Prostate-specific membrane antigen (PSMA) is a type II transmembrane glycoprotein which functions as a zinc metalloenzyme and is found on prostatic epithelium. In normal prostate tissue, PSMA expression and localization focuses on the cytoplasm and apical side of the epithelium surrounding prostatic ducts. However, during prostate carcinogenesis, PSMA is transferred to the luminal surface of the ducts.
PSMA is highly expressed (100-1000 fold normal) in the vast majority of prostate cancer cells, including in patients with advanced disease, in those with castration-resistant disease, and in those with poorly differentiated disease. Further, PSMA has a high internalization rate into prostate cancer cells. 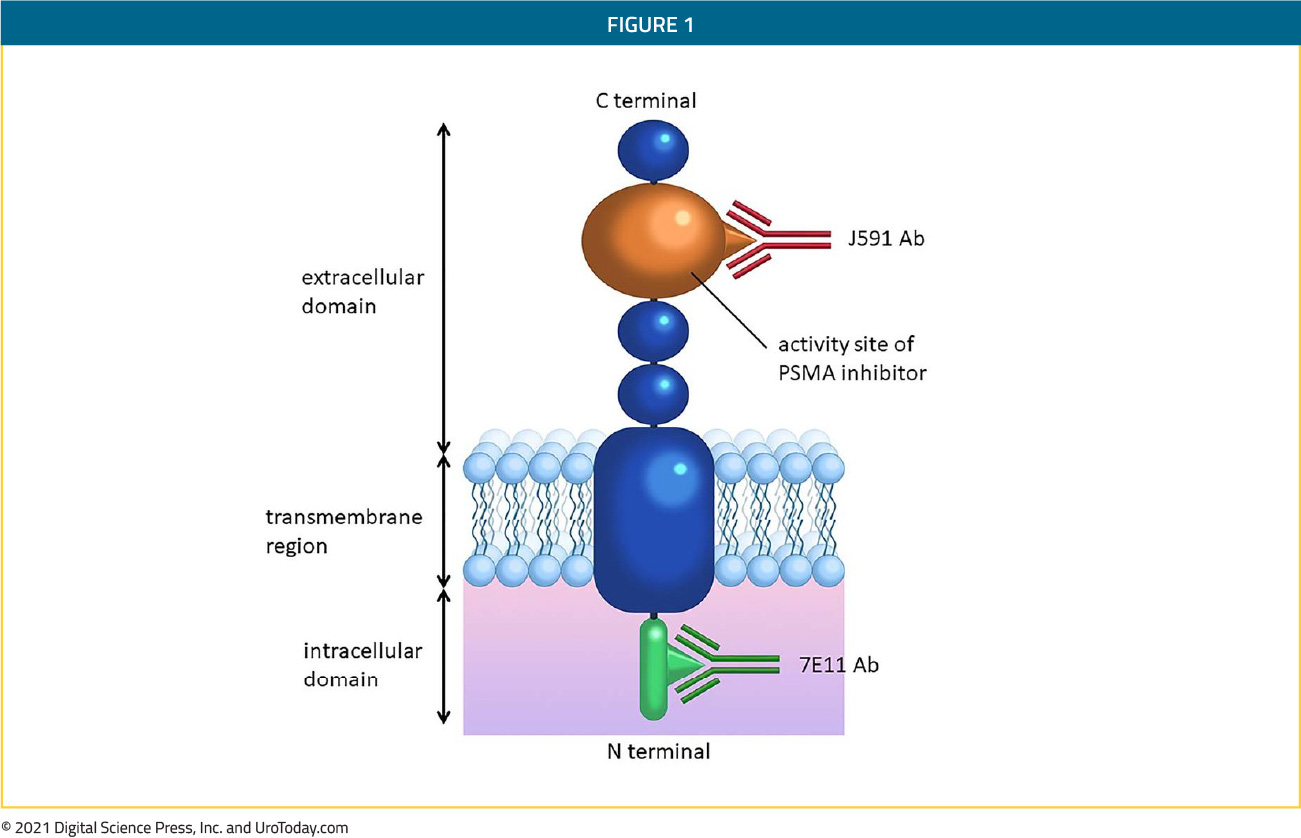
Due to its ubiquity in prostate cancer, as well as the features described above, PSMA has become an appealing target for investigations for imaging modalities and therapeutics in patients with prostate cancer with utility in the initial staging of patients, characterization of disease heterogeneity, detection of recurrence, response monitoring, and theranostic intervention. PSMA based approaches may also allow some degree of prognostication as the ratio of PSMA to its truncated isoform (PSM’) is proportion to tumor aggressivity.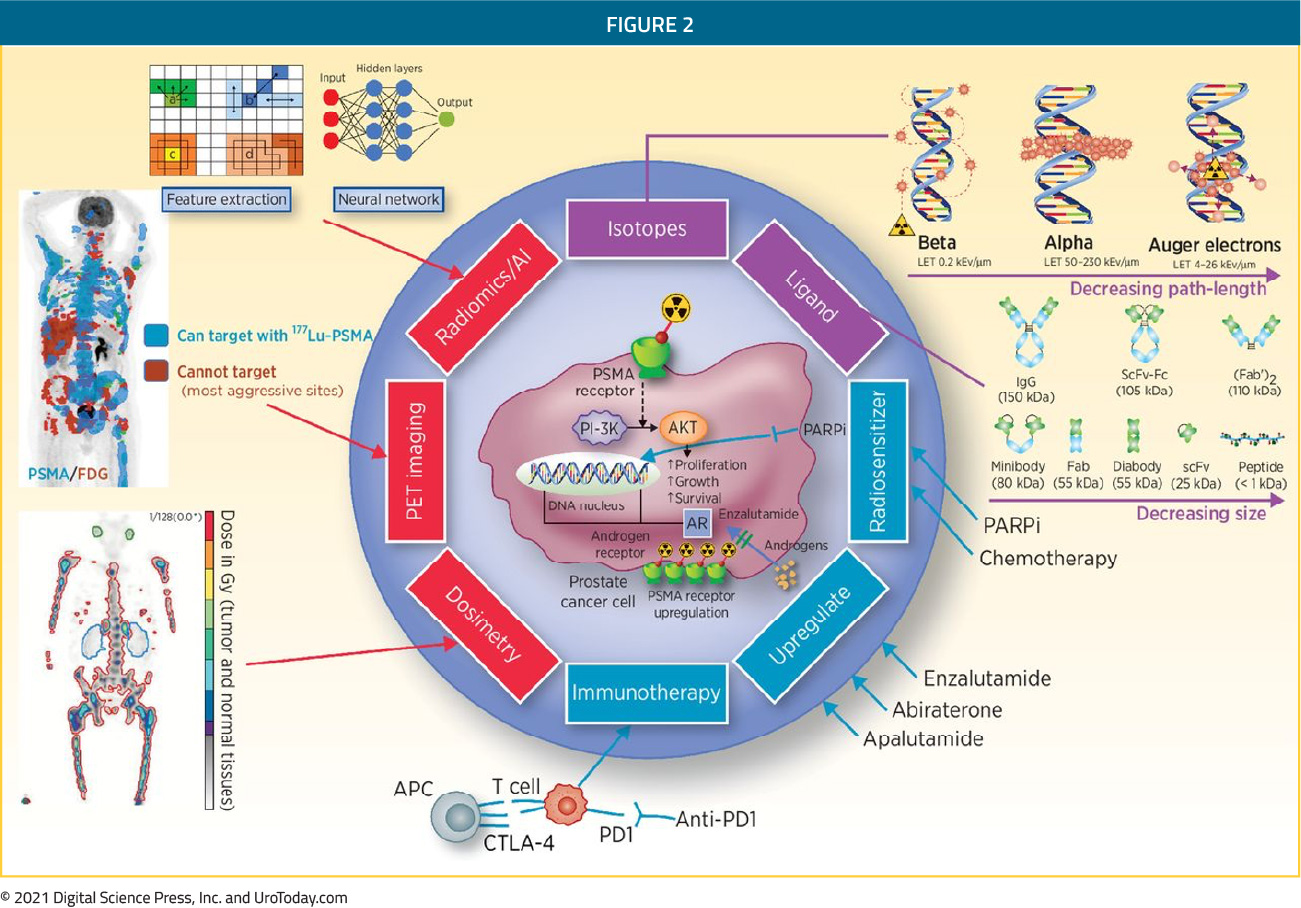
PSMA as a target for diagnostic imaging
An accurate assessment of the extent of disease (staging) is critical to the care of patients with cancer, across the natural history of disease including initial evaluation, following local treatment, and assessing response to systemic therapy.
Initially, radiographic diagnosis of bony prostate cancer metastasis was made on the basis of plain radiographs. However, this approach is limited as extensive bone mineral loss (exceeding 30-50%) may be required before such changes are radiographically apparent1. Following plain projectional radiography, skeletal scintigraphy was the next imaging modality widely adopted for the assessment of bony metastases in patients with prostate cancer. To date, it remains widely utilized and is currently recommended, along with abdominal and pelvic computed tomography, for the staging of patients according to many guideline bodies. Skeletal scintigraphy, when performed in patients with known cancer in the absence of bony pain, has a sensitivity of 86% and specificity of 81% for the detection of metastatic lesions1. As with any imaging modality, these characteristics differ somewhat on the basis of the patient population being tested (i.e. the pre-test probability or population-based disease prevalence). Among patients with prostate cancer, PSA levels are predictive of the likelihood of positive bone scan. Across a number of different cancers, Yang et al. found that bone scintigraphy had a specificity of 81.4% and sensitivity of 86.0%, on a per patient basis, for the detection of bony metastases2. In addition to bone scan, computed tomography has been utilized for the assessment of nodal metastatic disease, visceral disease, and bony metastasis. CT is highly sensitive for both osteoblastic tumors (such as prostate cancer) and osteolytic lesions in the cortical bone but is less sensitive in tumors that are restricted to the marrow space1. As a result, CT is of relatively limited utility as a screening test for bony metastasis due to a relatively low sensitivity (73%) despite excellent specificity (95%) – numbers based on a large scale meta-analysis from Yang and colleagues2. For this reason, conventional staging recommendations for patients with prostate cancer include bony scintigraphy for the detection of bony lesions along with computed tomography for identification of nodal/visceral lesions and correlation of any bony lesions3. Multiparametric magnetic resonance imaging (mpMRI) may also assist with evaluation for distant metastatic disease, including, for example, assessment of local/regional nodal involvement including obturator and external iliac nodal chains on routine pelvic/prostate MRI. Abdominal/pelvic or whole body MRI may also be useful as a staging modality but is not widely adopted.
Moving from anatomic to functional based imaging, traditional positron emission tomography (PET) imaging utilizing fluorodeoxyglucose (FDG) is not typically effective in the initial diagnosis of prostate cancer metastasis owing to the relatively low metabolic activity associated with the disease. However, at least four other PET imaging approaches have been assessed and employed in patients with prostate cancer including 18F-NaF PET/CT, choline-based PET/CT, fluciclovine (Axumin) PET/CT, and PSMA-targeted PET/CT4. While clearly improved compared to bony scintigraphy, the limitations are similar – namely, that sensitivity is highly dependent on PSA levels. While fluciclovine-PET/CT demonstrated lower false negatives and false positive rates in patients with biochemical recurrence compared to choline-PET/CT5,6, it has proven to be inferior to 68Ga-PSMA-PET/CT in the detection of metastatic disease (13% vs 56%) (56%) compared with fluciclovine-PET/CT (13%) in patients with biochemical recurrence following radical prostatectomy7. PSMA-based PET/CT demonstrated particular benefit in the evaluation of patients with low absolute PSA levels.
Thus, PSMA-based molecularly targeted imaging likely represents the way forward in prostate cancer diagnostics. While the most well examined PSMA based approach is 68Ga-PSMA-PET/CT, other radiotracers including 18F-DCFPyL and 177Lu-PSMA-617 have recently been examined in place of 68Ga-PSMA8 and recent work has also assessed the role of PET/MRI, rather than PET/CT. This approach leverages the advantages of the sensitivity of receptor targeted imaging and the spatial resolution of MRI9.
The role of PSMA-based imaging in prostate cancer
While there have been innumerable studies of the role of PSMA-based molecular imaging in prostate cancer, three warrant particular mention and will be discussed here.
First, assessing the role of PSMA-PET/CT in the initial staging is the proPSMA study, which was published in the Lancet10 and presented at the EAU 2020 Annual Meeting. This was a multi-center, two-arm randomized controlled trial among men with histologically confirmed prostate cancer who were being considered for curative intent radical prostatectomy or radiotherapy. To be eligible for inclusion, men must have had at least one high-risk factor including PSA greater than or equal to 20 ng/mL, ISUP grade group 3-5, or clinical stage T3 or greater. Patients who had undergoing staging investigations (apart from prostate MRI) within 8 weeks prior to randomization were excluded.
Following enrollment, patients were randomly assigned in a 1:1 ratio to either conventional imaging performed using bone scan and CT or PSMA PET/CT. Randomization was stratified according to center. Patients who were randomized to conventional imaging underwent abdomino-pelvic CT scan with contrast as well as technetium-99m bone scan with SPECT CT of chest, abdomen and pelvic in keeping with standard of care. These investigations were assessed in aggregate to determine the presence of findings of interest. For patients randomized to PET/CT, gallium-68 PSMA-11 PET/CT was performed. In patients who had fewer than 3 unequivocal sites of metastasis, cross-over imaging for confirmation was performed within 14 days. Confirmatory testing following imaging was performed at the discretion of the treating physician and included biopsy confirmation.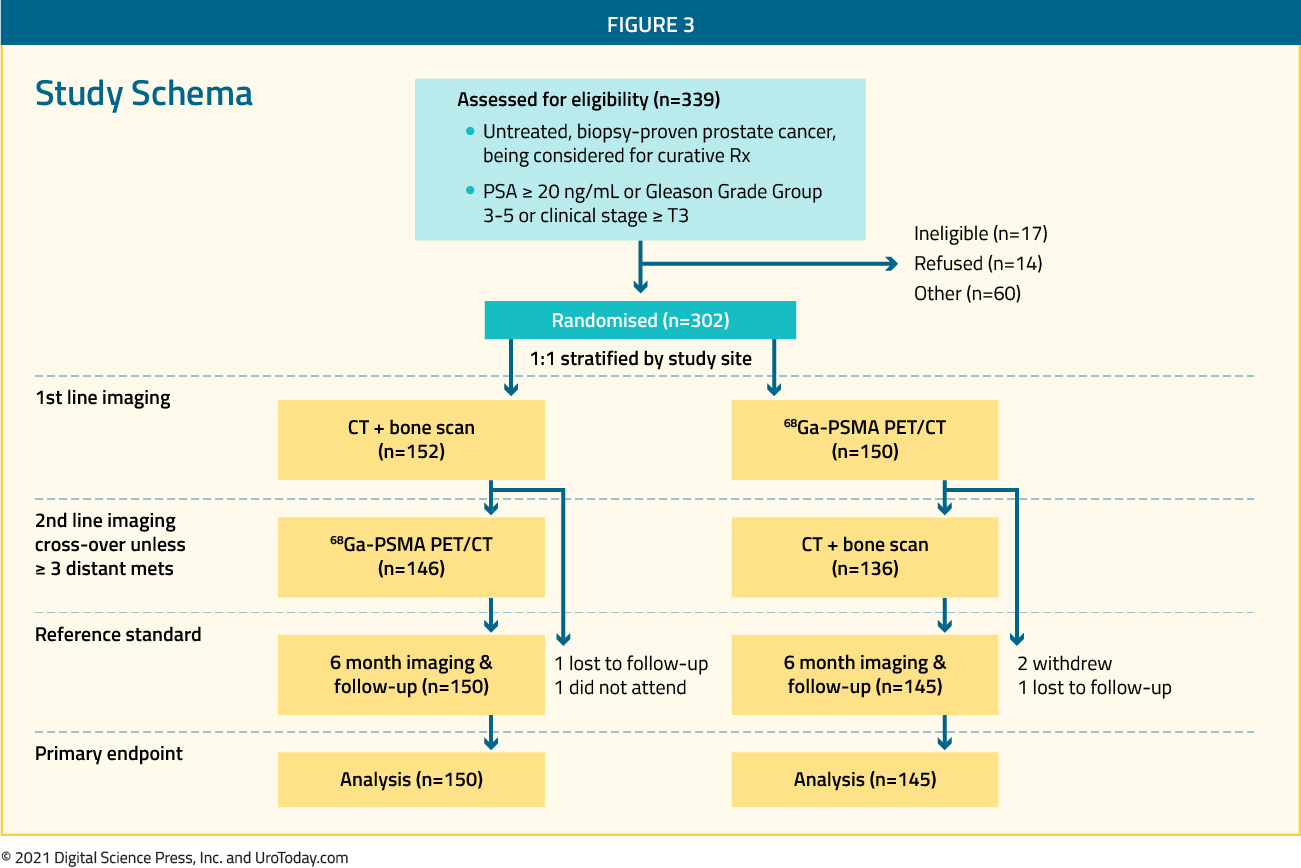
The primary study outcome was accuracy of first-line diagnostic imaging for the identification of either pelvic nodal or distant metastatic disease. Accuracy was assessed using the area under the curve (AUC) of the receiver operating characteristic (ROC) curve. The reference standard was a composite panel of histopathology, imaging, clinical, and biochemical characteristics.
Between 2017 and 2018, the authors randomly assigned 302 patients of whom 300 received assigned first line imaging. In keeping with the prostate cancer population, median age was 68 years, 293 men had ISUP grade 3 or higher, 65 had PSA20 ng/mL or higher, and 82 had clinical stage T3 or T4. 96% (146) of men assigned to conventional imaging underwent subsequent second line PSMA PET-CT. Assessment of the reference standard was possible in 295 (98%) of men, including 87 of whom had evidence of nodal or distant metastasis. Of these, hard criteria were used to define disease in 20 men.
In the primary outcome assessment, PSMA PET-CT had a 27% absolute greater AUC for accuracy compared to conventional imaging (95% confidence interval 23-31): 92% (95% CI 88-95%) vs 65% (60-69%). Conventional imaging had both a lower sensitivity (38% vs 85%) and also a lower specificity (91% vs 98%).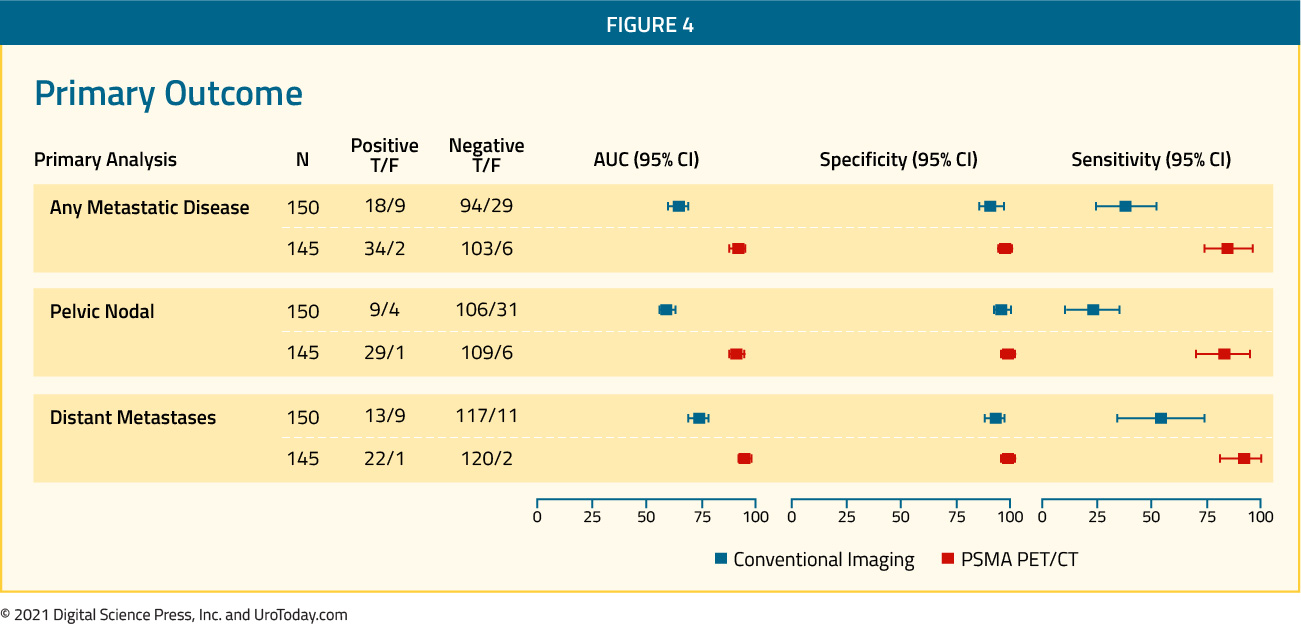
The authors performed a sensitivity analysis in which all lesions rated as equivocal were considered positive. This changed the results only marginally with an absolute difference of 28% (95% confidence interval 23-33%). These results were also consistent in subgroups of patients with pelvic nodal disease and those with distant metastasis. Further post-hoc subgroup analysis showed incremental benefit for PSMA PET-CT in men with GGG4-5 disease, those with GGG less than or equal to 3, and those with a PSA of 20 ng/mL or greater. Further, equivocal findings were more common in men undergoing conventional imaging (23%) compared to those undergoing PSMA PET-CT (7%).
Prior to treatment, the results of conventional imaging studies resulted in treatment change for 23 men (15%, 95% confidence interval 10-22) while the results of PSMA PET-CT resulted in treatment change for 41 (28%, 95% confidence interval 21-36). These changes included both a transition from curative intent to palliative intent treatment in 20 patients (14%) and also a change in treatment approach in 22 (14%). These data demonstrate the clinical utility of utilizing PSMA PET-CT in this clinical space.
Further, conventional imaging was associated with a higher radiation dose (19.2 mSv compared to 8.4 mSv; absolute difference 10.9 mSv, 95% confidence interval 9.8-12.0 mSv0. PSMA PET-CT was not associated with any adverse events and reporter agreement was high for both nodal (kappa 0.87, 95% confidence interval 0.81-0.94) and distant metastatic disease (kappa 0.88, 95% confidence interval 0.94-0.92).
Numerous other studies have assessed the role of 68Ga-PSMA-PET/CT, including in more advanced disease spaces. Two more recently published studies have examined the novel 18F-DCFPyL tracer in the CONDOR11 and OSPREY12 studies. The developmental program for this tracer have spanned the spectrum of prostate cancer from initial staging of patients with high-risk disease who are planned for radical prostatectomy and pelvic lymphadenectomy through to mCRPC.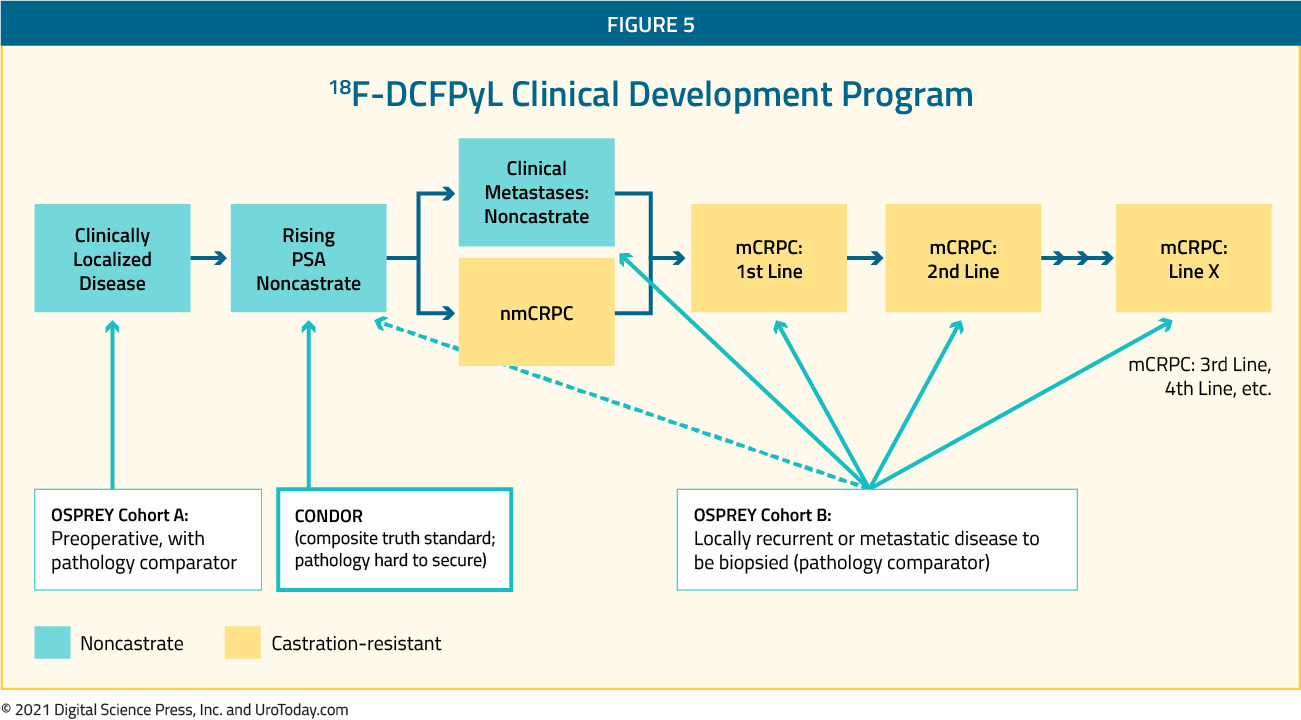
PCWG3 JCO 2016
The CONDOR study focused on patients with biochemically recurrent disease in which the authors recruited men aged 18 years and older with rising PSA after definitive therapy and negative or equivocal standard of care imaging (e.g., CT/MRI, bone scintigraphy, or F-18 fluciclovine)11. The authors undertook by PyL-PET/CT using s single 9 mCi (333 MBq) ± 20% dose of PyL, followed by PET/CT 1-2 hours later. Patients with positive 18F-DCFPyL-PET/CT scans based on local interpretation were scheduled for follow up within 60 days to verify suspected lesion(s) using a composite SOT.As their primary outcome of interest, the authors assessed the correct localization rate (CLR), defined as percentage of pts with a 1:1 correspondence between at least one lesion identified by PyL-PET/CT and the composite standard of truth: pathology, correlative imaging, or PSA response, in descending order of priority. The trial was successful if the lower bound of the 95% confidence interval for CLR exceeded 20% for at least two of three independent, blinded central 18F-DCFPyL-PET/CT reviewers.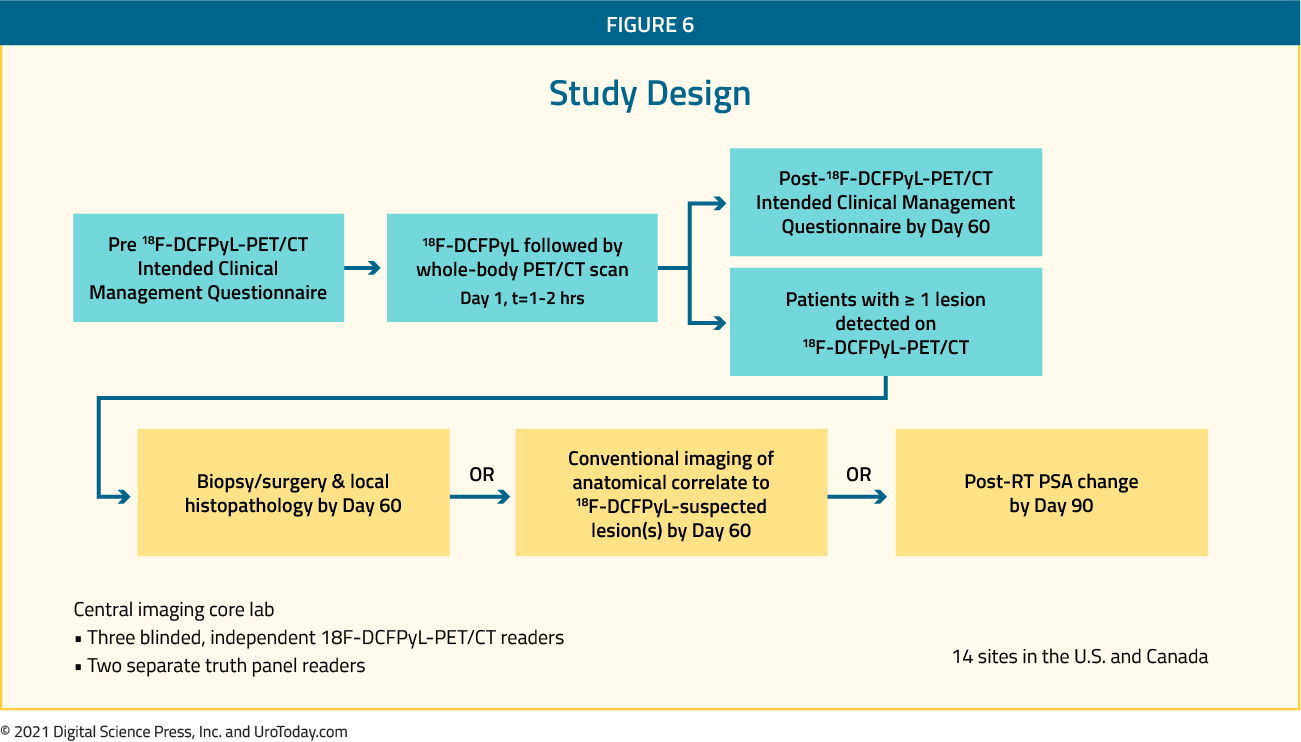
The authors accrued 208 men who met inclusion criteria. Median PSA in this cohort was 0.8 [0.2 - 98.4] ng/mL. Using their defined primary outcome of correct localization rate, the authors demonstrated that PyL-PET/CT correctly localized lesions in 84.8-87.0% of cases among the three readers (lower bound of 95% CI: 77.8%-80.4%), against the composite SOT. 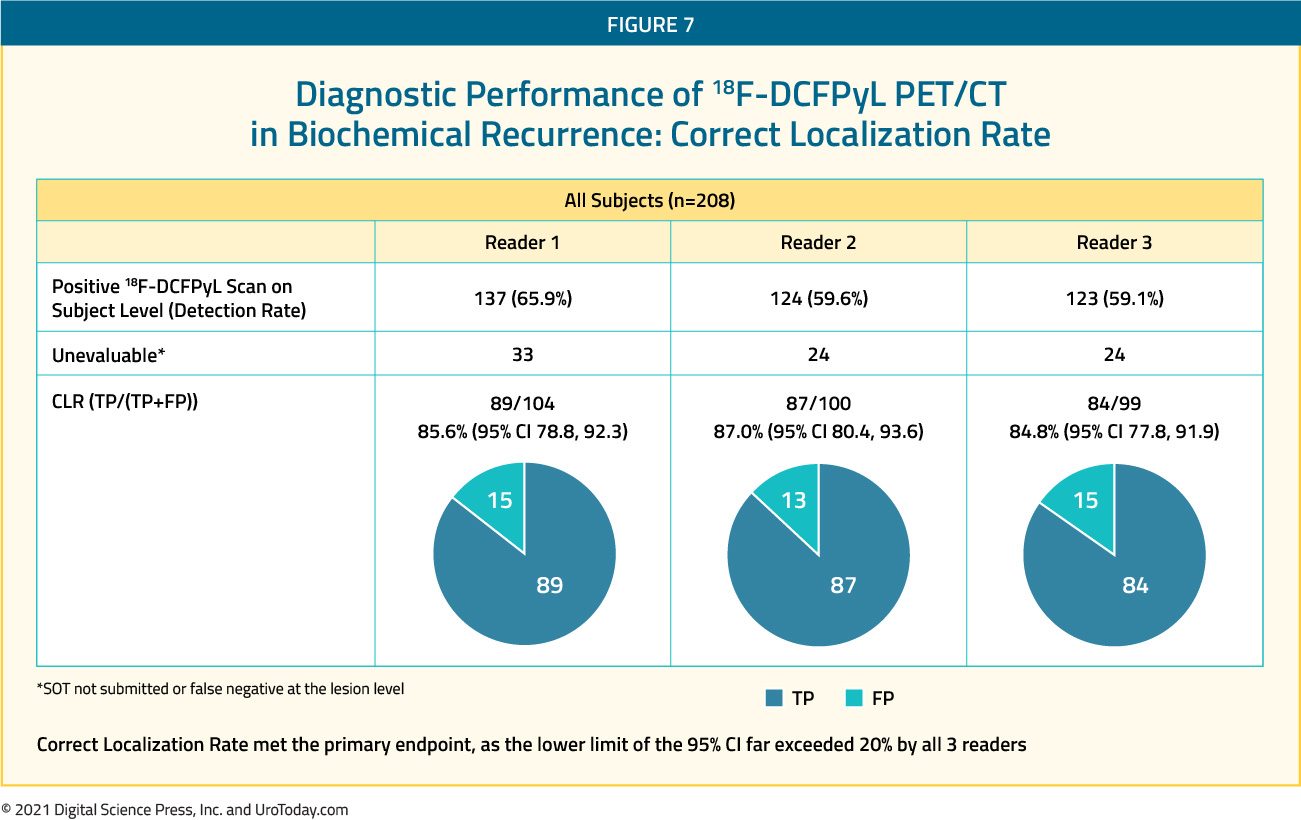
The performance of 18F-DCFPyL-PET/CT by CLR (≥1 lesion co-localized) and PPV (≥1 lesion confirmed) was maintained through all 3 SOT categories:
1. Histopathology (N=31): 78.6-82.8% and 92.9-93.3% for CLR and PPV, respectively
2. Correlative imaging (N=100): 86.1-88.6% and 87.0-89.5% for CLR and PPV, respectively
3. PSA response (N=1): 100% for both CLR and PPV
Additionally, CLR remained high regardless of which correlative imaging modality was used including 18F-fluciclovine-PET/CT (N=71; CLR 86.8-90.9%), MRI (N=23; CLR 80.0-86.7%) and CT (n=6; CLR 80.0-100%).
While these imaging characteristics are important, potentially more important is the demonstrated clinical effect of this information. Using local radiographic assessment, PSMA-avid lesion(s) were found in 142 of 208 patients (69.3%). As a result, more than two thirds of patients enrolled in this study (131 of 205, 63.9%) had a change in intended management following PyL-PET/CT. Of those with a change in management, nearly 80% (103/131, 78.6%) were attributable to positive PyL findings while the remaining 21.4% (28/131) were attributable to negative PyL scans. Changes in management included a transition from salvage local therapy to systemic therapy on the basis of more extensive disease (n=58), a period of observation (n=49), non-curative systemic therapy to attempted curative salvage local therapy (n=43) and observation in place of planned treatment (n=9). In addition to providing this information, PyL was well tolerated with one drug-related SAE (hypersensitivity) and the most common AE being headache (n=4; 1.9%).
Beyond those with biochemically recurrent disease (CONDOR), the 18F-DCFPyL clinical development program includes a variety of other disease spaces which are captured in the OSPREY cohort12. Patients in both cohort A (high-risk prostate cancer undergoing radical prostatectomy and pelvic lymphadenectomy) and cohort B (suspected recurrent/metastatic prostate cancer based on conventional imaging) were included and underwent 18F-DCFPyL PET-CT performed using a single dose of 9 mCi (333 MBq) of 18F-DCFPyL, administered via intravenous injection and followed by PET/CT acquisition 1 to 2 hours thereafter. 18F-DCFPyL-PET/CT detection rates including lesion counts were systematically analyzed according to TNM staging: prostatic (T), pelvic LN (N), extra-pelvic LN (M1a), bone (M1b) and other visceral organs/soft tissue (M1c). Images were reviewed by three blinded central reviewers and the diagnostic performance of 18F-DCFPyL PET-CT was compared to histopathology.
In cohort A, histologic detection of pelvic nodal disease (with specificity and sensitivity as co-primary endpoints) was defined on the basis of surgical lymphadenectomy. In cohort B, histologic detection was based on biopsy of lesions identified on conventional imaging. In total, 385 patients were enrolled of whom 252 were in cohort A and 93 were in cohort B.
In cohort A, 18F-DCFPyL-PET/CT had median specificity of 97.9% (95% CI: 94.5%-99.4%) and median sensitivity of 40.3% (28.1%-52.5%) among the three blinded reviewers. While specificity met the pre-specified threshold for efficacy, sensitivity did not. The median PPV and NPV were 86.7% (69.7%-95.3%) and 83.2% (78.2%-88.1%), respectively. In cohort B, the median sensitivity and PPV for extra-prostatic lesions were 95.8% (87.8%-99.0%) and 81.9% (73.7%-90.2%), respectively.
PSMA as a target for therapeutic intervention
Radiopharmaceuticals are pharmaceutical agents which contain radioisotopes that emit radiation and may be used for diagnostic or treatment purposes. From a therapeutic perspective, as they are typically given via intravenous infusion, radiopharmaceuticals are systemic radiotherapies, emitting alpha or beta radiation. Radiopharmaceuticals are indicated in patients with castrate resistant prostate cancer with symptomatic bone metastases. Historically, beta-particle emitting agents including strontium-89 (Metastron), samarium-153 (Quadramet), phosphorus-32, and rhenium-186 were used as palliative therapies for patients with symptomatic bone disease13. In this context, they are quite effective in relieving bony pain14. However, these agents did not significantly improve survival15. In contrast, the ALSYMPCA trial, demonstrated an improvement in both overall survival and skeletal-related events for patients receiving the alpha-emitter radium-22316. Radium-223 functions as a calcium mimetic and selectively binds newly forming bone stroma in regions of high bone turnover in osteoblastic or sclerotic bone metastasis17. It then emits high-energy alpha particles with a very short range (less than 100 μm)18. This high-energy radiation induces a highly localized cytotoxic effect due to double-stranded DNA breakage.
In contrast to the localization of radium-223 to areas of high bone turnover due to its calcium mimetic properties, PSMA-based theranostics are targeted to regions of tumor cells on the basis of the PSMA transmembrane protein. PSMA-based theranostics have, to date, utilized labelling to the beta-particle emitter Lutetium-117 (Lu-177). Lu-177 has favourable characteristics for theranostics as emitted beta-particles have limited tissue penetration (less than 2mm) which minimize injury to adjacent healthy tissue. Further, Lu-177 emits low-energy gamma rays which can be used to image the tumor in real time during treatment, with a relatively long half-life of 6.7 days resulting in a relatively prolonged treatment period following administration. While a number of 177Lu-labelled PSMA-targeted ligands have been developed, two are most commonly used: 177Lu-PSMA-617 and 177Lu-PSMA-I&T.
A recent systematic review and meta-analysis in press at European Urology as of April 8, 202119 has highlighted data for the use of Lu-177 in patients with metastatic castration-resistant prostate cancer (mCRPC). The authors included a total of 24 studies with 1192 patients who had received Lu-177 based therapy. The majority of these studies reported on 177Lu-PSMA-617 (20 studies) while 3 reported on 177Lu-PSMA-I&T, and 1 reported on both. In this heavily pre-treated population, 44% of patients (95% confidence interval 39-50%) had a PSA response of at least 50% among those receiving 177Lu-PSMA-617 with similar, though slightly lower numbers among those receiving 177Lu-PSMA-I&T (36%, 95% confidence interval 26-47%). Further, these authors found that treatment was well tolerated with very low rates of grade 3 or 4 toxicity, with the highest observed rates for anemia at 8% (95% confidence interval 5-12%). Using meta-regression, the authors demonstrated that patients who had more than one cycle of therapy were more likely to experience PSA declines of 50% or greater.
While the aforementioned systematic review highlighted 24 studies that have been performed examining the role of Lu-177 based theranostics, attention has focused on two key trials. The first of these, which is now published in the Lancet20, is the TheraP trial. This ANZUP/PCFA sponsored trial began in 2016 and represents a world-first study, being a phase III randomized controlled trial of a direct targeted radioligand. TheraP enrolled patients with mCRPC who had previously received docetaxel and were eligible to receive cabazitaxel. Patients were required to have progressive disease with a rising PSA with absolute PSA of 20 ng/mL or higher. All patients underwent both Ga-68-PSMA-PET/CT and F-18-FDG-PET/CT prior to randomization. To be eligible for inclusion, patients must have had a high avidity lesion on PSMA PET/CT (SUV max >20 at any site) with measurable disease with SUV max of 10 or greater. Further, there could be no sites of disease which were FDG positive but PSMA negative.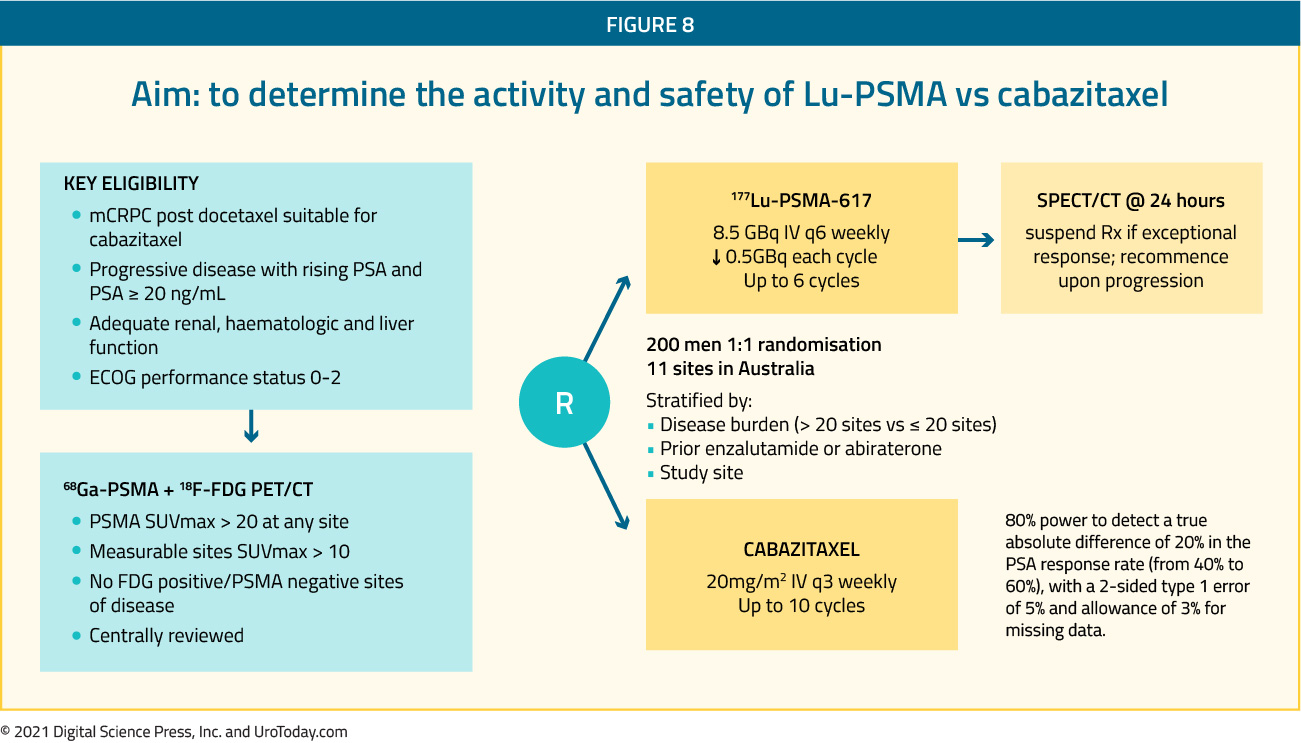
Among 200 men at 11 sites in Australia who were eligible, randomization was performed in a 1:1 fashion to 177Lu-PSMA-617 or cabazitaxel. Randomization was stratified according to disease burden, prior use of enzalutamide or abiraterone, and study site.
The primary study outcome was PSA response and these data were initially reported at ASCO 2020. PSA response was operationalized looking at a response of at least 50% from baseline. Compared to those receiving cabazitaxel (37%, 95% confidence interval 27 to 46%), responses were significant higher among those who received Lu-PSMA (66%, 95% confidence interval 56 to 75%) with an absolute difference of 29% (95% confidence interval 16 to 42%, p<0.0001).
More recent data were presented at ASCO-GU 2021 examining secondary endpoints including PSA/radiologic PFS (PCWG3), pain response (≥2 point reduction on McGill-Melzack Present Pain Intensity scale, objective response rate (RECIST 1.1), adverse events (CTCAE), PROs (EORTC QLQ-C30) and overall survival. As of a data cut-off of July 20, 2020, median follow-up was 18.4 months. PFS was significantly longer in those assigned Lu-PSMA rather than cabazitaxel (rates at 1 year 19% [95%CI 12-27%] vs 3% [1-9%], HR 0.63, 95%CI 0.46-0.86; p = 0.003) based on 173 events. As similar benefit was seen whether PFS was examined radiographically (rPFS, HR 0.64, 95%CI 0.46-0.88; p = 0.007; 160 events) or based on PSA (PSA-PFS, HR 0.60 95%CI 0.44-0.83; p = 0.002; 172 events). Among men with measurable disease (n=78), objective response rates were significantly greater in the Lu-PSMA arm (49% vs 24%, RR 2.1, 95%CI 1.1-4.1; p = 0.019). Similarly, among those with pain at baseline (n=90), pain responses occurred in 60% in the Lu-PSMA arm vs 43% for cabazitaxel (RR 1.42, 95%CI 0.84-4.48; p = 0.10). Overall, patient-reported global health status was similar between arms (Lu-PSMA 64 [95%CI 61-67] vs cabazitaxel 60 [57-64]), though significantly better function was noted for patients receiving Lu-PSMA with respect to fatigue, social functioning, insomnia, and diarrhoea domains. No PRO domains were superior for cabazitaxel. The authors further assessed deterioration free survival, defined as the time to a 10 point or greater decline in EORTC QLQ-C30 global health related quality of life. Again, this favoured the Lu-PSMA treated group.
On March 23, 2021, Novartis reported that the phase III VISION trial assessing 177Lu-PSMA-617 compared to standard of care met both primary endpoints, significantly improving overall survival and rPFS among men with PSMA-positive mCRPC. Important inclusion criteria for this trial included failure of a previous taxane and a novel androgen axis therapy. Patients in the VISION trial were randomized 2:1 to receive 177Lu-PSMA-617 plus best supportive/standard of care versus best supportive/standard of care alone. 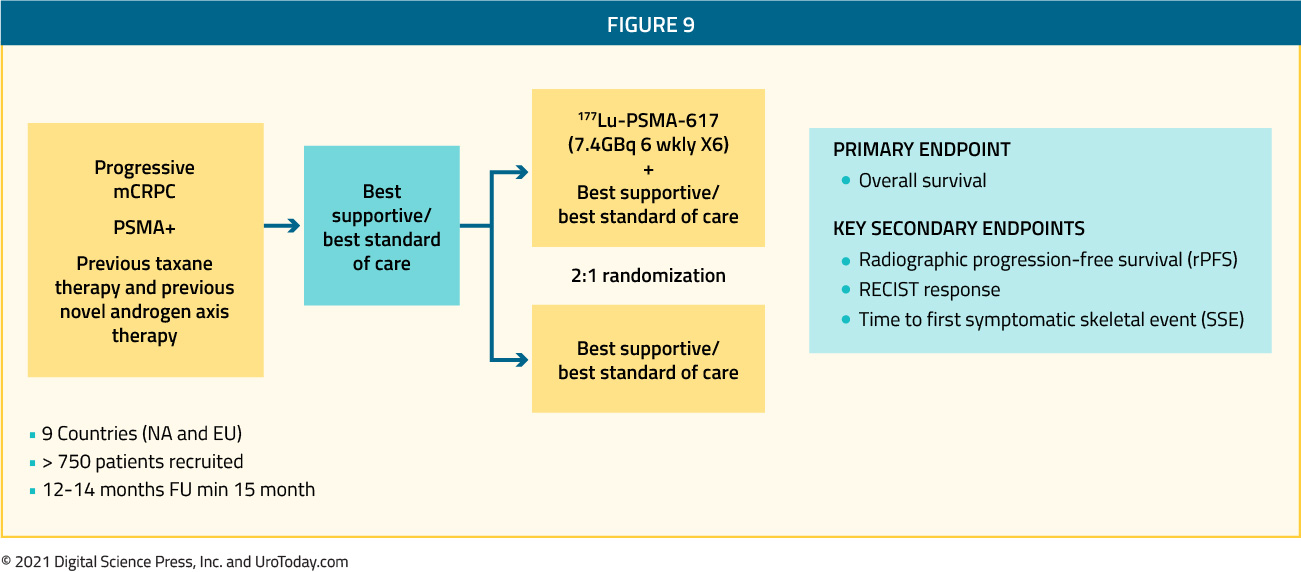
The results of the important VISION trial are expected to be presented in 2021 and have the potential to change practice patterns of advanced prostate cancer.
While both TheraP and VISION are assessing the role of 177-Lu-PSMA in mCRPC, there are notable differences. First, VISION is an industry sponsored trial with a much larger sample size (800 patients). Second, in VISION, a central production model is used with the agent subsequently shipped ready for clinical use. In contrast, in TheraP, lutetium is made on site. This allows some flexibility, but required standardization and quality control in order to undertake the study. Moving forward, this on-site approach is expected to be much lower cost than centralized processing. Third, as mentioned above, in order to be included in TheraP, patients could not have sites of disease which were FDG positive but PSMA negative. This requirement led to the exclusion of approximately 30% of otherwise eligible men. In contrast, the VISION trial didn’t have this requirement. This narrowing of the selection criteria in TheraP will likely enrich for patients who are likely to respond, compared to VISION.
Moving forward, the optimal role for 177Lu-PSMA therapy remains to be completely delineated. Additional trials are ongoing, including (i) the PRINCE trial assessing 177Lu-PSMA-617 plus pembrolizumab in men with mCRPC that have progressed after enzalutamide, abiraterone or apalutamide; (ii) the LuPARP trial assessing 177Lu-PSMA-617 + olaparib in mCRPC men progressing on 2nd generation AR-targeted therapy and taxane chemotherapy; (iii) the UpFrontPSMA trial assessing 177Lu-PSMA-617 + ADT followed by docetaxel versus ADT + docetaxel in men with de novo high-volume metastatic hormone naïve prostate cancer; and (iv) the LuTectomy trial assessing 177Lu-PSMA-617 prior to radical prostatectomy for men with high-risk localized prostate cancer. Certainty, the TheraP trial has demonstrated its value in patients who have progressed following prior docetaxel therapy for mCRPC. The results of the VISION trial will also provide further clarity as to the treatment options for men with mCRPC that have failed prior therapies. The aforementioned ongoing studies assessing 177Lu-PSMA-617 earlier in the disease process and in combination with other approved treatments for advanced prostate cancer will continue to delineate the role of 177Lu-PSMA-617 in the spectrum of prostate cancer therapeutics.
Written by: Zachary Klaassen, MD MSc, Medical College of Georgia, Augusta, Georgia, USA
Published Date: April 2021