C. The EFS benefit was consistent across prespecified subgroups, including CIS and T1 disease. Overall survival follow-up was immature at the interim analysis. Grade 3 or higher treatment-related adverse events occurred in 29.1% of patients in Arm A versus 6.3% in Arm C.
Sasanlimab is the first anti-PD-1 antibody to demonstrate a statistically significant EFS improvement when combined with BCG-I+M in BCG-naive, high-risk NMIBC. The positive comparison is regimen-level: sasanlimab plus BCG induction and maintenance versus BCG induction and maintenance alone. The result establishes the effect of the combined regimen without resolving the independent contribution of PD-1 blockade versus continued BCG exposure. Patient selection within the BCG-naive, high-risk category, by molecular subtype, PD-L1 expression, or TURBT response kinetics, is not addressed by CREST. A grade 3+ TRAE rate of 29.1% in Arm A versus 6.3% in Arm C raises a benefit-risk question CREST was not designed to answer: within the BCG-naive, high-risk category, which patients' progression or recurrence risk most clearly justifies added systemic toxicity has not been separately identified. The Arm B versus Arm C result, sasanlimab plus BCG induction only, will determine whether BCG maintenance is necessary to preserve the benefit.

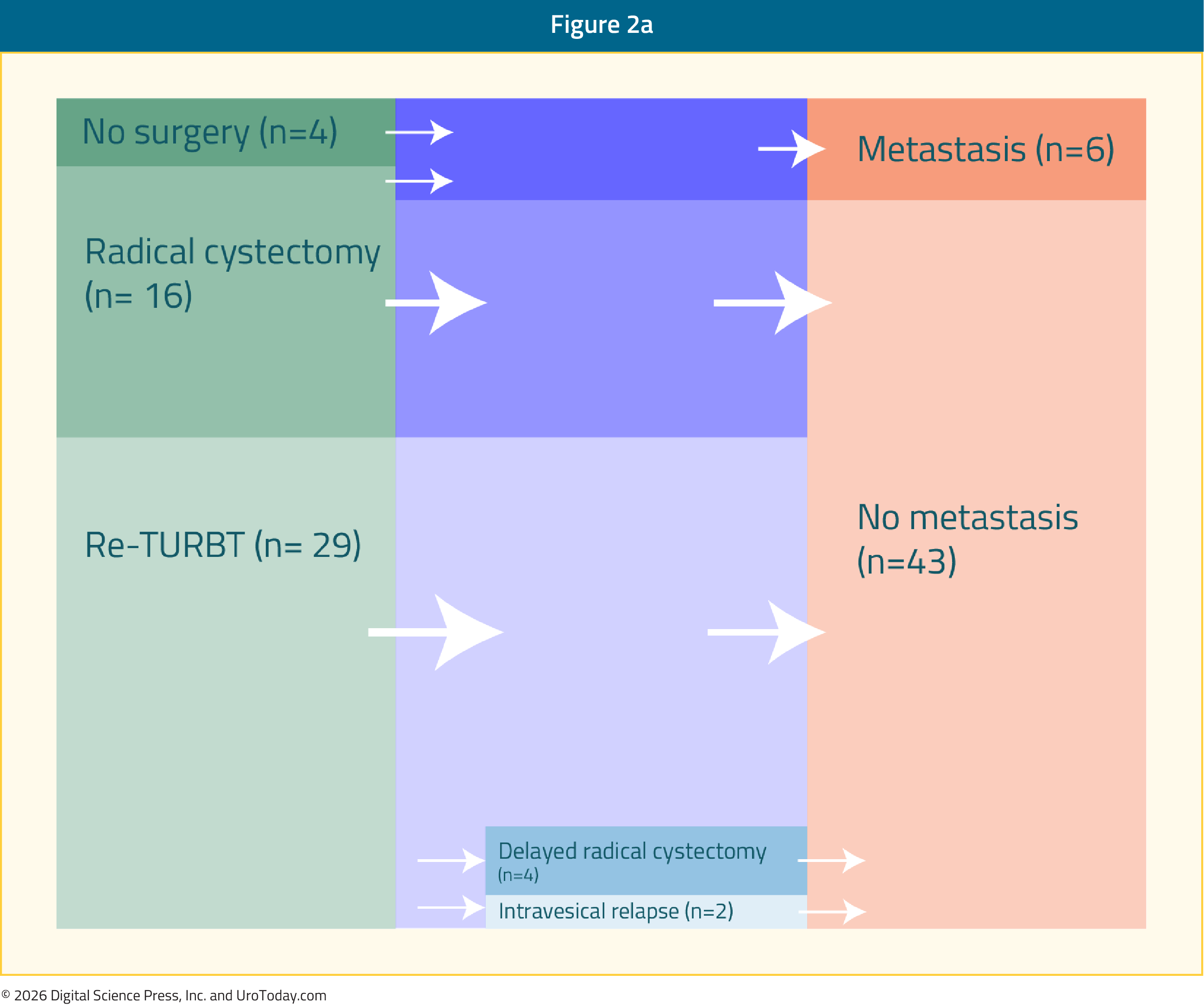
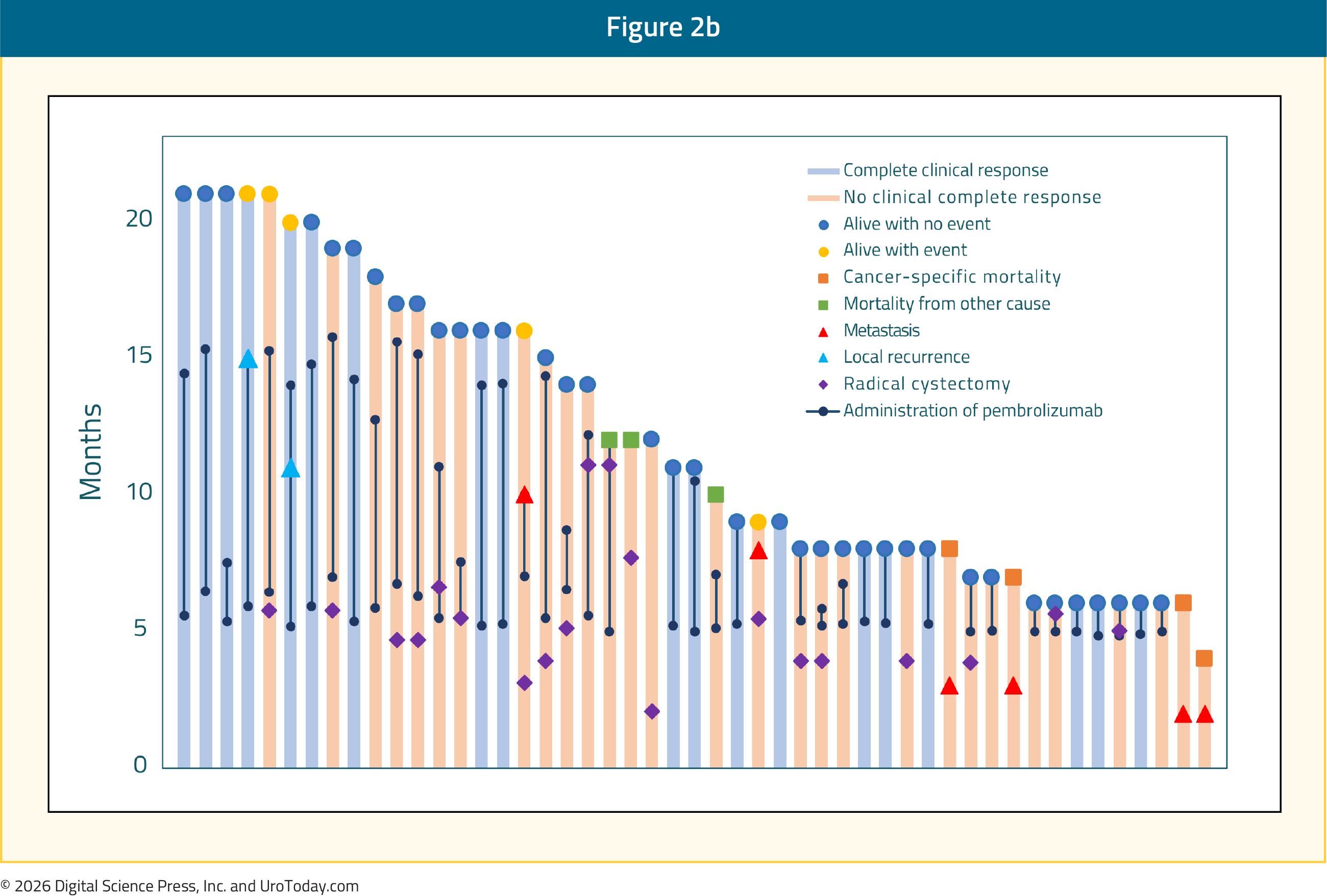
 Kaplan-Meier curves for investigator-assessed EFS in CREST. Arm A (sasanlimab plus BCG induction and maintenance) versus Arm C (BCG induction and maintenance alone), showing divergence sustained through 36 months. Shore et al. Nature Medicine, 2025. Figure 2a,b. DOI: 10.1038/s41591-025-03738-z
Kaplan-Meier curves for investigator-assessed EFS in CREST. Arm A (sasanlimab plus BCG induction and maintenance) versus Arm C (BCG induction and maintenance alone), showing divergence sustained through 36 months. Shore et al. Nature Medicine, 2025. Figure 2a,b. DOI: 10.1038/s41591-025-03738-z