Active Surveillance Background
Prostate cancer represents a public health dilemma: while prostate cancer is the second leading cause of death among men in the US1 and third in Canada,2 it is widely over-diagnosed and over-treated, leading to significant patient anxiety and morbidity.3 Much of the over-diagnosis of prostate cancer relates to the use of serum prostate-specific antigen (PSA) testing for prostate cancer screening, beginning in 1987.4 Widespread adoption of PSA screening resulted in a significantly increased number of incident cases and a significantly reduced number of cases of metastatic disease at presentation.5 Coinciding with the introduction of PSA testing, prostate cancer mortality has decreased approximately 40% from an epidemiologic perspective.6 Approximately 45-70% of the decline in mortality is attributable to PSA-based prostate cancer screening.7
Thus, to preserve the survival benefits associated with PSA screening for prostate cancer while minimizing the morbidity of this approach, there is a need to de-couple prostate cancer diagnosis and treatment, particularly among men with low-risk disease.
Shortly after the widespread adoption of PSA-based prostate cancer screening, in 1995, Dr. Klotz and colleagues undertook a prospective clinical trial to evaluate a program of so-called “active surveillance” of patients with favorable-risk prostate cancer and some with intermediate-risk prostate cancer.8 Patients were followed with biochemical, clinical, and pathologic reassessment: patients underwent PSA testing every three months for two years followed by every six months in patients with stable disease. A confirmatory biopsy was performed in the first year following prostate cancer diagnosis and then every three to four years until the patient reach aged 80 years. Within the context of this trial, the decision to intervene with active treatment was based on reclassification according to PSA kinetics, histologic upgrading, or clinical stage progression.9 This protocol was initially offered to all patients with low risk disease (Gleason score less than or equal to 6 AND PSA less than or equal to 10 ng/mL) as well as patients over the age of 70 with PSA less than or equal to 15 ng/mL OR Gleason score less than or equal to 7 (3 + 4). From 2000 onwards, the cohort was restricted to patients with low risk disease and those with favourable intermediate risk disease (PSA 10 ng/mL to 20 ng/mL and/or Gleason score 3+4) who also had significant comorbidity and life expectancy less than 10 years.
Active Surveillance Outcomes
In results published in 2015, Klotz et al. reported outcomes of 993 men with low- or intermediate-risk prostate cancer who were managed with active surveillance.9 With a median follow-up of 6.4 years (range 0.2 years to 19.8 years), 149 (15%) patients died. As a result, overall survival was 80% at 10 years and 62% at 15 years. Of the 149 patients who died, only 15 (1.5%) deaths were due to prostate cancer. Thus, actuarial cause specific survival is 98.1% at 10 years and 94.3% at 15 years. In addition to the 15 men who died of prostate cancer, an additional 13 (1.3%) men developed metastatic disease. Of these, 9 men were alive with metastasis at the time of publication and 4 died of other causes. Overall, 267 (27%) of the 993 patients who began an active surveillance strategy converted to active treatment. As a result, at 15 years, 55% of men remained on active surveillance without treatment.
In an updated analysis, Musunuru et al. found that the risk of metastasis-free survival (hazard ratio 3.14, 95% CI 1.51 to 6.53) and prostate cancer specific survival were worse for patients with intermediate risk disease undergoing active surveillance compared to those with low risk disease.10 This appeared to be driven by tumor grade, rather than PSA: 15-year metastasis free survival was 94% in men with Gleason score 6 + PSA less than 10 ng/mL, 94% in men with Gleason score 6 + PSA 10 to 20 ng/mL, 84% in men with Gleason score 7 (3+4) + PSA less than 20 ng/mL, and 63% in men with Gleason score 7 (4+3) + PSA less than 20 ng/mL.
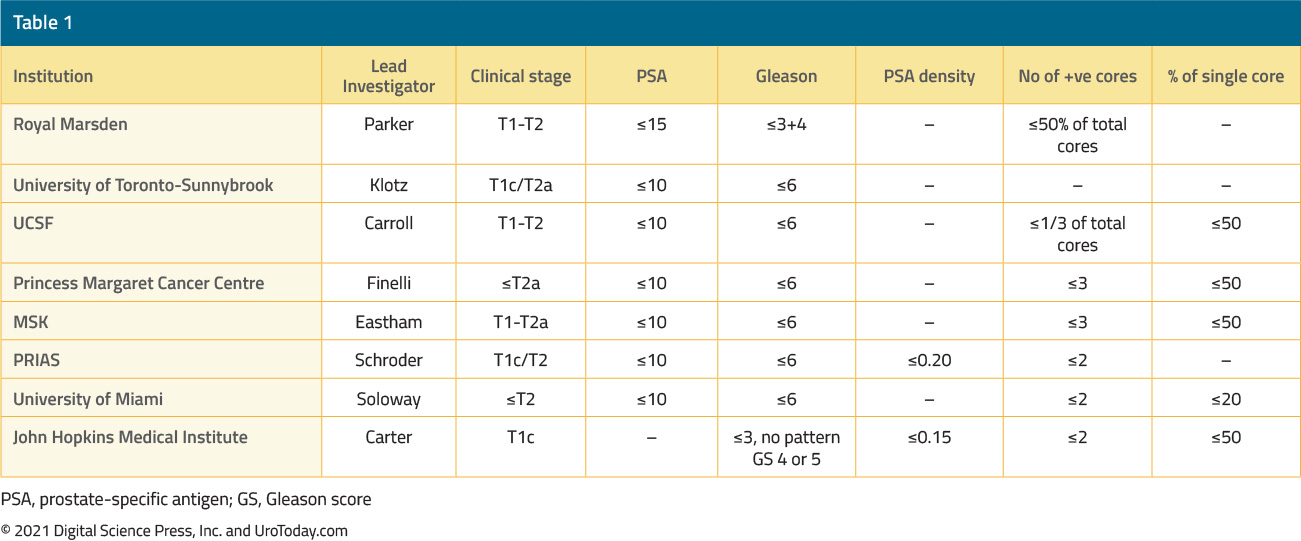
Many other institutions have adopted similar, but slightly different approaches to active surveillance in prostate cancer, including Johns Hopkins Medical Institute, the Royal Marsden, the University of California San Francisco, the Princess Margaret Cancer Centre, Memorial Sloan Kettering, the Prostate Cancer Research International Active Surveillance (PRIAS), and the University of Miami.11 Each of these differs in inclusion criteria as highlighted by the following table:11
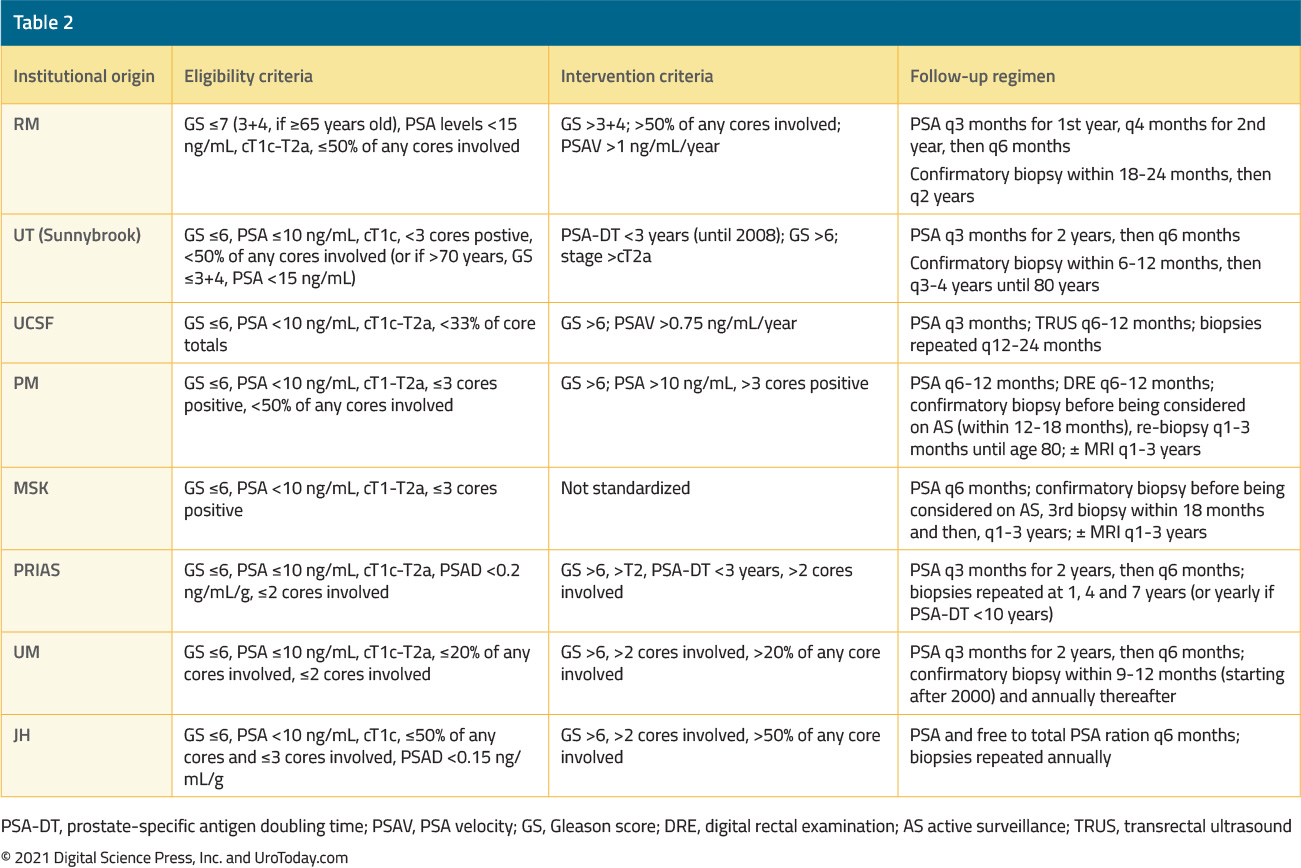
Beyond these institutional approaches, there are at least 16 published guidelines for the active surveillance of men with prostate cancer.11 As one may expect, differences in inclusion criteria and surveillance protocols may account for differences in prostate cancer progression risk observed between protocols.12 As follows is a summary of surveillance protocols followed by the major active surveillance institutions:11
Active Surveillance in Guidelines
While there remain many unanswered questions regarding the optimization of active surveillance, there is no question that this has become the preferred management option for patients diagnosed with low-risk prostate cancer. In December 2014, Cancer Care Ontario published guidelines on Active Surveillance for the Management of Localized Prostate Cancer (https://www.cancercareontario.ca/en/guidelines-advice/types-of-cancer/2286). These guidelines recommend that “For patients with low-risk (Gleason score less than or equal to 6) localized prostate cancer, active surveillance is the preferred disease management strategy” (emphasis added).13 These guidelines were subsequently endorsed by the American Society of Clinical Oncology (ASCO).14 In 2018, the European Association of Urology released a similar position statement recommending active surveillance for all men with low-risk prostate cancer.17
Among patients with very-low risk disease, the National Comprehensive Cancer Network (NCCN) had, for a number of years, recommended active surveillance as the “preferred” treatment approach among patients who had >20 year expected survival and as the only suggested treatment approach for those with life expectancy of 10 to 20 years (e.g NCCN Guidelines Version 2.2021).
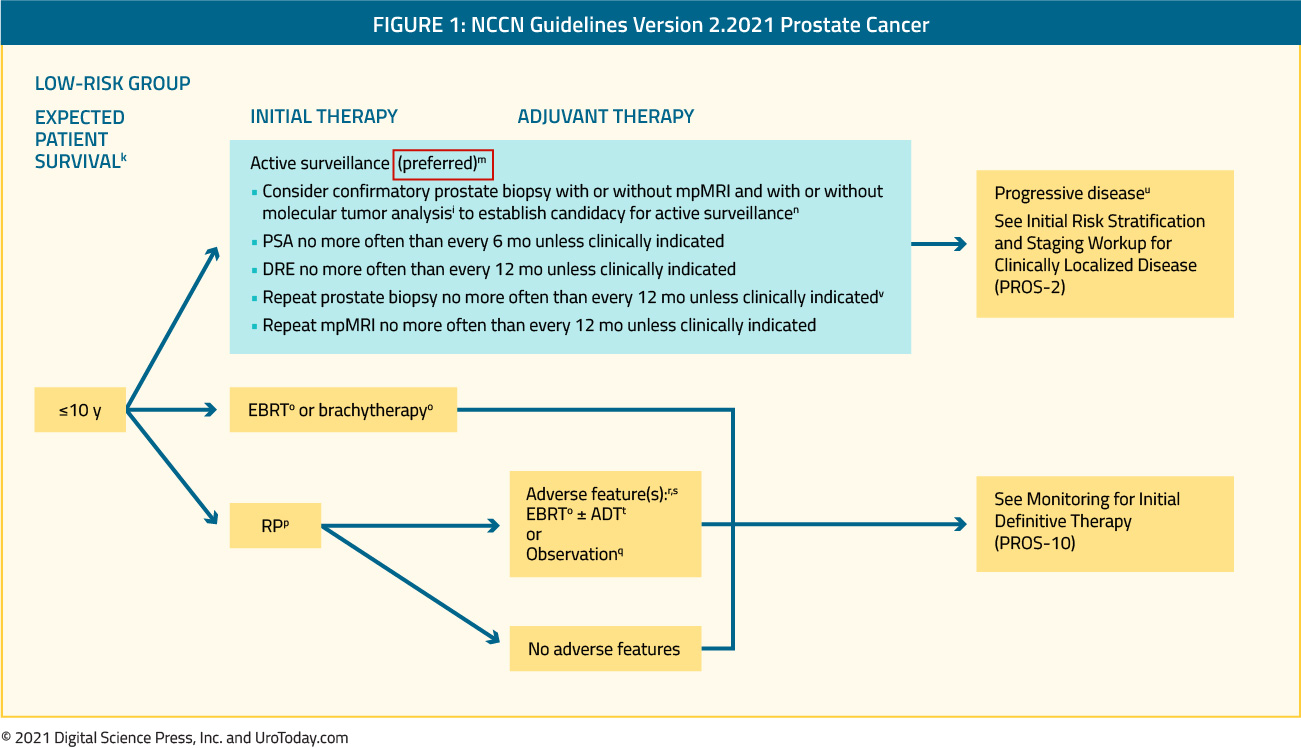
Similarly, among patients with low-risk disease, active surveillance was recommended as the “preferred” approach for patients with 10 years or greater life expectancy and, among patients with favourable intermediate risk disease, as a treatment consideration.
Active Surveillance Uptake in the US
As a result of increasing awareness and acceptance of the role of active surveillance over time, its utilization rose. Utilizing data from the Cancer of the Prostate Strategic Urologic Research Endeavour (CaPSURE) registry, Cooperberg and Carroll assessed trends in the management of patients diagnosed with localized prostate cancer among 45 urology practices in the United States.15 Among patients with low risk prostate cancer (CAPRA score 0-2), the use of active surveillance or watchful waiting was uncommon from 1990 to 2009 (ranging from 6.7% to 14.3%). However, in the most recent time interval examined (2010-2013), rates of active surveillance increased significantly to 40% (p-value for trend <0.001). Interestingly, despite overall favorable trends in the uptake of active surveillance, rates at individual urology practices varied widely (8% to 64%; median 36%; interquartile range 13% to 54%). It is encouraging to see that in the Veterans Affairs medical system, active surveillance uptake has increased: conservative management increased among men younger than 65 years (27% in 2005 to 72% in 2015) and 65 years or older (35% in 2005 to 79% in 2015).16
Widespread adoption of active surveillance is one of the reasons cited for the revision of the United States Preventative Services Task Force (USPSTF) recommendation regarding PSA-based prostate cancer screening from “D” (not recommended) to “C” (neutral).
The NCCN Controversy
Thus, when the 2022 version of the NCCN Clinical Practice Guidelines in Oncology were released on September 10, 2021, it was to the consternation of many urologists and key opinion leaders that active surveillance was no longer cited as a “preferred” treatment approach for patients with low-risk disease and 10 years or greater life expectancy, though it retained this recommendation among those with very-low risk disease and 20 years expected survival.
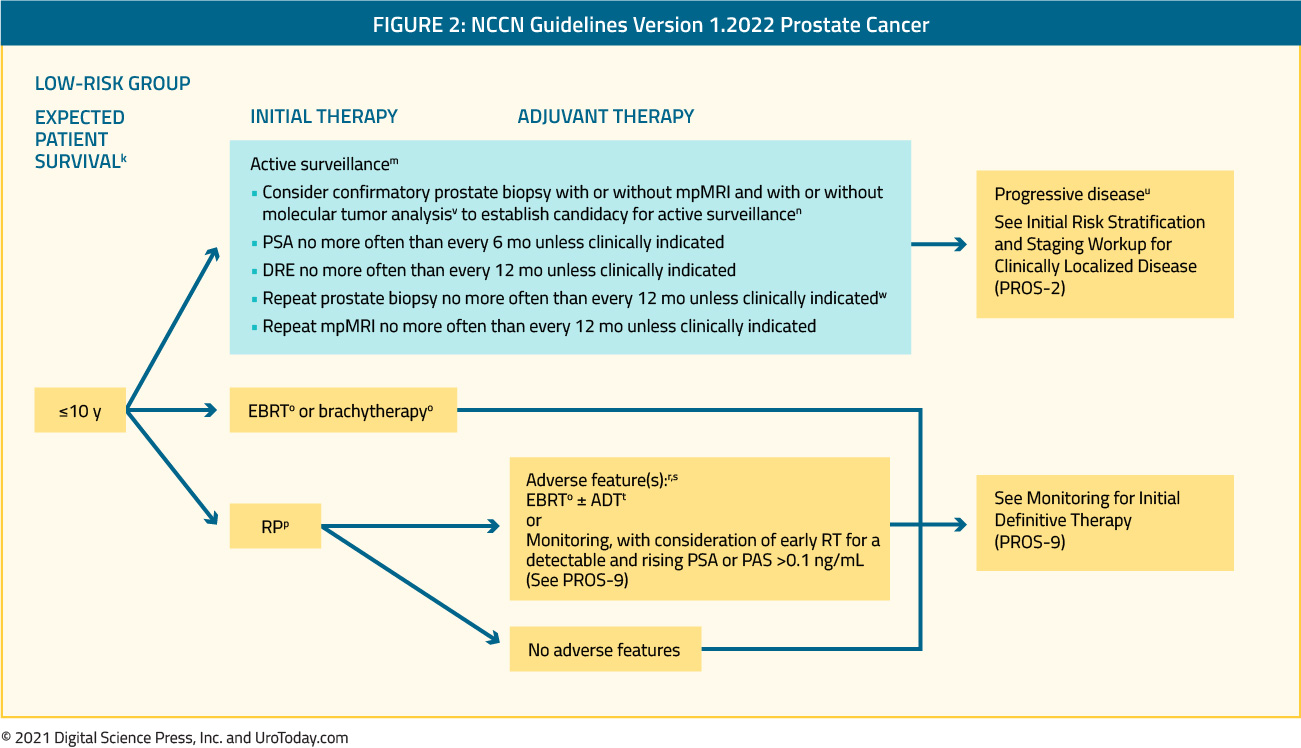
Relatively swiftly, on November 30, 2021, an updated (version 2.2022) of the NCCN guidelines were released which suggested that, for patients with low-risk disease and an expected survival of 10 years or more, active surveillance was “preferred for most patients”.
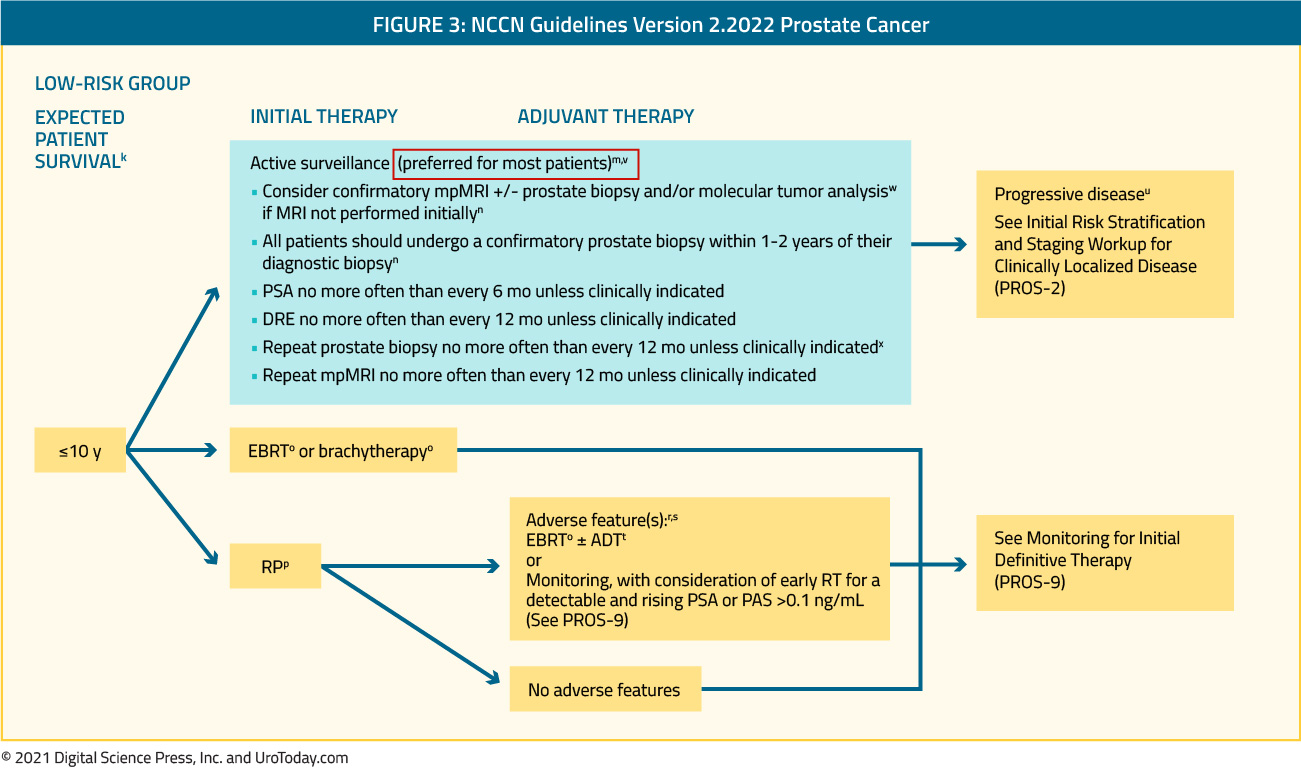
In the updated version 2.2022 of the guidelines, the panel noted that, among patients with low-risk disease, there is substantial heterogeneity between individuals with respect to the probability of disease progression or early grade reclassification. In particular, the panel highlighted high PSA density, a high number of involved cores (3 or greater), a high genomic risk (on the basis of tissue-based molecular tumor assays), or known BRCA2 germline mutations as factors that may warrant upfront treatment, in the context of shared decision making. The panel further emphasized that, for patients opting for surveillance, confirmatory biopsy within 1-2 years of diagnosis should be recommended.
The ability of active surveillance to “de-couple” prostate cancer diagnosis and prostate cancer treatment offers the real opportunity to maximize the benefit of prostate cancer screening. In response to feedback from the genitourinary oncology community, the NCCN guidelines panel rapidly reaffirmed the key role that active surveillance holds in the management of patients with low-risk disease.
Published Date: December 2021