Introduction
In December 2020, Gallium 68 PSMA-11 (68Ga PSMA-11) was approved by the U.S. Food and Drug Administration (FDA) for the initial staging of prostate cancer patients at high risk of metastases,1 and this was shortly followed by the FDA approval of 18F-DCFPyL (PYLARIFY®) in May 2021.2 These positron emission tomography (PET) imaging modalities have since been endorsed by numerous international guidelines and have been widely adopted in clinical practice for the primary staging of unfavorable intermediate- and high-risk prostate cancer patients.There are, however, some limitations to the use of these radiotracers in clinical practice. These agents have short half-lives (68Ga: 68 mins;18F-DCFPyl: 110 mins) that limit their product shelf life (68Ga: 4 hours;18F-DCFPyl: 10 hours) and imaging windows (68Ga: 50–100 mins;18F-DCFPyl: 60–90 mins). They also have limited sensitivities for detecting lymph node metastases <5 mm in size.3 Notably, neither 68Ga PSMA-11 nor 18F-DCFPyL can be radiolabeled with an α or β emitter for theranostic purposes. Accordingly, there has been significant interest in developing novel radiotracers to overcome these practical limitations and enhance the diagnostic performance of PET imaging modalities.
In this Center of Excellence article, we will discuss new radiotracers for the primary staging of prostate cancer patients.
Flotufolastat F 18 (POSLUMA®)
Flotufolastat F 18 is an optimized, high-affinity radiohybrid (rh) PSMA-targeted PET imaging agent that has the potential to overcome some of the limitations of other approved tracers in this space. Radiohybrid PSMA ligands are a novel class of compounds that can be efficiently labeled with 18F or with radioactive metal isotopes and, consequently offer both diagnostic and therapeutic PSMA targeting.4 Flotufolastat F 18 demonstrates high PSMA binding affinity, high internalization by PSMA-expressing cells, medium-to-low lipophilicity, and high human serum albumin binding, which together can provide optimal kidney clearance.5-7On May 30, 2023, the U.S. FDA approved POSLUMA® (flotufolastat F 18) injection, formerly referred to as 18F-rhPSMA-7.3, as a PSMA-PET/CT tracer for the initial staging of prostate cancer patients who are candidates for initial definitive therapy, based on the results of the phase 3 LIGHTHOUSE trial.8
LIGHTHOUSE
LIGHTHOUSE (NCT04186819) was an open-label, single arm, prospective phase 3 trial that included patients with unfavorable intermediate-, high-, and very high-risk prostate cancer planned for a radical prostatectomy with pelvic lymph node dissection at one of 31 sites across the USA and Europe. All patients received standard-of-care imaging (bone scan, abdominal/pelvic CT or MRI, or chest CT as per institutional preference) as part of the baseline assessment at least 24 hours before their flotufolastat F 18 PET/CT.
All images were initially evaluated by study site-based readers to determine whether N1 or M1 disease was detected on PET imaging and to inform subsequent standard-of-truth activities. For the evaluation of study endpoints, all flotufolastat F 18 PET/CT images were interpreted by three expert, independent central PET readers who were blinded to all clinical information, including the local site conventional imaging and PET reads, and received specific training on interpreting flotufolastat F 18 PET/CT images.
The standard of truth was histopathology from surgically removed lymphatic tissue. For suspected M1 lesions, histopathology, or confirmatory conventional imaging (CT, bone scan, or MRI) was used. The coprimary endpoints were patient-level sensitivity and specificity of flotufolastat F 18 PET/CT for the detection of pelvic nodal metastases. Prespecified statistical thresholds (lower bounds of 95% CI) were set at 22.5% for sensitivity and 82.5% for specificity, based on the low sensitivity but high specificity of other PSMA-PET ligands used for nodal staging.
The study cohort included 296 patients in the efficacy population (352 in the extended population for M1 efficacy). The median PSA was 8.5 ng/ml, and 33% of patients had unfavorable intermediate-risk disease. As per the independent reads, 7.8–13% of patients had flotufolastat F 18 PET/CT-positive pelvic lymph nodes. Conversely, on histopathology, 24% of patients had positive pelvic lymph nodes.
The patient-level sensitivity among the efficacy population ranged across the three readers between 23% and 30% (majority read: 24%). The lower bound 95% CI ranged from 13.7% to 19.6%, not exceeding the prespecified statistical threshold of 22.5% (p = 0.09–0.50). Among patients with high- or very high-risk disease only, the sensitivity ranged between 24% and 44% (majority read: 27%). Notably, the sensitivity of flotufolastat F 18 PET/CT by the underlying size of the involved pelvic lymph node was not examined.
With regards to specificity, the patient-level specificity ranged between 93% and 97% (majority read: 96%). The lower bound 95% CI ranged between 88.8% and 93.7%, exceeding the prespecified statistical threshold for all three readers (p < 0.001) and, thus, meeting this co-primary endpoint. The patient-level positive predictive and negative predictive values ranged between 57–70% and 80–81%, respectively.
Extra-pelvic M1 lesions were detected in 16–28% of patients. Using predominantly confirmatory conventional imaging as the gold standard, the verified detection rate was 10–14%. No new safety signals were identified, and there were no serious treatment-emergent adverse events.9
Framing These Results in Context of Other PSMA Registration Trials
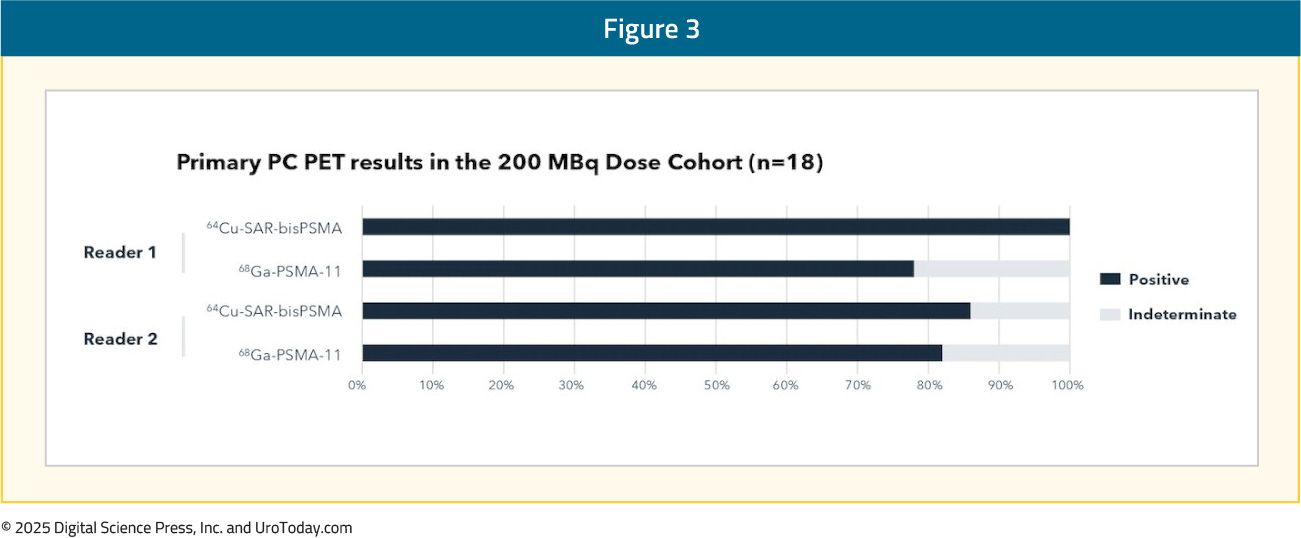
A direct comparison of the results of LIGHTHOUSE to other registrational trials, including OSPREY and 68Ga-PSMA-11, is limited by important differences in the cohort characteristics.10,11 OSPREY recruited only high-risk patients, and the 68Ga-PSMA-11 trial cohort included only 18% with unfavorable intermediate risk disease. While the percentage of patients with pathologic nodal involvement is similar across all three trials (24-27%), lower-risk patients may have smaller micrometastatic nodal deposits expressing lower levels of PSMA that are less likely to be identified on PSMA PET/CT.
Summarized in the table below is the individual performance characteristics of the three PSMA PET/CT radiotracers for the primary staging of prostate cancer patients from the three registrational trials to date. Caution should be applied in drawing comparisons based on individual trial data secondary to the impact that differing patient populations, scanning procedures, readers, and the differences in standard of truth protocols have on reported outcomes.
Inter- and Intra-reader Reproducibility of Flotufolastat F 18 PSMA PET/CT in Newly Diagnosed Prostate Cancer Patients
A follow-up analysis of the LIGHTHOUSE trial demonstrated that Flotufolastat F 18 PSMA PET/CT scans can be reliably interpreted, with a high degree of inter- and intra-reader agreement observed across three blinded readers given the same set of scans and having completed identical training. The inter- and intra-reader agreements (≥4 weeks apart) were ≥95% overall at the patient level. On a regional basis, the agreement was ≥81% across the pair‑wise inter‑reader comparisons for all regions, and highest in the prostate region.12
64Cu-SAR-bisPSMA
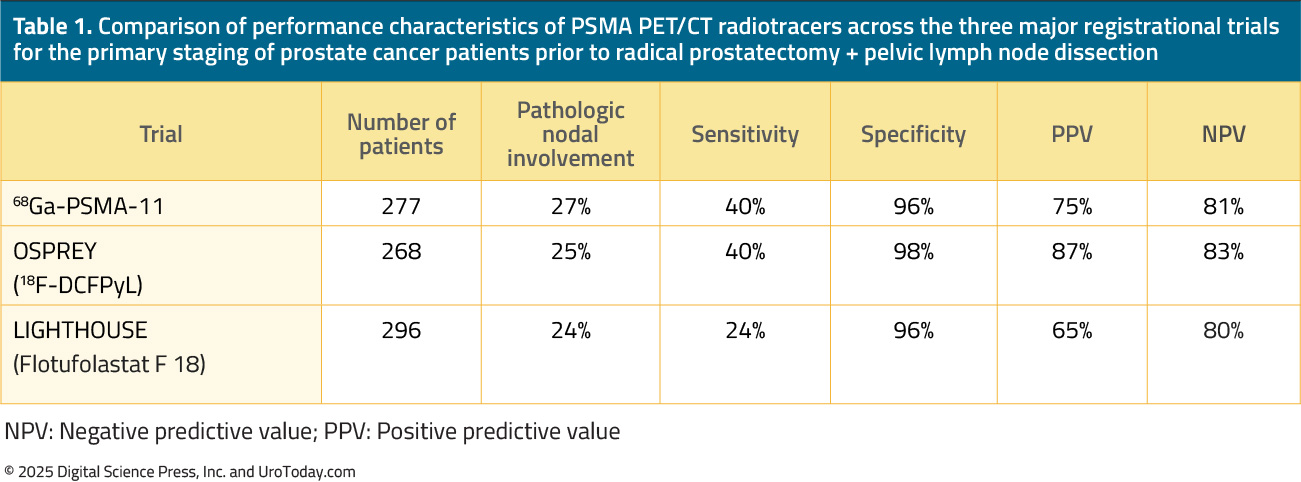
64Cu-SAR-bisPSMA is a next generation theranostic radiopharmaceutical developed by Clarity Pharmaceuticals. It utilises copper isotopes for imaging (64Cu) and therapy (67Cu). The targeting moiety, linked to a SAR chelator, has two PSMA-targeting functional groups, which exhibit increased tumor uptake and retention.
64Cu has a long half-life of 12.7 hours, compared to 1.1 and 1.83 hours for 68Ga and 18F radiotracers, respectively. This allows for a much longer product shelf life (up to 48 hours versus 4 and 10 hours for 68Ga and 18F, respectively) and imaging windows (1–30 hours versus 50–100 and 60–90 mins for 68Ga and 18F, respectively). Additionally, 64Cu has a shorter positron range (0.56 mm), leading to improved scan resolution.
PROPELLER: Phase I Trial in the Primary Staging Setting
PROPELLER (NCT04839367) was a prospective, phase I, multi-center, blinded review, dose-ranging study that evaluated the safety and preliminary efficacy of 64Cu-SAR-bisPSMA PET in patients with known primary prostate cancer, initially presented at ASCO 2023. The study objectives were to determine the:
- Safety and tolerability of 64Cu-SAR-bisPSMA
- Ability of 64Cu-SAR-bisPSMA PET to detect primary prostate cancer
- Image quality at 100 MBq, 150 MBq and 200 MBq dosages of 64Cu-SAR-bisPSMA
- How 64Cu-SAR-bisPSMA compares to 68Ga-PSMA-11 PET
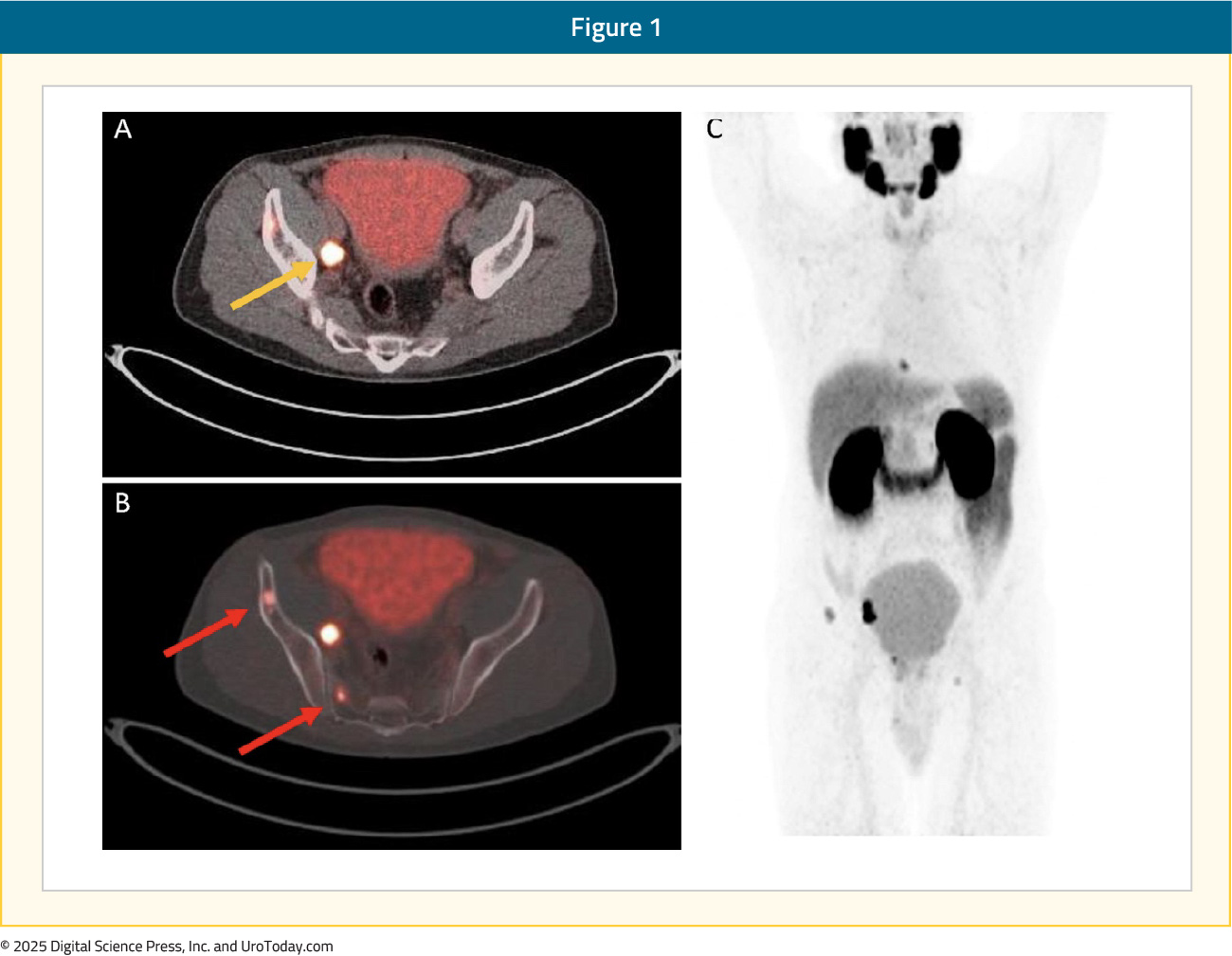
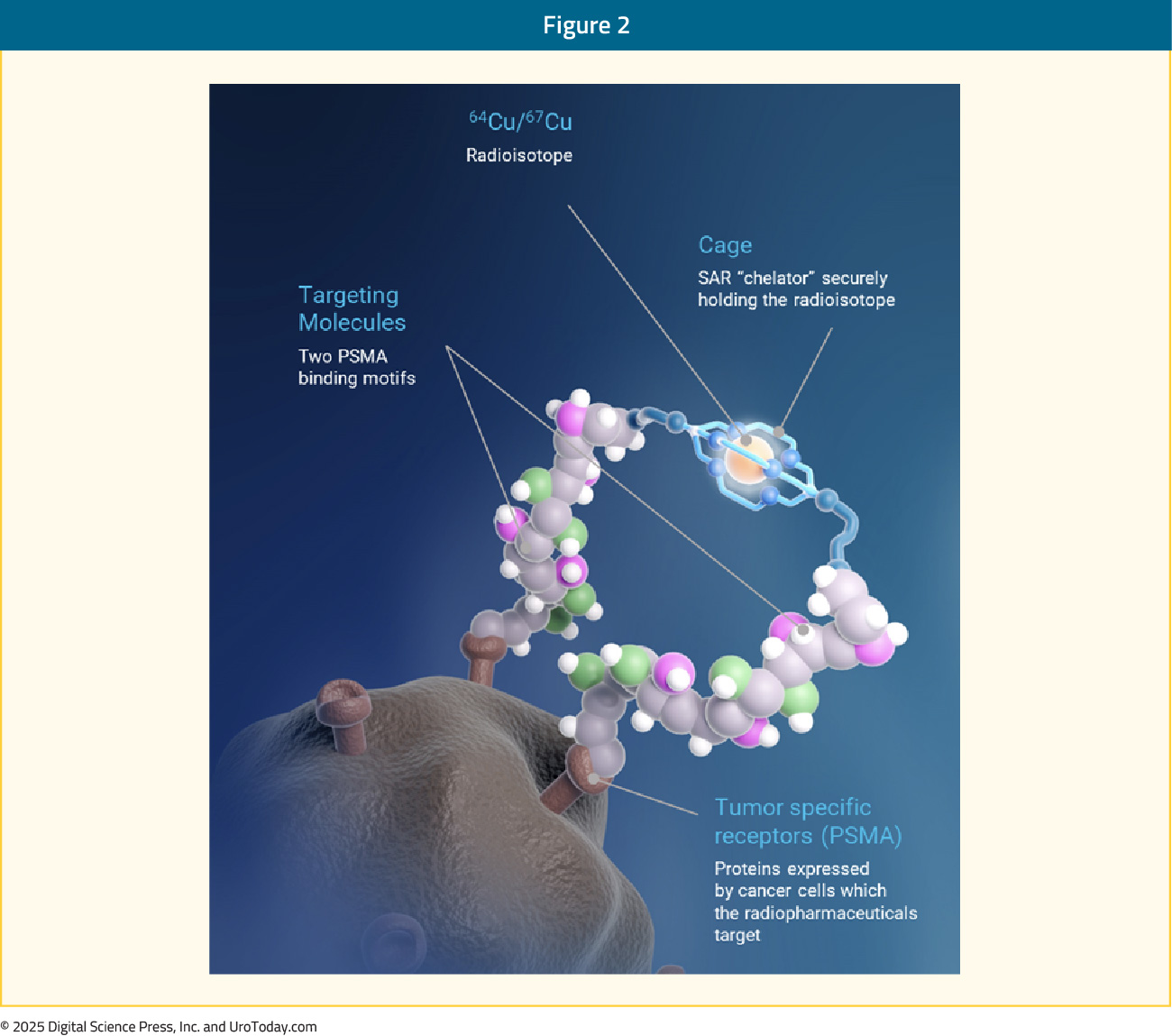
From a safety standpoint, there was one grade 1 64Cu-SAR-bisPSMA-related adverse event reported in the 200 MBq cohort. For image quality, both readers scored 200 MBq of 64Cu-SAR-bisPSMA as the dose providing the highest image quality. In the 200 MBq cohort, 64Cu-SAR-bisPSMA and 68Ga-PSMA-11 were able to detect primary prostate cancer in 100% and 77.8% of patients for Reader 1 and 85.7% and 83.3% of patients for Reader 2, respectively:
Concordant lesions on 64Cu-SAR-bisPSMA and 68Ga-PSMA-11 PET/CT exhibited 2.5–3 fold higher uptake on 64Cu-SAR-bisPSMA compared to 68Ga-PSMA-11 for all parameters assessed:
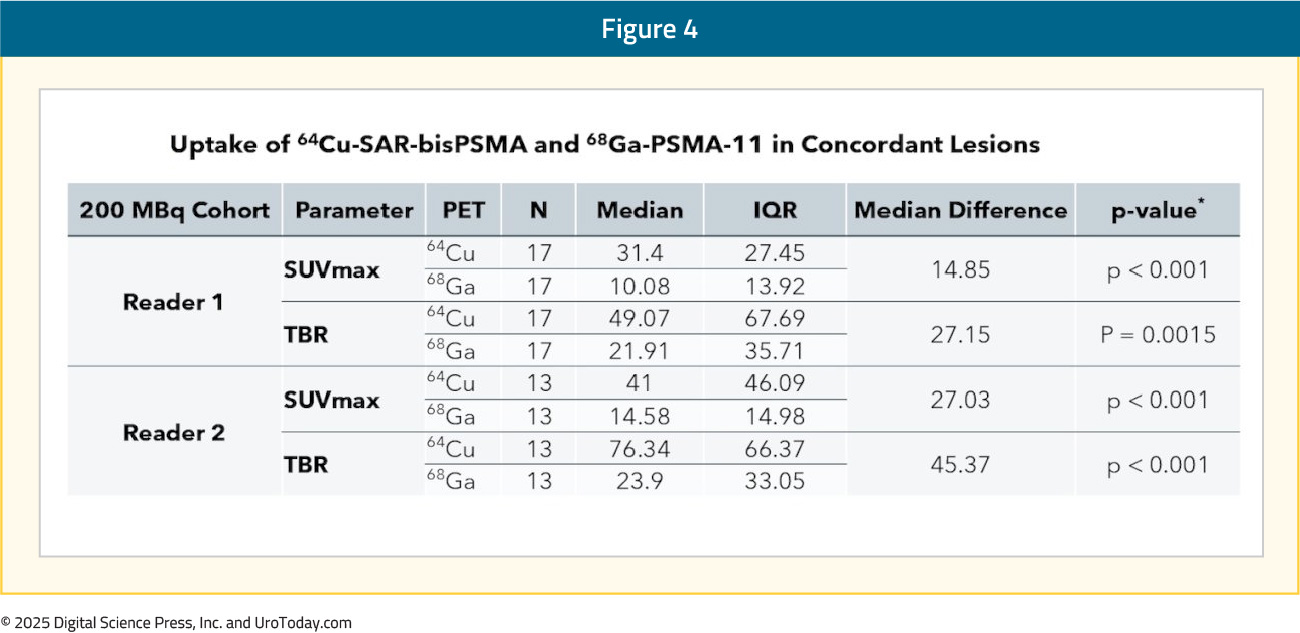
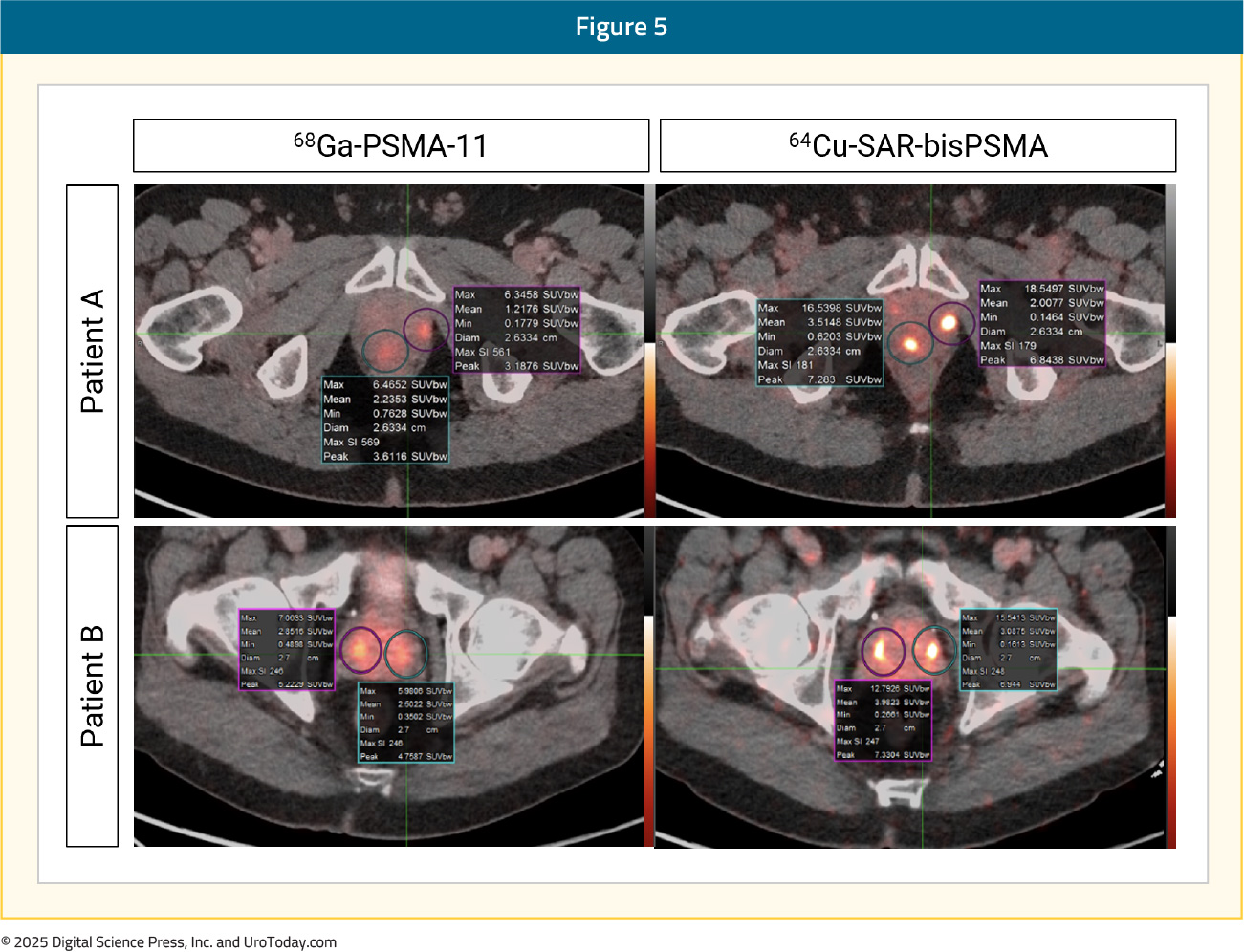
With regards to number of lesions detected, readers 1 and 2 noted that 64Cu-SAR-bisPSMA was able to detect more lesions in 39% and 43% of patients, respectively. Conversely, 68Ga-PSMA-11 PET/CT was able to detect more lesions in 22% and 14% of patients, respectively. The median number of lesions detected per patient were two and one for 64Cu-SAR-bisPSMA and 68Ga-PSMA-11 PET/CT, respectively. Additionally, lesions detected on 64Cu-SAR-bisPSMA demonstrated higher median SUVmax (31–41 versus 10–15) and higher tumor-to-background ratios (49–76 versus 22–24).13
Overall, this phase I trial demonstrated that 64Cu-SAR-bisPSMA was safe and effective for detecting PSMA-expressing lesions, with 200 MBq of 64Cu-SAR-bisPSMA determined as the optimal dose for future trials. 64Cu-SAR-bisPSMA PET/CT detected a greater number of lesions, and lesions exhibited significantly higher uptake when compared to 68Ga-PSMA-11 in men with intermediate- to high-risk prostate cancer.
CLARIFY: Ongoing Phase III Trial in Primary Setting
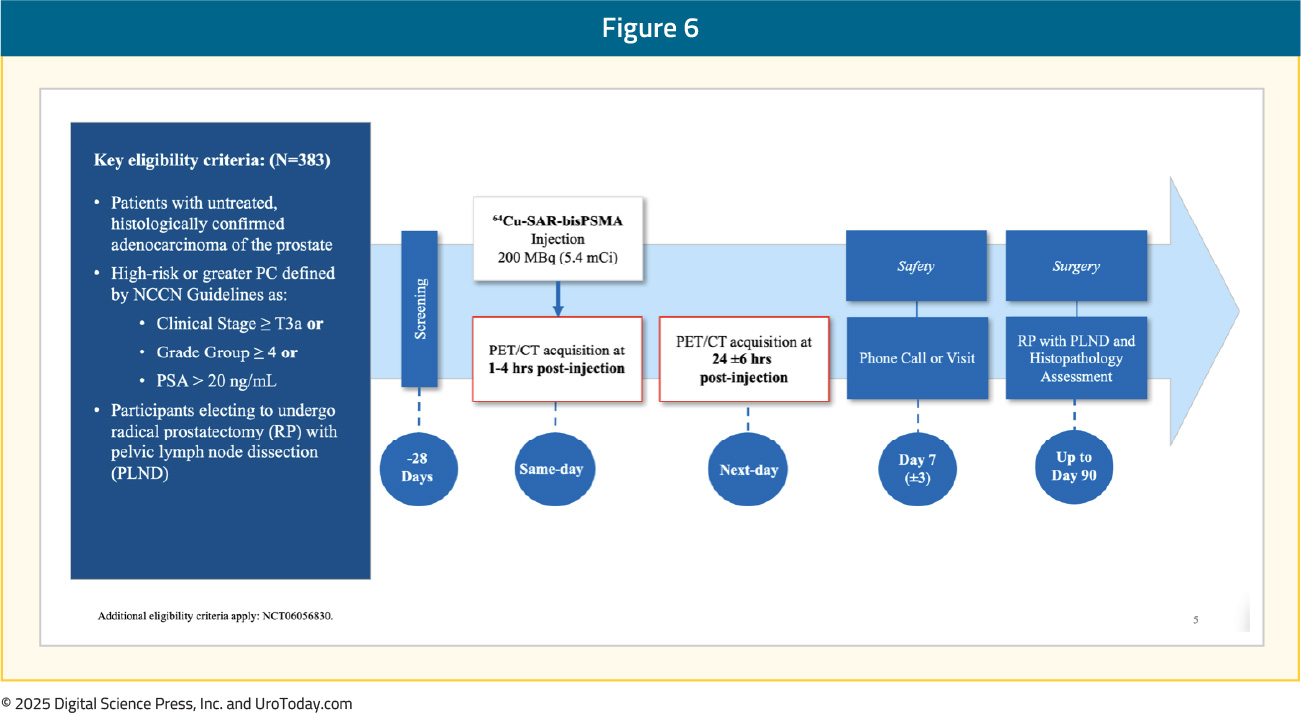
CLARIFY (NCT06056830) is an open-label, multicenter, single arm phase III trial of 64Cu-SAR-bisPSMA in the primary staging setting for patients with high-risk prostate cancer planned for a radical prostatectomy with pelvic lymph node dissection (n = 383).14
Eligible patients will receive a single administration of 64Cu-SAR-bisPSMA (200 MBg) followed by a PET/CT scan on Day 1 (1–4 hours post-dose) and on Day 2 (24 +/- 6 hours post-dose). Patients will be assessed for safety and then proceed to the radical prostatectomy with a pelvic lymph node dissection. The standard-of-truth reference will be the histopathology from the surgical specimen. The study design is as follows:
The Day 1 and Day 2 64Cu-SAR-bisPSMA PET/CT scans will be interpreted locally and by three independent blinded central readers. The diagnostic performance of 64Cu-SAR-bisPSMA will be based on the scan result for each respective day independently (Day 1 and 2) matched against the standard of truth.
The primary objective is to assess the diagnostic performance (sensitivity and specificity) of 64Cu-SAR-bisPSMA PET for the detection of regional nodal metastases, assessed independently for Days 1 and 2. The key secondary objectives are:
- To assess the consistency of 64Cu-SAR-bisPSMA PET/CT interpretations for the three central readers
- To assess the positive and negative predictive values of 64Cu-SAR-bisPSMA PET for pelvic nodal disease
- To assess the ability of 64Cu-SAR bisPSMA PET to detect prostate cancer (all regions)
- To assess the ability of 64Cu-SAR bisPSMA PET to detect primary prostate cancer
- To assess the diagnostic performance of 64Cu-SAR bisPSMA PET to detect regional nodal metastases without subregion matching
Conclusions
Following the regulatory approvals of 68Ga PSMA-11 and 18F-DCFPyL in 2020 and 2021, respectively, a third radiotracer, Flotufolastat F 18 (POSLUMA®), was approved by the US FDA in May 2023. While this radiotracer did not demonstrate improved sensitivity for detecting pelvic nodal metastases, compared to 68Ga PSMA-11 and 18F-DCFPyL, it does offer the theranostic potential of radiolabeling with a radioemitter.64Cu-SAR-bisPSMA is a promising radiotracer in this space that offers many practical advantages with its significantly longer half-life allowing for longer product shelf lives and imaging windows, which may have important economic and operational advantages, 64Cu also has a shorter positron range (0.56 mm), leading to potentially improved scan resolution. Initial phase I data appears promising for this radiotracer, with an ongoing phase III trial evaluating 64Cu-SAR-bisPSMA in the primary setting (CLARIFY).
Published January 2025