The patient underwent a digital rectal examination demonstrating a T3 disease, with a total PSA of 8 ng/ml, and a prostatic health index of 62. The patient also underwent a 1.5 Tesla multiparametric MRI in another institution, which demonstrated a PIRADS 5 lesion with evidence of left seminal vesicle involvement in T2-weighted sequences with concomitant restricted diffusion at the ADC map. Furthermore, there was evidence of enlarged lymph nodes at the T1 sequence, at the right obturator (12 mm) and right external iliac (14 mm). The patient went on to have a transrectal targeted and systematic biopsy which revealed 10/15 cores positive for Gleason 7 (4+3) disease. His bone scan was negative, and his CT scan revealed two suspicious lymph nodes at the right obturator, measuring 12 mm, and a right external iliac node measuring 14 mm. Various treatment options were presented at this time, including radical prostatectomy, external beam radiotherapy + androgen deprivation therapy (ADT), or systemic therapies.
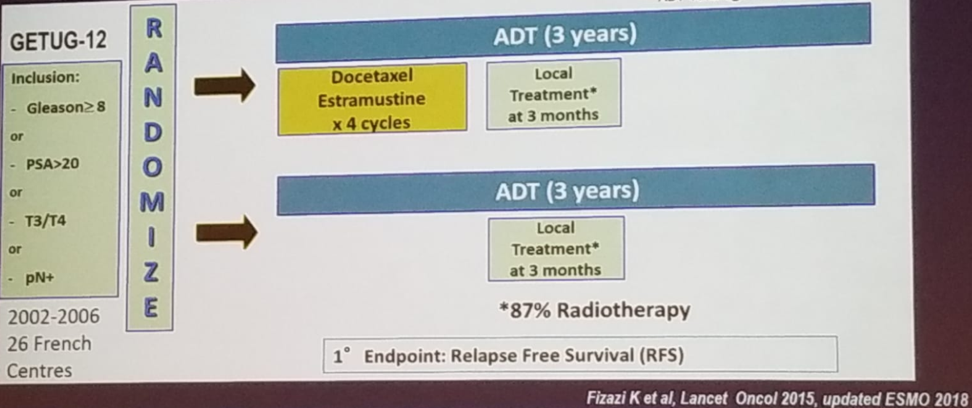
Dr. Gillessen began discussing the GETUG-12 trial1 which randomized high-risk prostate cancer patients to either ADT for three years, with a local treatment at three months and the addition of docetaxel for four cycles, or to ADT with local treatment only (Figure 1). The endpoint of the trial was relapse-free survival.
Figure 1 – GETUG-12 trial design:
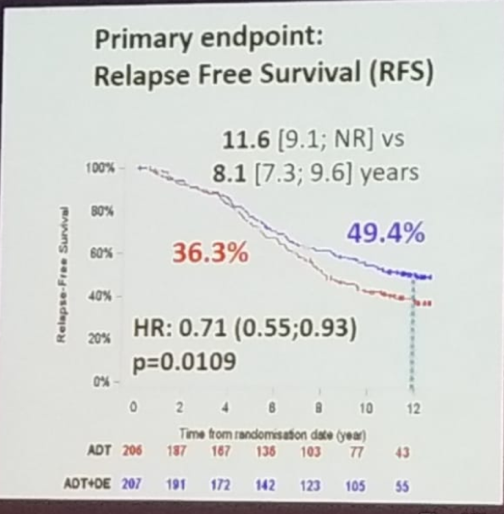
The trial demonstrated that docetaxel in these patients significantly improved relapse-free survival (49.4% vs. 36.3%, HR 0.71 [0.55-0.93], p=0.0109) and PSA response (Figure 2). However, there was no statistically significant difference in the metastasis-free survival, prostate cancer-specific survival and overall survival. Only 2% of the patients who received docetaxel had a neutropenic fever, with no toxic deaths demonstrated. The quality of life was not negatively impacted after one year due to chemotherapy. When specifically assessing patients with positive node disease, HR was 0.64 (0.43-0.96).
Figure 2 – Relapse-free survival in GETUG-12:
In a meta-analysis assessing the addition of docetaxel in M0 prostate cancer, an HR of 0.87 and 0.7 for overall survival and failure-free survival, respectively, were noted.2 Currently, the addition of chemotherapy is not part of the standard of care in unselected patients with M0 high-risk prostate cancer receiving ADT and EBRT.
The STAMPEDE trial demonstrated that abiraterone in high-risk M0 prostate cancer patients resulted in an improved failure-free survival with an HR of 0.21 (0.15-0.31), but no difference was seen in overall survival (HR 0.75, 0.48-1.18). 3 Therefore, abiraterone is also currently not approved for M0 high-risk prostate cancer patients, despite the interesting failure-free survival difference.
In conclusion, Dr. Gillessen does not recommend systemic therapy alone in this patient. EBRT should be given in combination with long-term ADT. Adding further drugs is an emerging concept, but the patient selection will be the key factor to consider.
Presented by: Silke Gillessen, MD, Professor and Chair in Genitourinary Oncology Systemic Therapy Research at The University of Manchester and The Christie NHS Foundation Trust, Co-founder of the Advanced Prostate Cancer Consensus Conference (APCCC)
Written By: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the 2019 American Society of Clinical Oncology Genitourinary Cancers Symposium, (ASCO GU) #GU19, February 14-16, 2019 - San Francisco, CA
References:
- Fizazi K et al.Androgen deprivation therapy plus docetaxel and estramustine versus androgen deprivation therapy alone for high-risk localised prostate cancer (GETUG 12): a phase 3 randomised controlled trial
Lancet Oncol. 2015 Jul;16(7):787-94. doi: 10.1016/S1470-2045(15)00011-X. Epub 2015 May 28. - Vale et al. Addition of docetaxel or bisphosphonates to standard of care in men with localised or metastatic, hormone-sensitive prostate cancer: a systematic review and meta-analyses of aggregate data
Lancet Oncol 2016 Feb;17(2), 243-256 - James N et al. Abiraterone for Prostate Cancer Not Previously Treated with Hormone Therapy July 27, 2017, N Engl J Med 2017; 377:338-351, DOI: 10.1056/NEJMoa1702900
Further Related Content:
Oligometastatic Disease: Tumor Board - A Urologic Oncologist Perspective by Edward Schaeffer, MD
Oligometastatic Disease: Tumor Board, A Radiation Oncologist Perspective by Bridget Koontz, MD
Oligometastatic Disease: Tumor Board - A Medical Oncologist Perspective by Michael Morris, MD
Oligometastatic Disease: Tumor Board - A Radiation Oncologist Perspective by Gert de Meerleer, MD