Figure 1 – Metastases location has a significant prognostic impact in metastatic prostate cancer:
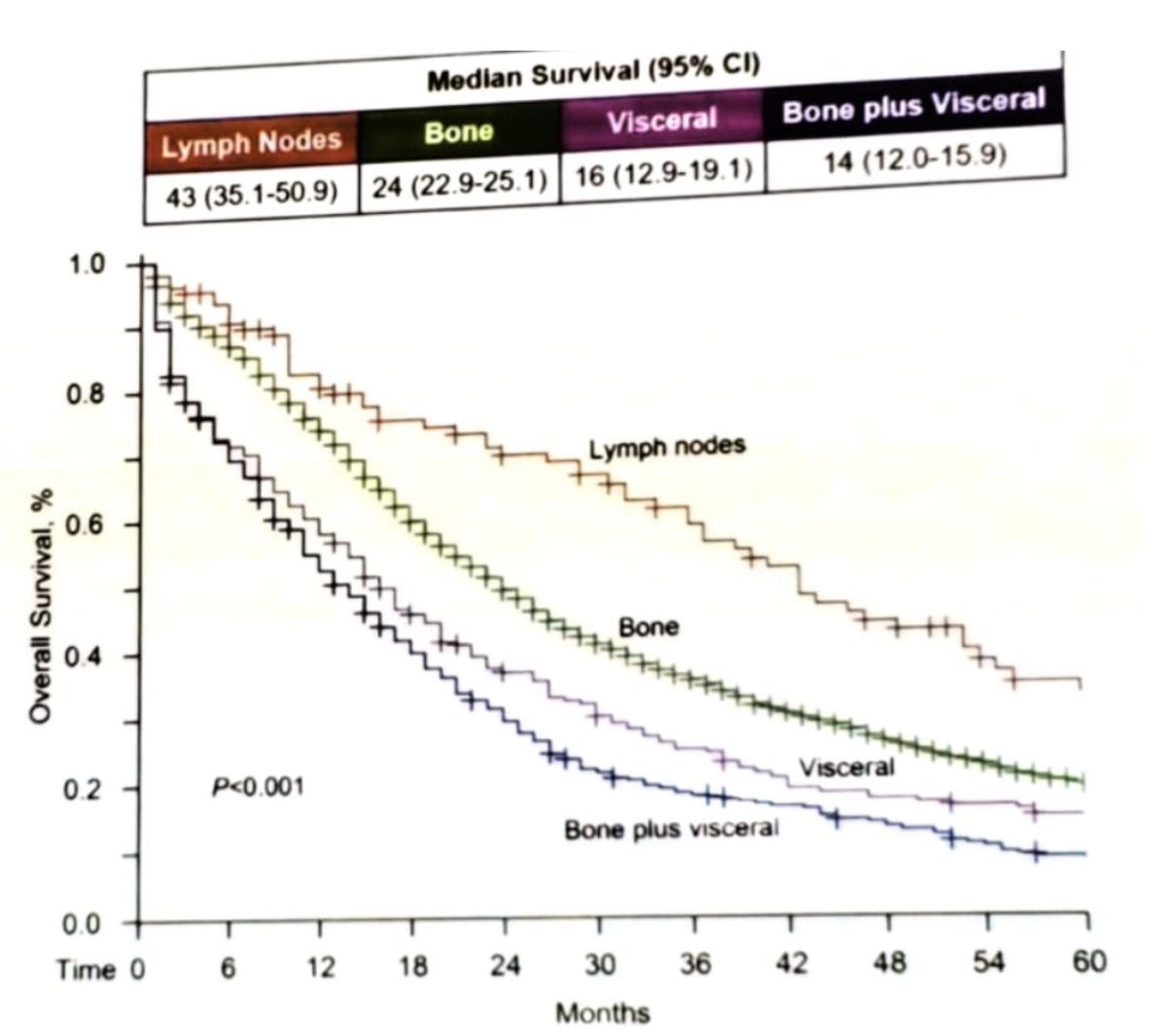
The metastases usually spread between distant sites rather than as separate waves form the primary tumor. Tumor cells sharing a common heritage trip from one site to another and retain their genetic imprint. This supports the “seed and soil” theory, in which subclones develop the potential to metastasize in the primary tumor, rather than being a property of the primary tumor.
Bone metastases are strongly associated with a higher risk of death and a higher risk of skeletal-related events (SRE). SREs, in turn, are associated with increased morbidity, higher treatment costs, and lower quality of life (Figure 2).
Figure 2 – The impact of bone metastases:
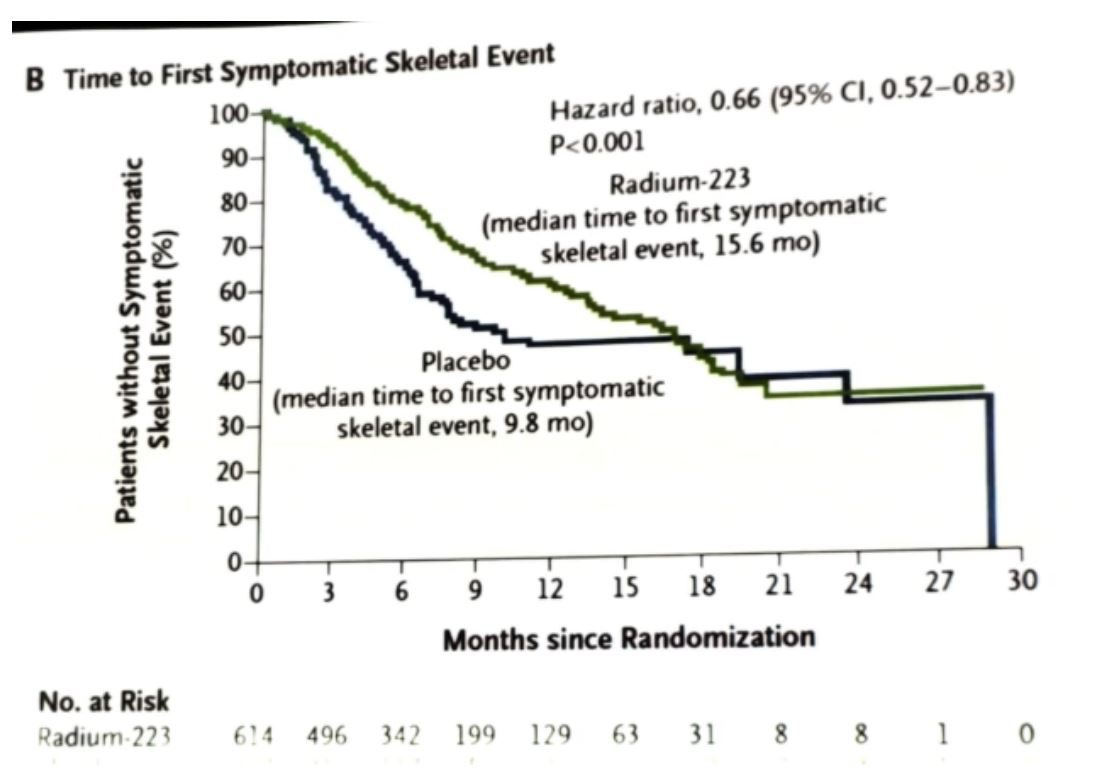
Radium-223 dichloride (radium-223) is a targeted alpha therapy and is incorporated into the newly formed bone in areas of osteoblast activity and increased bone turnover surrounding prostate cancer bone metastases.2,3 Radium-223 emits high energy alpha particles over a short-range. This results in a localized potent antitumor effect and also leads to inhibition of tumor-induced osteoblastic activity.4 Radium-223 is recommended for the treatment of patients with metastatic castrate-resistant prostate cancer (mCRPC) with symptomatic bone metastases.5 In the landmark trial showing the overall survival benefit of radium-223, the phase 3 ALSYMPCA study,6 mCRPC patients with symptomatic bone metastases assigned to radium-223 with best standard of care showed prolonged overall survival (median 14.0 vs 11.2 months, HR 0.70; 95% CI, 0.58–0.83; p < 0.001, as shown in Figure 3) and delayed time to first symptomatic skeletal event (SSE) compared with those assigned to placebo-treated with best standard of care6 (Figure 4). Radium-223 was generally well-tolerated and improvements in patient quality of life with this therapy were noted when compared with patients treated in the placebo arm.6
Figure 3 – Overall survival comparison between radium-223 and placebo in the ALSYMPCA trial:

Figure 4 – Symptomatic skeletal-related event comparison between radium-223 and placebo in the ASLSYMPCA trial:
Bone metastases are associated with multiple symptoms (Figure 5). Following treatment with radium-223, 42% of patients reported improved pain, 18% reported no change, 28% reported worsening pain, and 10% reported improvement and worsening. It has been shown that patients with less prior therapy completed more radium-223 cycles. Moreover, clinical parameters which reflect earlier disease stage were associated with radium-223 therapy completion. The total number of received Radium-223 cycles is correlated with overall survival and progression-free survival. Higher mortality was seen in patients who received less than 5 cycles compared to those who received more than 5 cycles (51% vs. 30%).
Figure 5 – The concept of treatment layering in metastatic castrate-resistant prostate cancer:
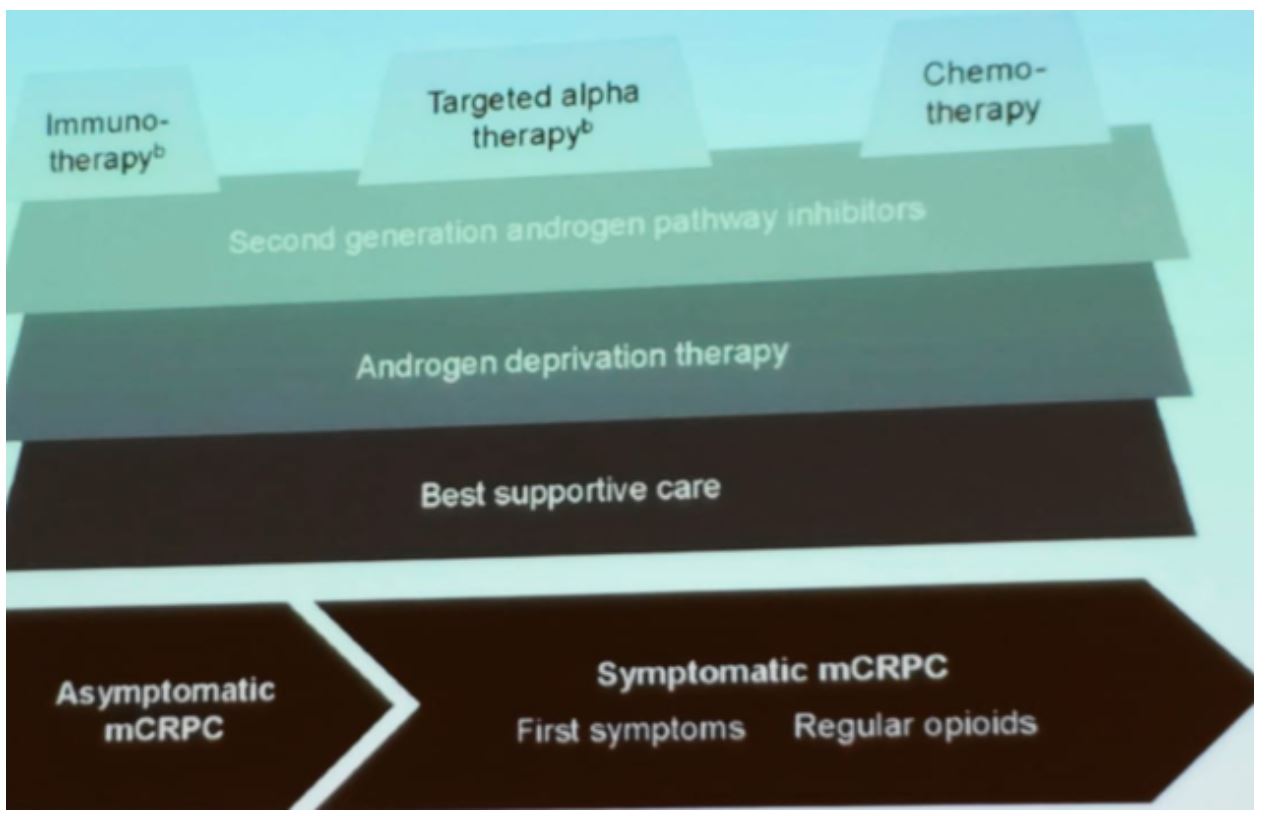
Combination therapies with Radium-223 and other used medications such as abiraterone or enzalutamide have not shown thus far, and overall survival benefit.7,8 These combinations, however, did show an increased rate of fractures that were reduced using bone protective agents. There are other analyzed combination therapies that might hold promise soon. These include the combination of radium-223 with sipuleucel-T, pembrolizumab, atezolizumab, and PARP inhibitors. The concept of treatment layering has been recently introduced in an attempt to optimize the treatment of patients with mCRPC.9 According to this concept, treatment should be given in a layered approach to optimize the treatment outcomes of these patients, as seen in figure 5.
Concluding his talk Dr. Koo emphasized some points. First, radiopharmaceuticals can have an overall survival benefit, while remaining quite a safe treatment option. Second, the concept of treatment should be according to the layering/combination of treatment rather than the sequencing of treatments. Importantly, preserving bone health is imperative and together with vitamin D and calcium, protective bone agents should be given to these patients. Lastly, it is unclear if moving treatment with Radium 223 to an earlier disease state will cause an overall survival benefit, and this will be needed to be further explored in the near future.
Presented by: Phillip Koo, MD, Division Chief of Diagnostic Imaging at the Banner MD Anderson Cancer Center in Arizona
Written by: Hanan Goldberg, MD, Urology Department, SUNY Upstate Medical University, Syracuse, New-York, USA @GoldbergHanan at the 2019 SNMMI Therapeutics Conference: Therapies, Theranostics, and Building Your Radionuclide Clinical Practice, October 25-27, 2019 in Las Vegas, Nevada.
References:
1. Gandaglia G, Karakiewicz PI, Briganti A, et al. Impact of the Site of Metastases on Survival in Patients with Metastatic Prostate Cancer. European urology 2015; 68(2): 325-34.
2. Henriksen G, Breistol K, Bruland OS, Fodstad O, Larsen RH. Significant antitumor effect from bone-seeking, alpha-particle-emitting (223)Ra demonstrated in an experimental skeletal metastases model. Cancer research 2002; 62(11): 3120-5.
3. Bruland OS, Nilsson S, Fisher DR, Larsen RH. High-linear energy transfer irradiation targeted to skeletal metastases by the alpha-emitter 223Ra: adjuvant or alternative to conventional modalities? Clinical cancer research : an official journal of the American Association for Cancer Research 2006; 12(20 Pt 2): 6250s-7s.
4. Suominen MI, Fagerlund KM, Rissanen JP, et al. Radium-223 Inhibits Osseous Prostate Cancer Growth by Dual Targeting of Cancer Cells and Bone Microenvironment in Mouse Models. Clinical cancer research : an official journal of the American Association for Cancer Research 2017; 23(15): 4335-46.
5. Parker C, Gillessen S, Heidenreich A, Horwich A. Cancer of the prostate: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Annals of oncology : official journal of the European Society for Medical Oncology 2015; 26 Suppl 5: v69-77.
6. Parker C, Nilsson S, Heinrich D, et al. Alpha Emitter Radium-223 and Survival in Metastatic Prostate Cancer. New England Journal of Medicine 2013; 369(3): 213-23.
7. Smith M, Parker C, Saad F, et al. Addition of radium-223 to abiraterone acetate and prednisone or prednisolone in patients with castration-resistant prostate cancer and bone metastases (ERA 223): a randomised, double-blind, placebo-controlled, phase 3 trial. The Lancet Oncology 2019; 20(3): 408-19.
8. Tombal BF, Loriot Y, Saad F, et al. Decreased fracture rate by mandating bone-protecting agents in the EORTC 1333/PEACE III trial comparing enzalutamide and Ra223 versus enzalutamide alone: An interim safety analysis. Journal of Clinical Oncology 2019; 37(15_suppl): 5007-.
9. Crawford ED, Petrylak DP, Shore N, et al. The Role of Therapeutic Layering in Optimizing Treatment for Patients With Castration-resistant Prostate Cancer (Prostate Cancer Radiographic Assessments for Detection of Advanced Recurrence II). Urology 2017; 104: 150-9.