Catheters are semi-rigid but flexible tubes. They drain the bladder but block the urethra.
The challenge is to produce a catheter that matches as closely as possible to the normal physiological and mechanical characteristics of the voiding system.
This requires construction of a thin-walled, continuously lubricated, collapsible (conformable) catheter to protect the integrity of the urethra; a system to hold the catheter in place without a balloon; and a design to imitate the intermittent washing of the bladder with urine.
Catheter products have changed significantly in their composition, texture, and durability since the 1990s.
The catheter should have a smooth surface with two drainage eyes at the tip that allow for urine drainage.
Drainage eyes are placed either laterally or opposed. Opposing drainage eyes generally facilitate better drainage.
Catheter Tips
The most commonly used catheter is a straight-tipped catheter.
A Coudé-tipped catheter, or Tiemann catheter, is angled upward at the tip to assist in negotiating the upward bend in the male urethra.
This feature facilitates passage through the bladder neck in the presence of obstruction from a slightly enlarged prostate gland (e.g., in benign prostatic hyperplasia) or through a narrowed stricture in the urethra.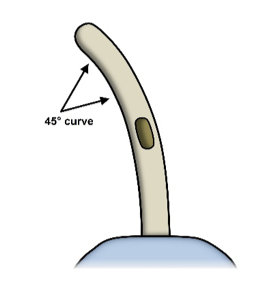
The Carson catheter is a slightly larger bulb to assist in negation of restrictions.
The Council catheter features a reinforced hole at the tip of the catheter.
A whistle-tipped catheter is open at the end and allows drainage of large amounts of debris (e.g., blood clots).
Catheter Size and Length
Each catheter is sized by the outer circumference and according to a metric scale known as the French (Fr) gauge (range is 6 to 18 Fr), in which each French unit equals 0.33 mm in diameter.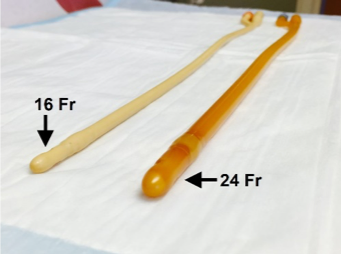
The golden rule is to use the smallest catheter size (termed bore), generally 14 to 16 Fr, that allows for adequate drainage.
The use of large-size catheters (e.g., 18 Fr or larger) is not recommended because catheters with larger diameters can cause more erosion of the bladder neck and urethral mucosa, can cause stricture formation, and do not allow adequate drainage of periurethral gland secretions, causing a buildup of secretions that may lead to irritation and infection. Also, large size catheters can cause pain and discomfort.
Balloon Size
A retention balloon prevents the catheter from being expelled. The preferred balloon size may be labeled either 5 mL or 10 mL, and both are instilled with 10 mL of sterile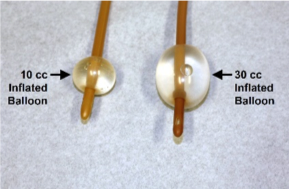 water for inflation per manufacturer’s instructions. Larger balloons (30 cc – 60 cc) are generally used to facilitate drainage or provide hemostasis when necessary, especially in the postoperative period. The balloon of the catheter usually sits at the base of the bladder, obstructing the internal urethral orifice.
water for inflation per manufacturer’s instructions. Larger balloons (30 cc – 60 cc) are generally used to facilitate drainage or provide hemostasis when necessary, especially in the postoperative period. The balloon of the catheter usually sits at the base of the bladder, obstructing the internal urethral orifice.
A fully inflated balloon allows the catheter tip to be located symmetrically. If a 5 mL balloon is inflated with more than 10 mL of water, irritation may occur unilaterally on the bladder wall from increased pressure of the balloon.
The specified amount of inflation ensures a symmetrical shape and allows for the catheter to maintain position in the bladder while minimizing patient discomfort Underfilling or overfilling may interfere with the correct positioning of the catheter tip, which may lead to irritation and trauma of the bladder wall.
A balloon with a fill size greater than 10 mL, such as a 30 mL balloon, is not recommended because the 10 mL size keeps residual urine minimal, thus reducing the risk of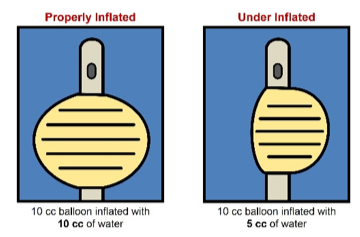 infections and irritation.
infections and irritation.
The catheterized bladder is in a collapsed state as a result of constant urine drainage. However, a 30 mL balloon will allow persistence of a small pool of undrained urine, so the bladder emptying is not complete and the undrained urine can leak around the catheter (referred to as “catheter bypassing”)..
The use of a larger balloon size is mistakenly believed by many nurses to be a solution to catheter leakage or urine bypassing around the catheter. However, a large balloon increases the chance of contact between the balloon or catheter tip and the bladder wall, leading to bladder spasms that may cause urine to be forced out around the catheter.
A 30 mL balloon is used primarily to facilitate traction on the prostate gland to stop bleeding in men after prostate surgery or to stop bleeding in women after pelvic 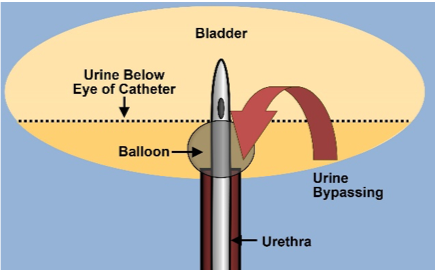 surgery.
surgery.
Routine use of larger capacity balloons (30 mL) should be avoided for long-term use as they can lead to bladder neck and urethral erosion.
Several catheter materials have been found to lose water from the inflated balloon over time in the bladder with 100% silicone catheters losing as much as 50% of their volume within 3 weeks.
In men, the catheter should be passed initially to the bifurcation (the “Y” junction where the balloon arm and catheter meet) to ensure that the balloon will not be inflated in the urethra.
Catheter Materials
A wide range of catheter materials are available, and the material selected should be chosen by:
- how long the catheter will remain in place,
- comfort,
- the presence of latex sensitivity,
- ease of insertion and removal, and
- ability to reduce the likelihood of complications such as urethral and bladder tissue damage, colonization of the catheter system by microorganisms, and encrustation
Note: Prior to insertion, all indwelling catheters should be visually inspected for any imperfections or surface deterioration.
1. Latex Catheter: The possibility of a latex allergy is an important consideration as many urinary catheters are constructed from latex or a related material.
There are reported increases in allergies and reactions in patients with long-term use of all urinary latex and rubber catheters. Patients who have asthma and other allergies are at increased risk for these allergies. Latex allergy can result in symptoms such as skin irritation, rashes, and blisters. Urethritis and urethral strictures can also result from latex allergies. Coatings such as silicone and polytetrafluoroethylene (PTFE) are used to coat latex catheters.
2. Hydrogel coating, which remains intact when used, has demonstrated the ability to reduce the high level of cytotoxicity associated with latex catheters. However, coated latex catheters do not protect against an allergic reaction to the underlying latex because the coating wears off.
Bonded hydrogel-coated latex catheters may be longer lasting than silicone catheters because their hydrogel coating prevents bacterial adherence and reduces mucosal friction. Hydrogels or polymers coat the catheter, absorbing water to produce a slippery outside surface. This results in the formation of a thin film of water on the contacting surface, thus improving its smoothness and lubricity. These properties might act as potential barriers to bacterial infection and reduce the adhesion of both gram-positive and gram-negative bacteria to catheters.
3. Silicone- and hydrogel-coated catheters usually last longer than PTFE-coated catheters. If the person is latex sensitive, silicone catheters should be used. Avoiding  latex catheters may also decrease the incidence of encrustation. All-silicone (100%) catheters are biocompatible and are believed to have encrustation-resistant properties. Silicone catheters are thin-walled, rigid catheters with a larger diameter drainage lumen.
latex catheters may also decrease the incidence of encrustation. All-silicone (100%) catheters are biocompatible and are believed to have encrustation-resistant properties. Silicone catheters are thin-walled, rigid catheters with a larger diameter drainage lumen.
4. Antimicrobial-coating: A major problem with Foley catheters is that they have a tendency to contribute to urinary tract infections (UTI). This occurs because bacteria can travel up the catheters to the bladder where the urine can become infected. In an attempt to prevent bacterial colonization, catheters have been coated with silver alloy or nitrofurazone, a nitrofurantoin-like drug.
This has been helpful, but it has not completely solved this major problem. An additional problem is that Foley catheters tend to become coated over time with a biofilm that can obstruct the drainage. This increases the amount of stagnant urine left in the bladder, which further contributes to the problem of urinary tract infections. When a Foley catheter becomes clogged, it must be flushed or replaced.
Both nitrofurazone-coated and silver alloy-coated catheters seem to reduce the development of asymptomatic bacteriuria during short-term (< 30 days) use.
Despite their unit cost, there is a suggestion that these devices might be a cost-effective option if overall numbers of infections are significantly reduced through their use.
- Antibiotic-coated catheters were found in a meta-analysis to prevent or delay bacteriuria in short-term catheterized, hospitalized patients. However, in 2012, nitrofurazone impregnated catheters were taken off the market.
- Silver is an antiseptic that inhibits growth of gram-positive and gram-negative bacteria. Silver alloy-coated catheters are thought to cause less inflammation and have a bacteriostatic effect because they reduce microbacterial adherence and migration of bacteria to the bladder.
Because they prevent bacterial adherence, these catheters also minimize biofilm formation through their release of silver ions that prevent bacteria from settling on the surface.
There appear to be few adverse effects, and microbial resistance to the active agent is unlikely.
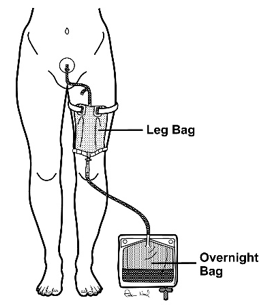 drainage bag, and a spare leg strap or a device to secure the catheter tubing to the leg. Drainage bags that cannot be worn and concealed are commonly referred to as “nighttime or overnight bags,” or “large capacity bags,” or “bedside bags”. Drainage bags that can be worn and concealed are commonly referred to as “leg bags” or abdominal bags, commonly referred to as “belly bags.” Leg bags generally hold 300- 900 cc whereas an overnight bag can hold up to 2000cc. It is recommended that reusable drainage bag be replaced every 30 days.
drainage bag, and a spare leg strap or a device to secure the catheter tubing to the leg. Drainage bags that cannot be worn and concealed are commonly referred to as “nighttime or overnight bags,” or “large capacity bags,” or “bedside bags”. Drainage bags that can be worn and concealed are commonly referred to as “leg bags” or abdominal bags, commonly referred to as “belly bags.” Leg bags generally hold 300- 900 cc whereas an overnight bag can hold up to 2000cc. It is recommended that reusable drainage bag be replaced every 30 days. The current design of urinary drainage bags prevents the introduction of bacteria into the closed indwelling urinary catheter system. There are anti-reflux bags, single use bags, closed urinary drainage systems, and bags with urine sampling ports. A leg bag cannot be characterized as closed because of the need to regularly open the leg bag for drainage and connect to an overnight drainage bag in most cases. To minimize opening of a catheter system, a leg bag can be attached to a larger bag for overnight drainage.
References:
1. Brosnahan J, A. Jull, et al. Types of urethral catheters for management of short-term voiding problems in hospitalized patients. Cochrane Database of Systematic Reviews, 2004, (1): CD004013.
2. Gray M. Does the construction material affect outcomes in long-term catheterization? JWOCN, 2006, 33: 116-121.
3. Lawrence EL. and IG. Turner. Materials for urinary catheters: A review of their history and development in the UK. Med Engineering Phys, 2005, 27: 443-453.
4. Leuck AM, Johnson JR, Hunt MA, Dhody K, Kazempour K, Ferrieri P, et al. Safety and efficacy of a novel silver-impregnated urinary catheter system for preventing catheter-associated bacteriuria: a pilot randomized clinical trial. Am J Infect Control. 2015;43:260-5. DOI: 10.1016/j.ajic.2014.11.021.
5. Newman D. The indwelling urinary catheter: Principles for best practice. JWOCN, 2007, 24: 655-661.
6. Pickard R, Lam T, MacLennan G, Starr K, Kilonzo M, McPherson G, et al. Antimicrobial catheters for reduction of symptomatic urinary tract infection in adults requiring short-term catheterisation in hospital: a multicentre randomised controlled trial. Lancet. 2012;380:1927-35. DOI: 10.1016/S0140-6736(12)61380-4.
7. Politano AD, Campbell KT, Rosenberger LH, Sawyer RG. Use of silver in the prevention and treatment of infections: silver review. Surg Infect (Larchmt). 2013;14:8-20. DOI: 10.1089/sur.2011.097.
8. Weissbart SJ, Kaschak CB, Newman DK. Urinary drainage bags. In: Newman DK, Rovner ES, Wein AJ, editors. Clinical Application of Urologic Catheters and Products. Switzerland: Springer International Publishing; 2018, 133-147.
9. Zugail AS, Pinar U, Irani J. Evaluation of pain and catheter-related bladder discomfort relative to balloon volumes of indwelling urinary catheters: A prospective study. Investig Clin Urol. 2019 Jan;60(1):35-39. doi: 10.4111/icu.2019.60.1.35. Epub 2018 Dec 6.