Approximately half of patients with MIBC are ineligible for or decline cisplatin-based neoadjuvant chemotherapy. Trop-2-directed cytotoxic payload and checkpoint blockade offer mechanistically distinct and potentially complementary routes to tumor reduction before local therapy.
SURE-02 is a single-arm, phase 2 study at a single center (IRCCS San Raffaele Hospital, Milan). Eligible patients had histologically confirmed MIBC (cT2–T3bN0M0), ECOG PS 0–1, and were either ineligible for or declined cisplatin. All were scheduled for radical cystectomy. Patients received four cycles of pembrolizumab 200 mg on day 1 and sacituzumab govitecan 7.5 mg/kg on days 1 and 8, every 3 weeks, followed by radical cystectomy or re-TURBT (for patients who declined cystectomy after multidisciplinary board discussion) and 13 cycles of adjuvant pembrolizumab 200 mg every 3 weeks. The primary endpoint was cCR, defined as negative imaging and no viable tumor at re-TURBT, in the intention-to-treat population (NCT05535218).
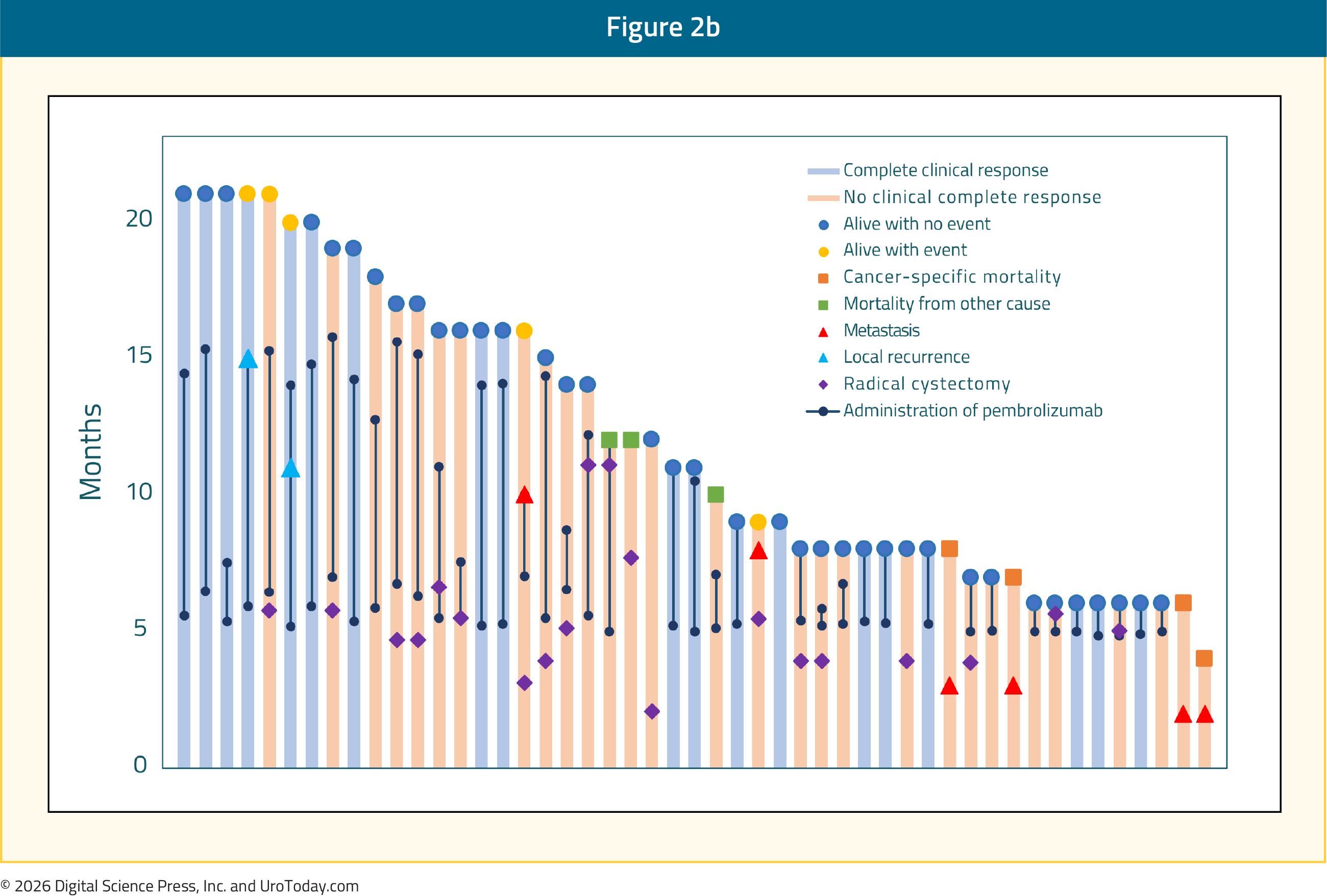
49 patients were enrolled and evaluable (63 screened; median age 66 years, IQR 61–71; 43% centrally confirmed variant histology; 67% cT2 stage). At a median follow-up of 14 months (IQR 8–18), 19 patients achieved cCR (39%; 95% CI 25–54%). All 19 underwent re-TURBT, all were metastasis-free at follow-up, and 2 developed intravesical relapse. Grade 3 TRAEs occurred in 8 patients (16%); diarrhea was most frequent (4 patients, 8%). Serious TRAEs were reported in 3 patients (6%): bullous pemphigoid in 2 and colitis in 1. No grade ≥4 or fatal TRAEs occurred.
A cCR rate of 39% in a cisplatin-ineligible population with 43% variant histology establishes clinical activity sufficient to justify a randomized evaluation. The bladder-preservation decision operated through multidisciplinary board review and re-TURBT confirmation rather than prospectively specified biomarker criteria for cystectomy omission. The next evidence needed is not simply a higher cCR rate in a larger cohort. The key question is whether residual-disease assessment, using ctDNA kinetics, repeat tissue biopsy, radiographic response, or cystectomy-pathology correlation, can identify patients for whom bladder preservation is oncologically safe, and whether the 39% cCR rate translates to durable local control at 2 and 3 years.
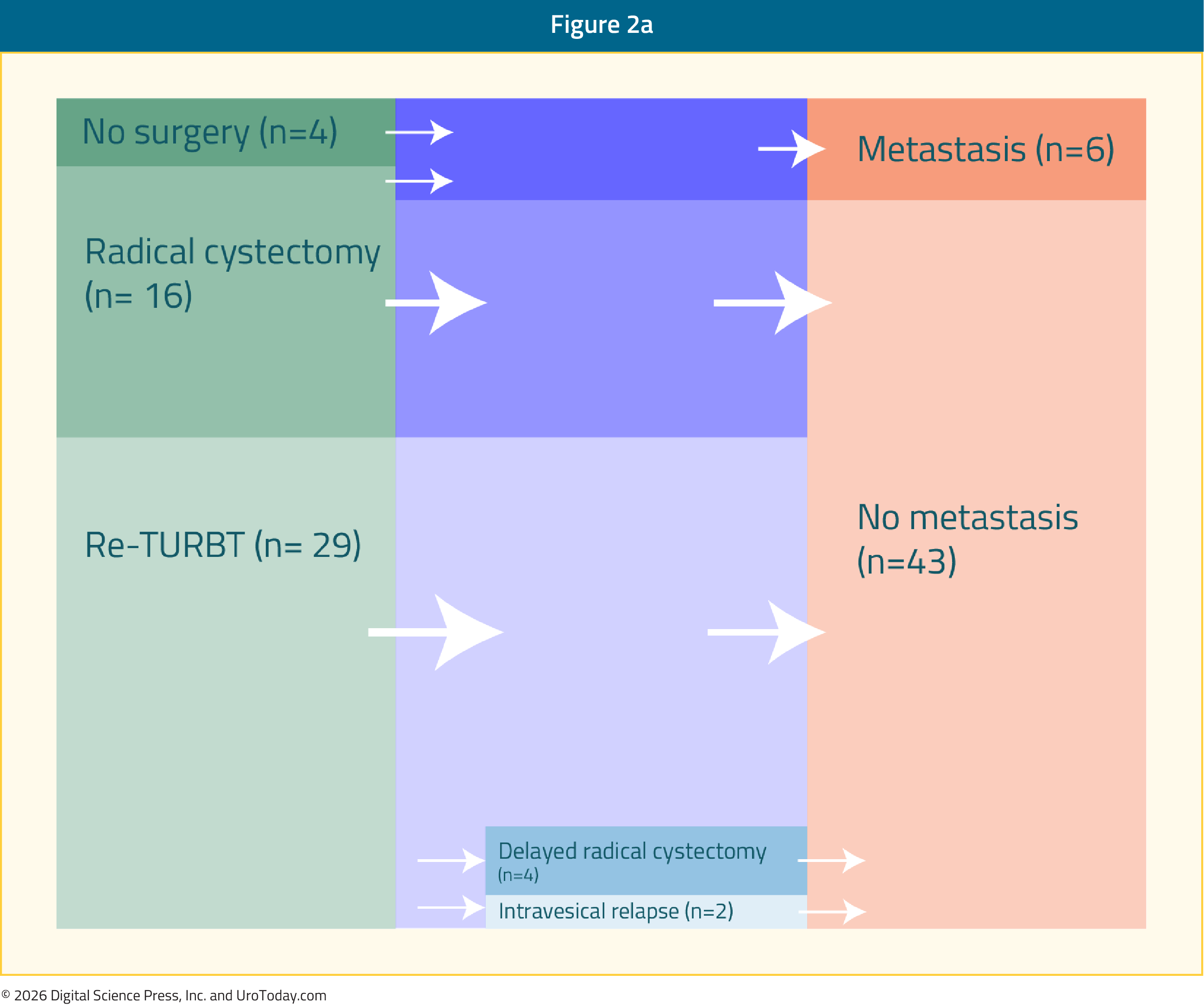
 SURE-02 treatment and response-adapted local-management schema. The figure places cCR in the clinical pathway, which is the central decision point for bladder-preservation development. Necchi et al. The Lancet Oncology, 2026. Clinical outcomes figure. DOI: 10.1016/S1470-2045(26)00050-1
SURE-02 treatment and response-adapted local-management schema. The figure places cCR in the clinical pathway, which is the central decision point for bladder-preservation development. Necchi et al. The Lancet Oncology, 2026. Clinical outcomes figure. DOI: 10.1016/S1470-2045(26)00050-1