Introduction
Metastatic urothelial carcinoma is associated with a poor prognosis, with an estimated 17,000 deaths annually in the United States from this disease.1 Platinum-based chemotherapy had long been considered the standard of care first line treatment for platinum-eligible patients with metastatic urothelial carcinoma.However, prognoses with such regimens are poor, with limited median overall survivals of approximately 15 to 16 months.2,3 Progress in this disease space had been limited over the prior two decades, with multiple attempts at combining chemotherapy with PD-1/PD-L1 inhibitors failing to improve overall survival (OS) in patients with locally advanced/metastatic urothelial carcinoma.4,5
At ESMO 2023, the results of two practice-changing trials were presented: EV-302/KEYNOTE-A39 (enfortumab vedotin + pembrolizumab) and CheckMate 901 (nivolumab + gemcitabine/cisplatin).6,7 The combination of enfortumab vedotin + pembrolizumab has ‘moved the goalpost’ in this disease space, doubling the median overall survival of such patients to approximately 32 months, irrespective of cisplatin eligibility. Additionally, CheckMate 901 is the 1st trial to demonstrate an OS benefit for combination immune checkpoint inhibitors plus chemotherapy. The results of these trials have culminated in the US Food and Drug Administration (FDA) approving enfortumab vedotin + pembrolizumab in December 2023 for patients in this setting,8 with nivolumab + gemcitabine/cisplatin currently undergoing priority review by the FDA, with a target action date of April 2024.9
In this Center of Excellence article, we review the EV-302/KEYNOTE-A39 trial and discuss its impact on the metastatic urothelial carcinoma treatment landscape, review the landmark trials of cisplatin-based chemotherapy in the 1st line treatment setting, including CheckMate 901, as well as review recent data for avelumab maintenance therapy among patients that did not progress on first-line chemotherapy.
Enfortumab Vedotin + Pembrolizumab
Enfortumab vedotin is an antibody-drug conjugate targeting Nectin-4, which is a tumor-associated antigen found on the surface of most urothelial carcinoma cells. Its cell surface expression decreases as urothelial carcinoma progresses through more advanced stages,10 providing a strong rationale for the use of enfortumab vedotin in the front-line setting. Additionally, both enfortumab vedotin and pembrolizumab have individually demonstrated a survival benefit in previously treated locally advanced/metastatic urothelial carcinoma.11,12The objective of EV-302/KEYNOTE-A39 (NCT04223856) was to compare the combination of enfortumab vedotin + pembrolizumab to platinum-based chemotherapy in previously untreated locally advanced/metastatic urothelial carcinoma patients, regardless of cisplatin eligibility and PD-L1 expression status.
Patients in this trial were randomized 1:1 to either enfortumab vedotin + pembrolizumab (n=442) or gemcitabine + cisplatin/carboplatin (n=444) for a maximum of 6 cycles. Notably, there were no maximum treatment cycles for enfortumab vedotin (i.e., continued until clinical/disease progression or unacceptable toxicity), whereas pembrolizumab was administered for a maximum of 35 cycles. The dual primary endpoints were progression-free survival, assessed via blinded independent central review (BICR), and OS. The study design is as follows:
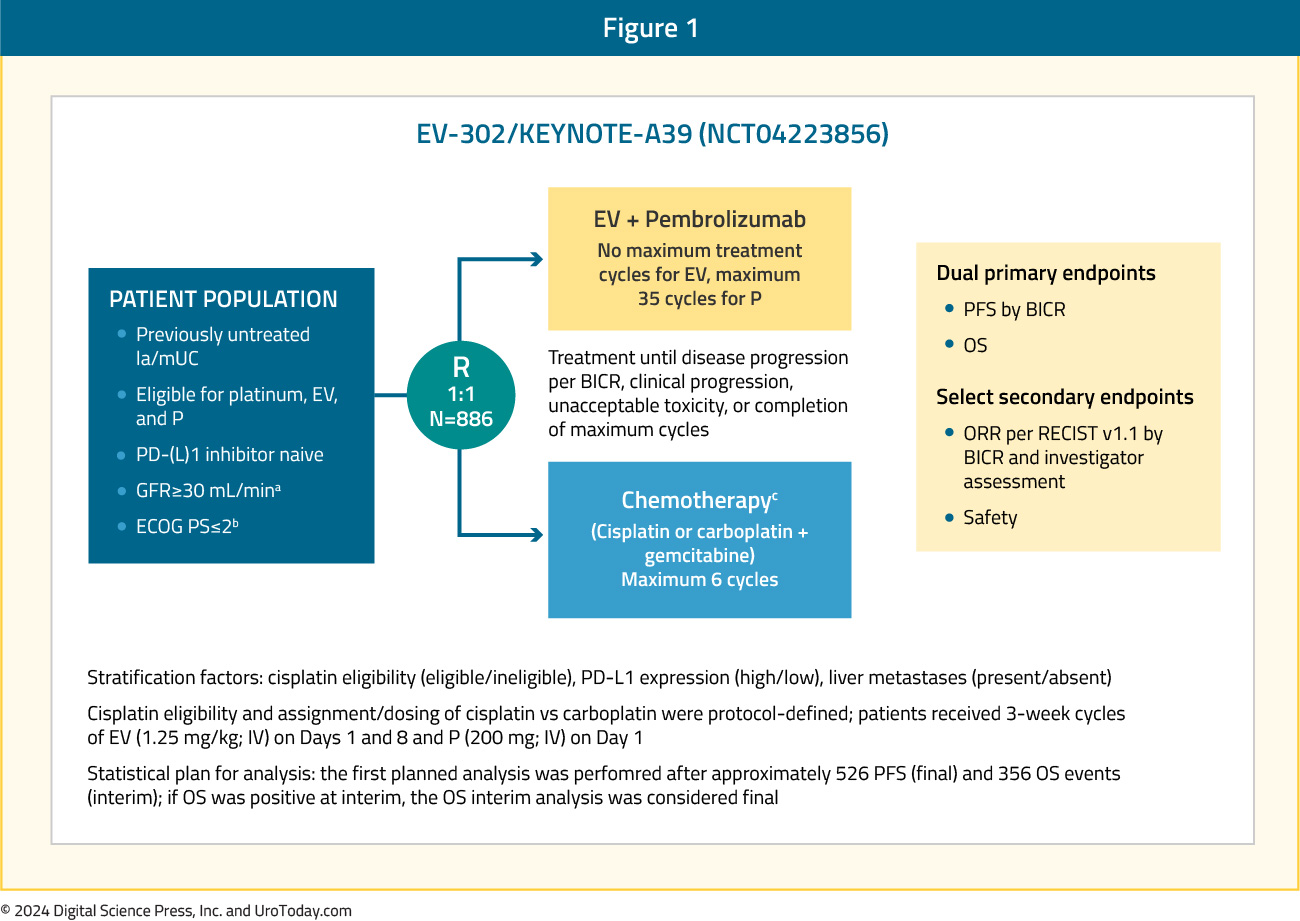
The median patient age was 69 years, and 98% had an excellent performance status (ECOG: 0 – 1). Notably, ~25% of patients had upper tract disease. Overall, 46% of patients were cisplatin-ineligible, and 58% had tumors with a high PD-L1 expression. Liver metastases, a known adverse prognostic factor, were present in 22% of patients.
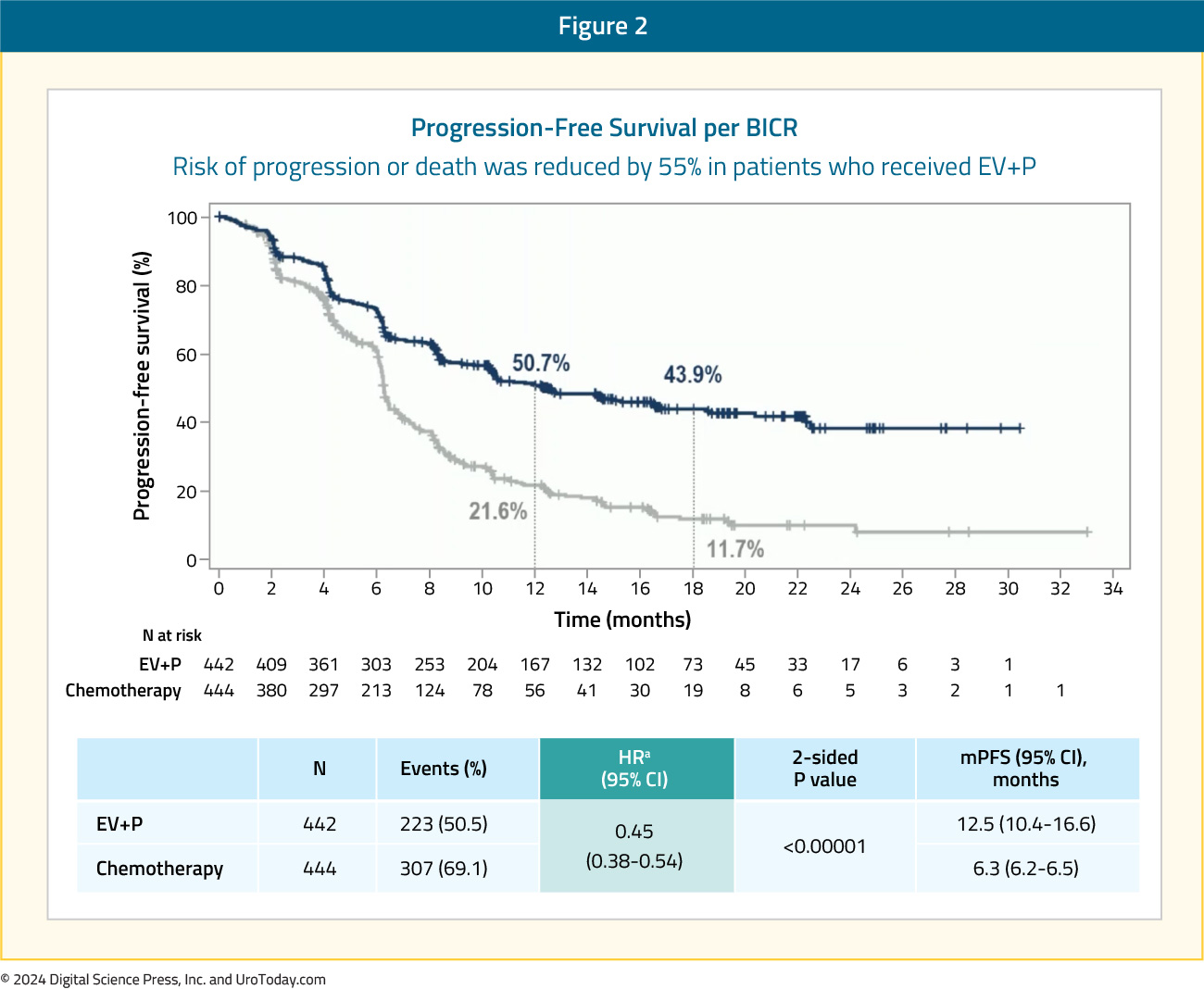
Compared to platinum-based chemotherapy, enfortumab vedotin + pembrolizumab prolonged progression-free survival from a median of 6.3 months to 12.5 months (HR: 0.45, 95% CI: 0.38 – 0.45, p<0.001):
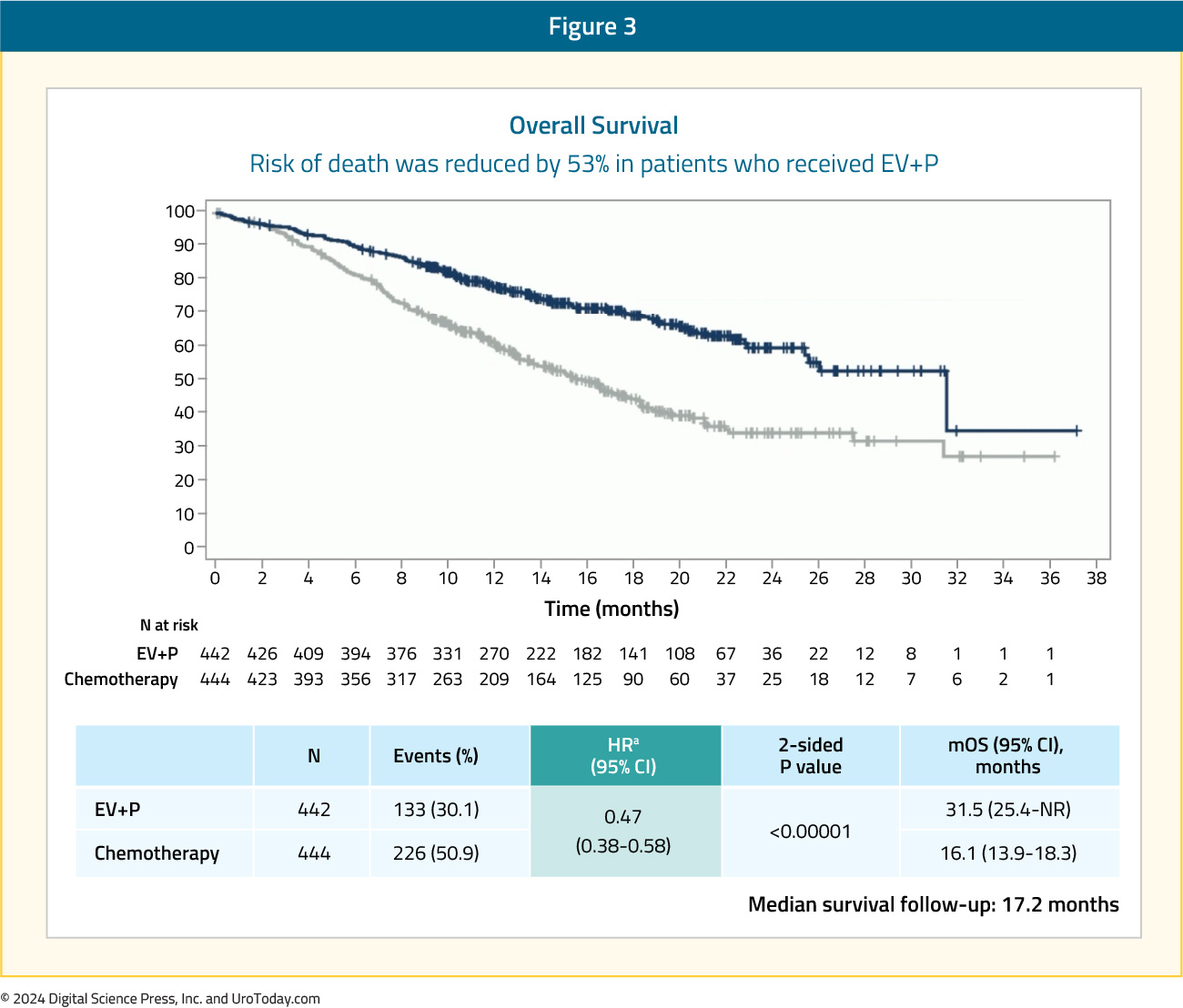
OS was nearly doubled in the enfortumab vedotin + pembrolizumab arm, with median survivals of 31.5 and 16.1 months, respectively (HR: 0.47, 95% CI: 0.38 – 0.58, p<0.00001). These survival benefits were observed despite a higher proportion of patients in the chemotherapy arm receiving subsequent systemic therapy (66.2% versus 28.9%):
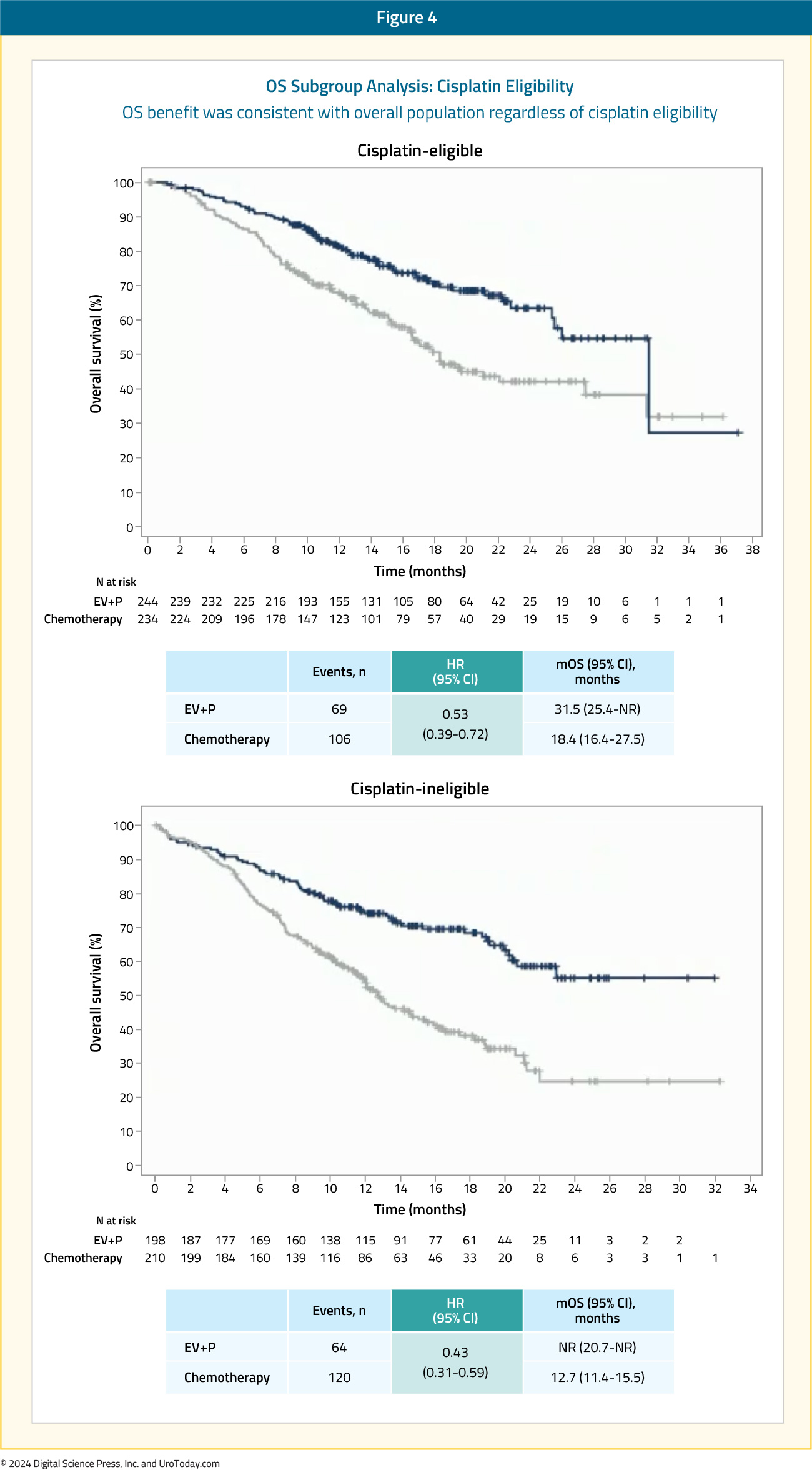
Significantly, clinically meaningful benefits for enfortumab vedotin + pembrolizumab were observed irrespective of cisplatin eligibility or tumoral PD-L1 expression:
A complete response was observed in 29% of patients in the enfortumab vedotin + pembrolizumab arm, compared to 12.5% for platinum-based chemotherapy. The objective response rates were 68% and 44%, respectively:

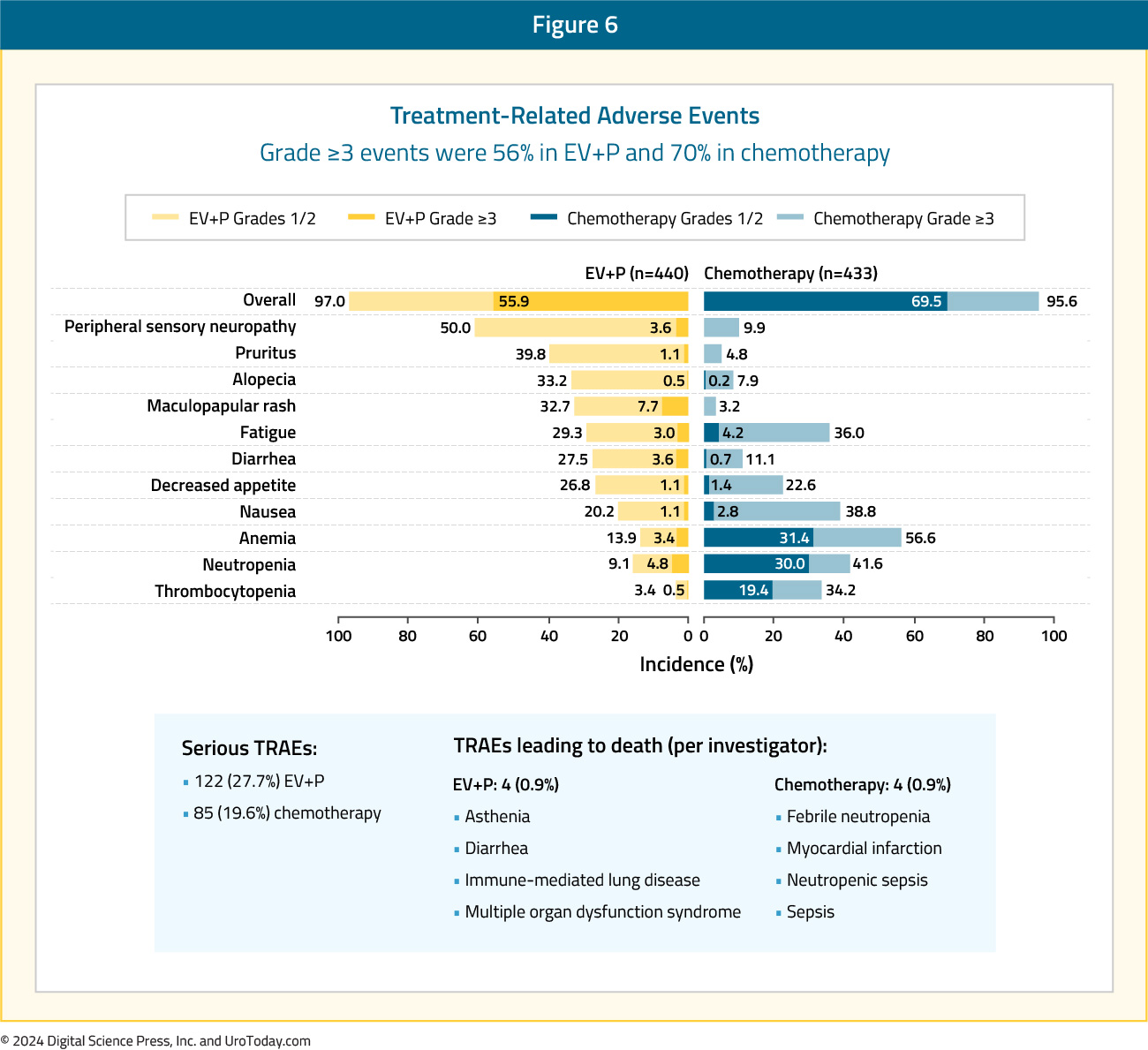
Treatment-related adverse events (TRAEs) were consistent with the known safety profiles of each of the drugs. Serious TRAEs occurred in 27.7% of patients in the enfortumab vedotin + pembrolizumab arm, compared to 19.6% with chemotherapy. TRAE leading to death occurred in 4 patients (0.9%) in each arm. Overall, grade 3+ adverse events occurred in 56% and 70% of patients in the enfortumab vedotin + pembrolizumab and chemotherapy arms, respectively. The most common enfortumab vedotin TRAEs were skin reactions, peripheral neuropathy, ocular disorders, and hyperglycemia:
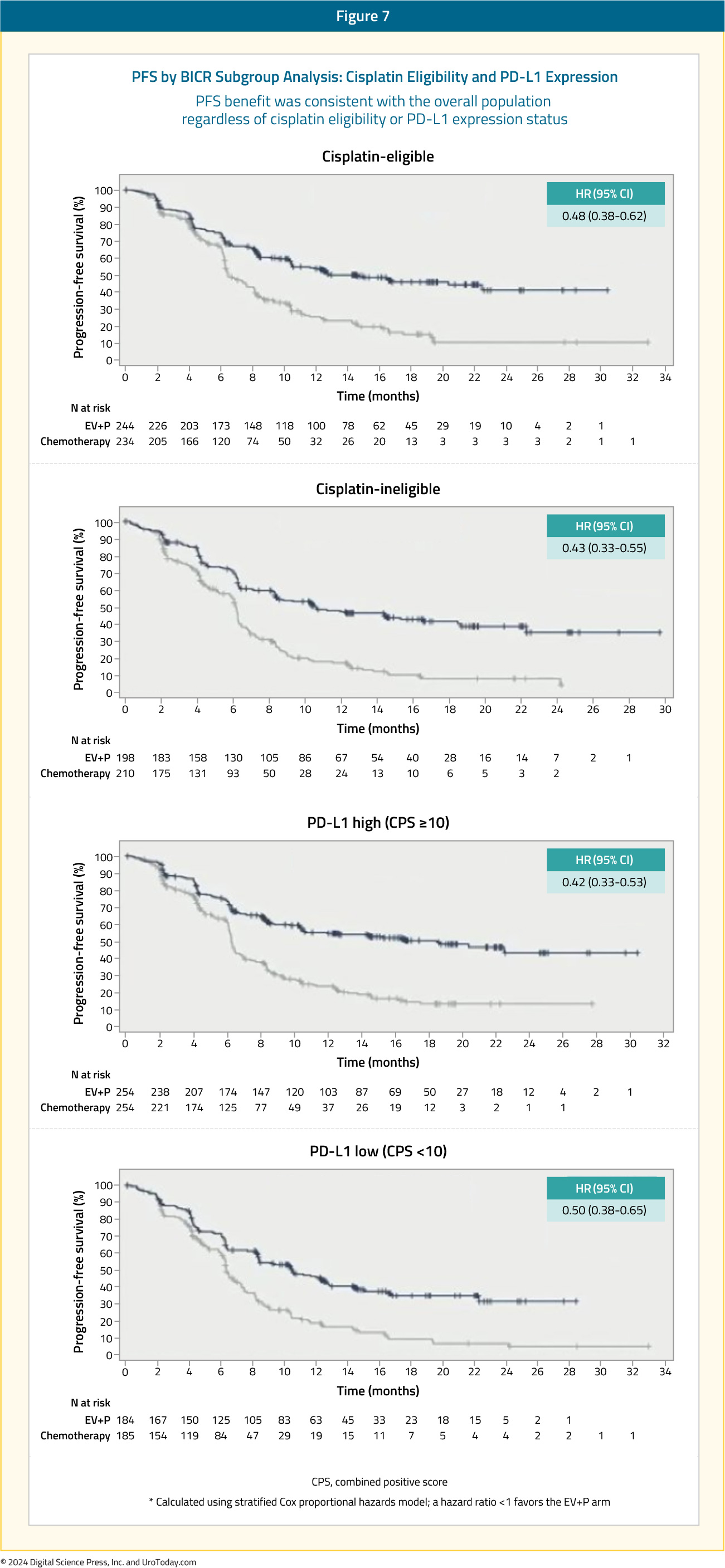
At ASCO GU 2024, prespecified subgroup analysis results were presented by Dr. Michiel van der Heijden. For these analyses, consistent PFS results were observed in favor of enfortumab vedotin + pembrolizumab, irrespective of cisplatin eligibility (eligible versus ineligible) and PD-L1 status (high versus low), with HRs consistently in the 0.42 – 0.50 range:
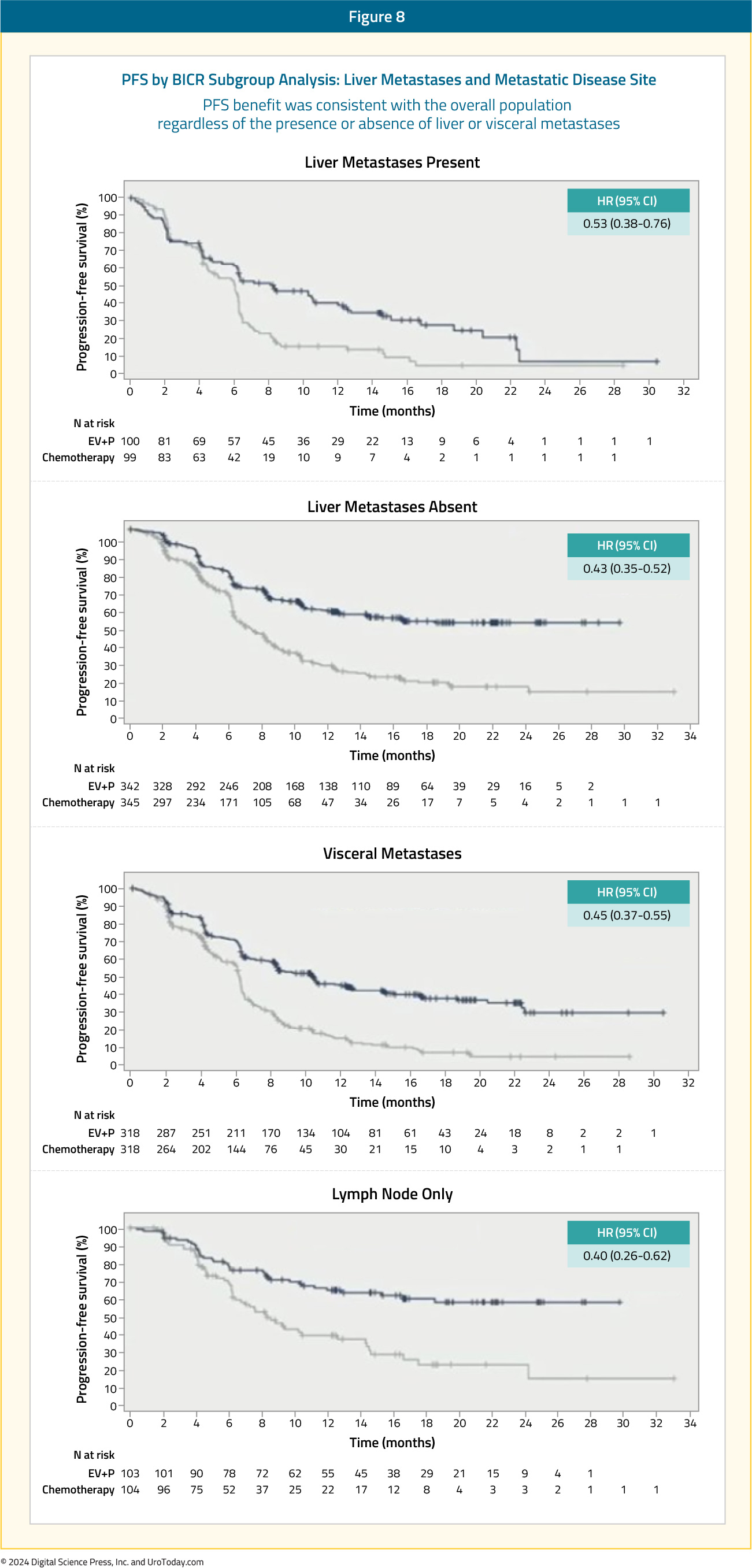
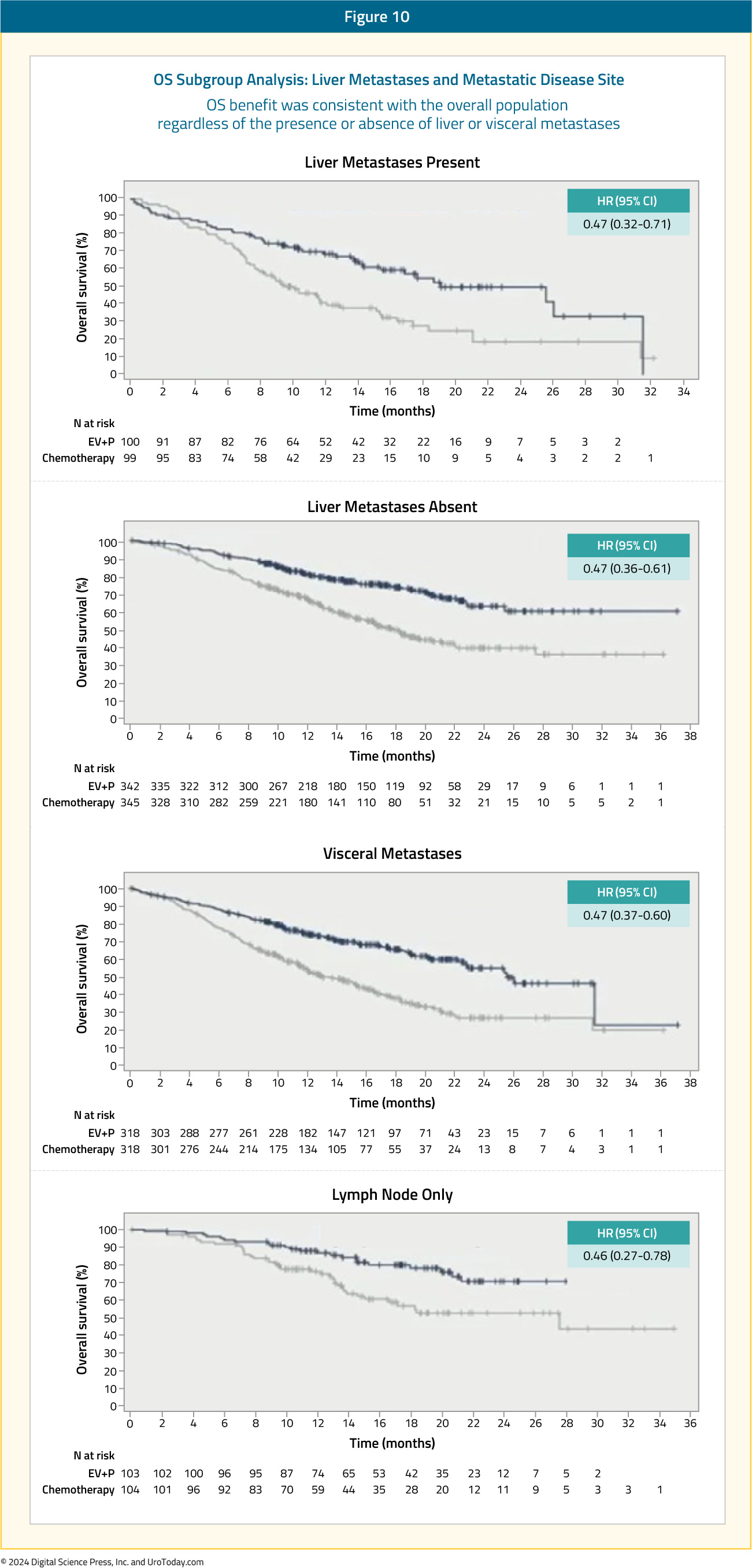
When stratified by site/extent of metastatic disease spread, enfortumab vedotin + pembrolizumab consistently outperformed chemotherapy irrespective of presence/absence of liver metastases and presence of visceral versus lymph node only metastases:
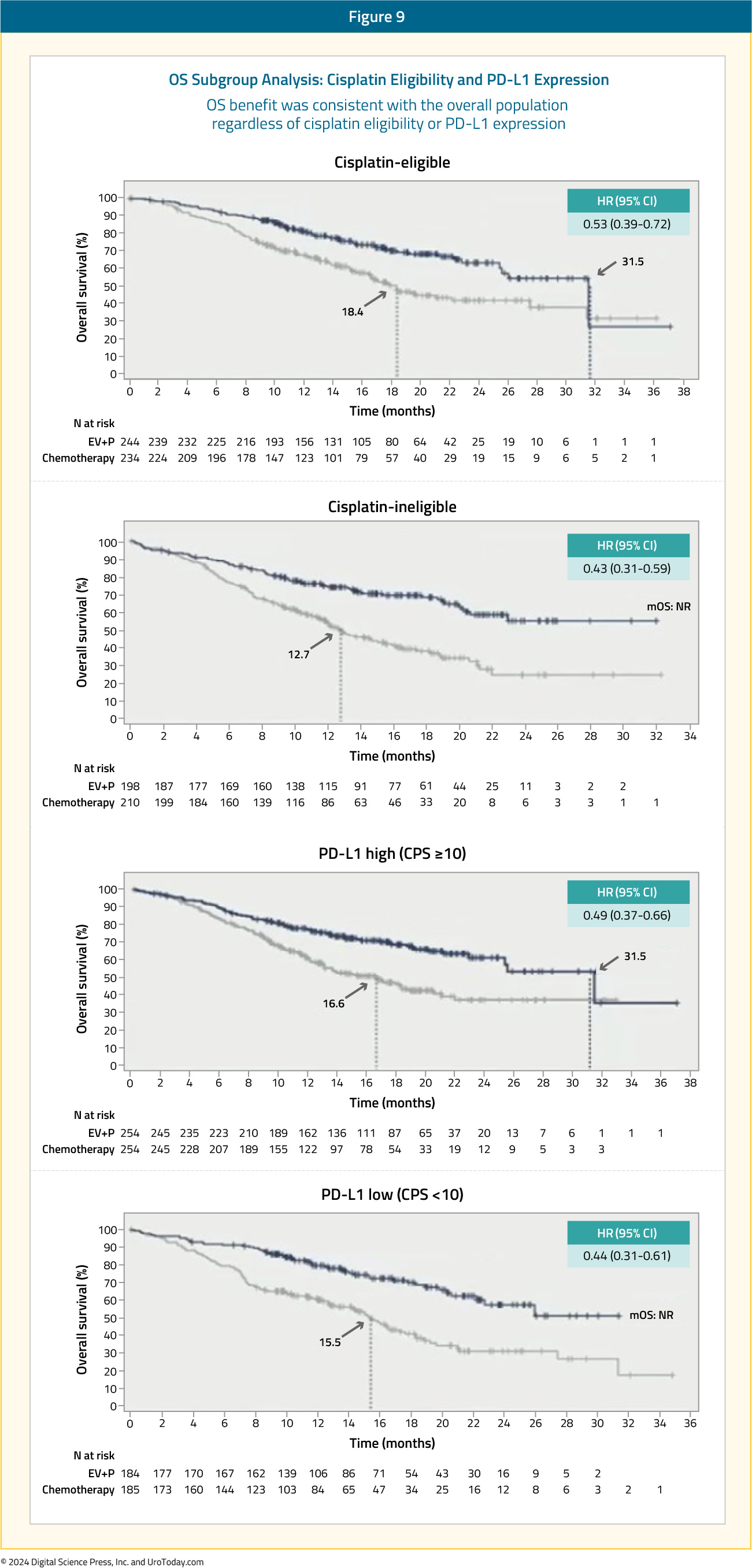
Similar results were consistently observed for the overall survival subgroup analyses in favor of enfortumab vedotin + pembrolizumab, with clinically meaningful HR and median survival improvements across all subgroup comparisons:
Cisplatin-Based Chemotherapy
Determining Cisplatin EligibilityThe Galsky criteria, published in the Journal of Clinical Oncology in 2011, are commonly used to determine eligibility for cisplatin-based chemotherapy.13 Based on a review of phase II and phase III trials, Galsky and colleagues determined that unfit patients for cisplatin-based chemotherapy were those who met ≥1 of the following criteria:
- Eastern Cooperative Oncology Group performance status of 2
- Creatinine clearance <60 mL/min
- Grade ≥ 2 hearing loss
- Grade ≥ 2 neuropathy
- New York Heart Association Class III heart failure
MVAC
The MVAC regimen was first reported in 1985 at Memorial Sloan Kettering Cancer Center to show sensitivity to urothelial carcinoma.14 Patients with measurable disease had a 72% response rate and 36% of patients achieved a complete response, with an OS of 13.1 months.15 In an update of this cohort published in 1999, the median overall survival was 14.8 months, with a 5-year survival rate of 17%.16
MVAC versus Gemcitabine + Cisplatin
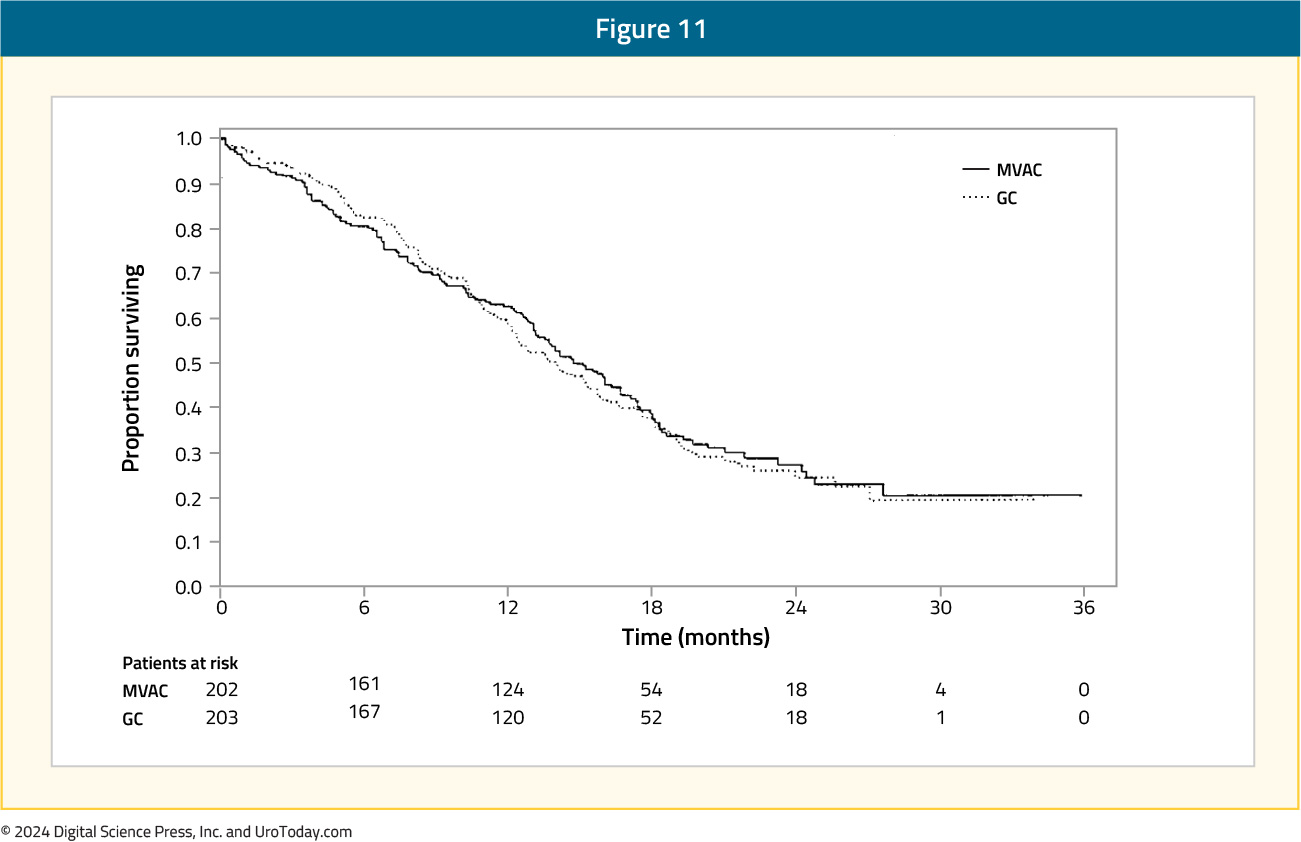
In 2000, van der Maase et al.2 published a sentinel phase 3 randomized, multinational, multicenter trial that compared gemcitabine + cisplatin versus MVAC. This trial included 405 patients with stage IV urothelial carcinoma and no prior systemic therapy who were randomized to gemcitabine 1,000 mg/m2 days 1, 8, and 15 + cisplatin 70 mg/m2 (n = 203) or standard MVAC every 28 days (n = 202) for a maximum of six cycles. Overall survival was similar in both arms (HR: 1.04, 95% CI: 0.82 – 1.32):
Additionally, there was no difference in time to progressive disease (HR: 1.05, 95% CI: 0.85 – 1.30), time to treatment failure (HR 0.89, 95% CI 0.72 – 1.10), and response rate (gemcitabine + cisplatin: 49% vs MVAC: 46%). Grade 3-4 anemia (27% versus 18%) and thrombocytopenia (57% versus 21%) occurred more commonly in gemcitabine + cisplatin-treated patients compared to MVAC; however, MVAC patients had higher rates of grade 3-4 neutropenia (82% versus 71%), neutropenic fever (14% versus 2%), and neutropenic sepsis (12% versus 1%). As such, this trial was able to conclude that gemcitabine + cisplatin provides a similar survival advantage to MVAC, with a better risk-benefit ratio.
Dose Dense versus Standard MVAC
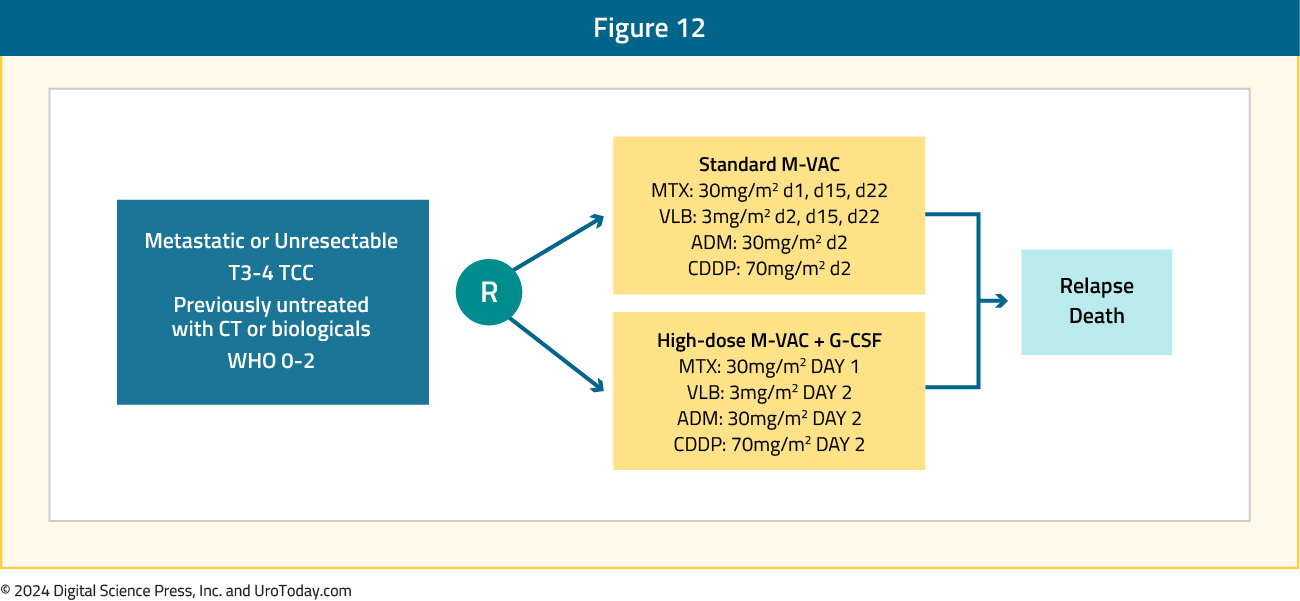
In an attempt to improve upon the results obtained with MVAC, Dr. Sternberg and colleagues initiated the EORTC 30924 trial assessing dose dense MVAC + recombinant human granulocyte colony-stimulating (GCF) versus classic MVAC as first line treatment for metastatic urothelial carcinoma.3 The trial design for EORTC 30924 is as follows:
Overall, there were 263 patients randomized to 2 weeks of dose dense MVAC versus 4 weeks of MVAC, and with a median follow-up of 38 months, the complete response rate in the dose dense MVAC arm was 21% and partial response rate was 41%, for an overall response rate of 62%. This was superior to the MVAC arm which had a complete response rate of 9% (p = 0.009) and partial response rate was 41%, for an overall response rate of 50% (p = 0.06). Although there was an improvement in progression-free survival among patients receiving dose dense MVAC (HR 0.75, 95% CI 0.58 – 0.98), there was no difference in overall survival (p = 0.122) or time to progression (p = 0.114).
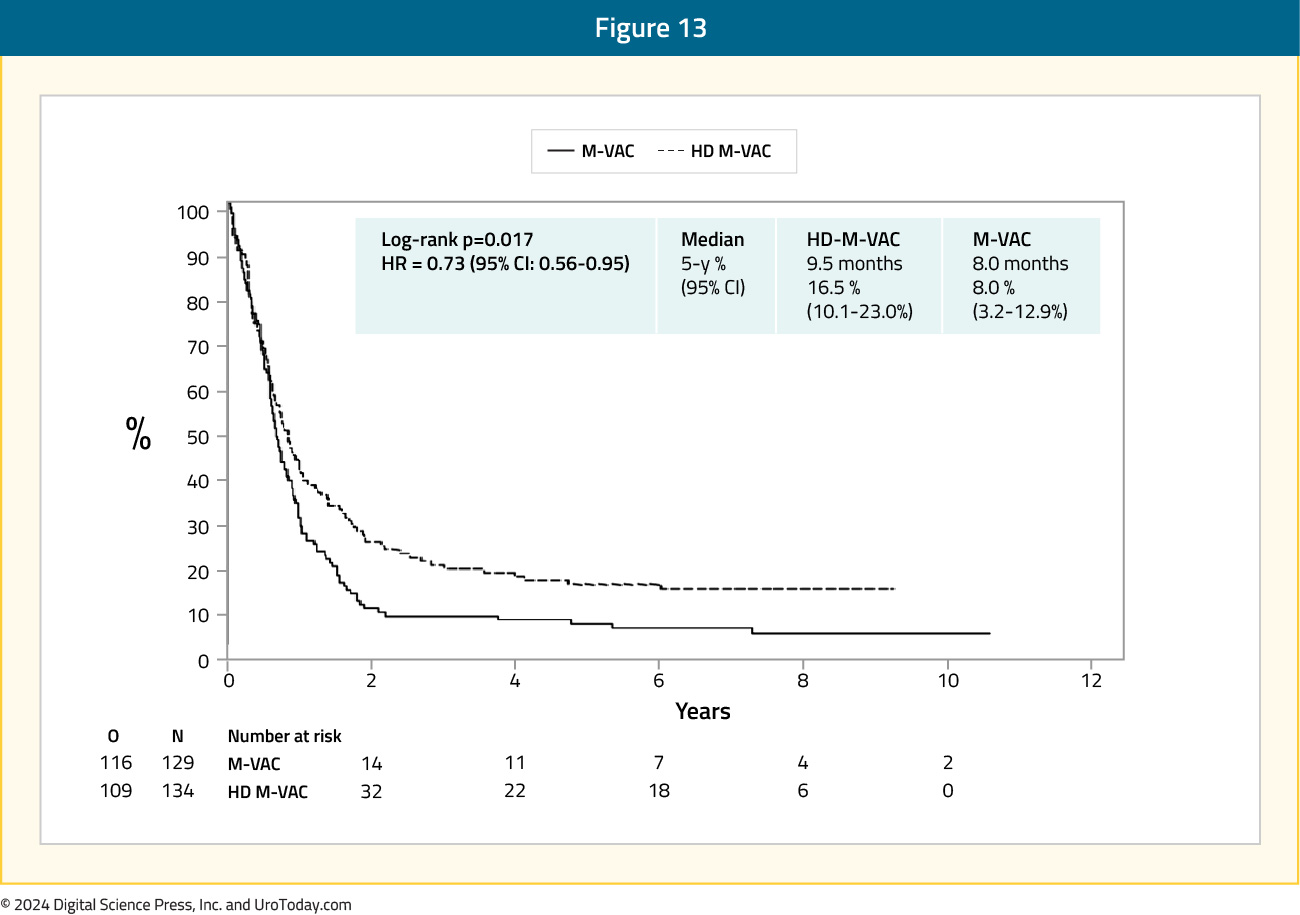
Extended follow-up (median 7.3 years) of the EORTC 30924 trial was published in 2006.17 At the time of this analysis, 24.6% of patients were alive in the dose dense MVAC arm versus 13.2% in the MVAC arm. The median progression-free survival was still improved in the dose dense MVAC arm (9.5 months) compared to the MVAC (8.1 months) arm (HR: 0.73, 95% CI: 0.56 – 0.95):
Additionally, the median overall survival was 15.1 months in the dose dense MVAC arm compared to 14.9 months in the MVAC arm (HR: 0.76, 95% CI: 0.58 – 0.99), with a 5-year survival rate of 21.8% and 13.5%, respectively:
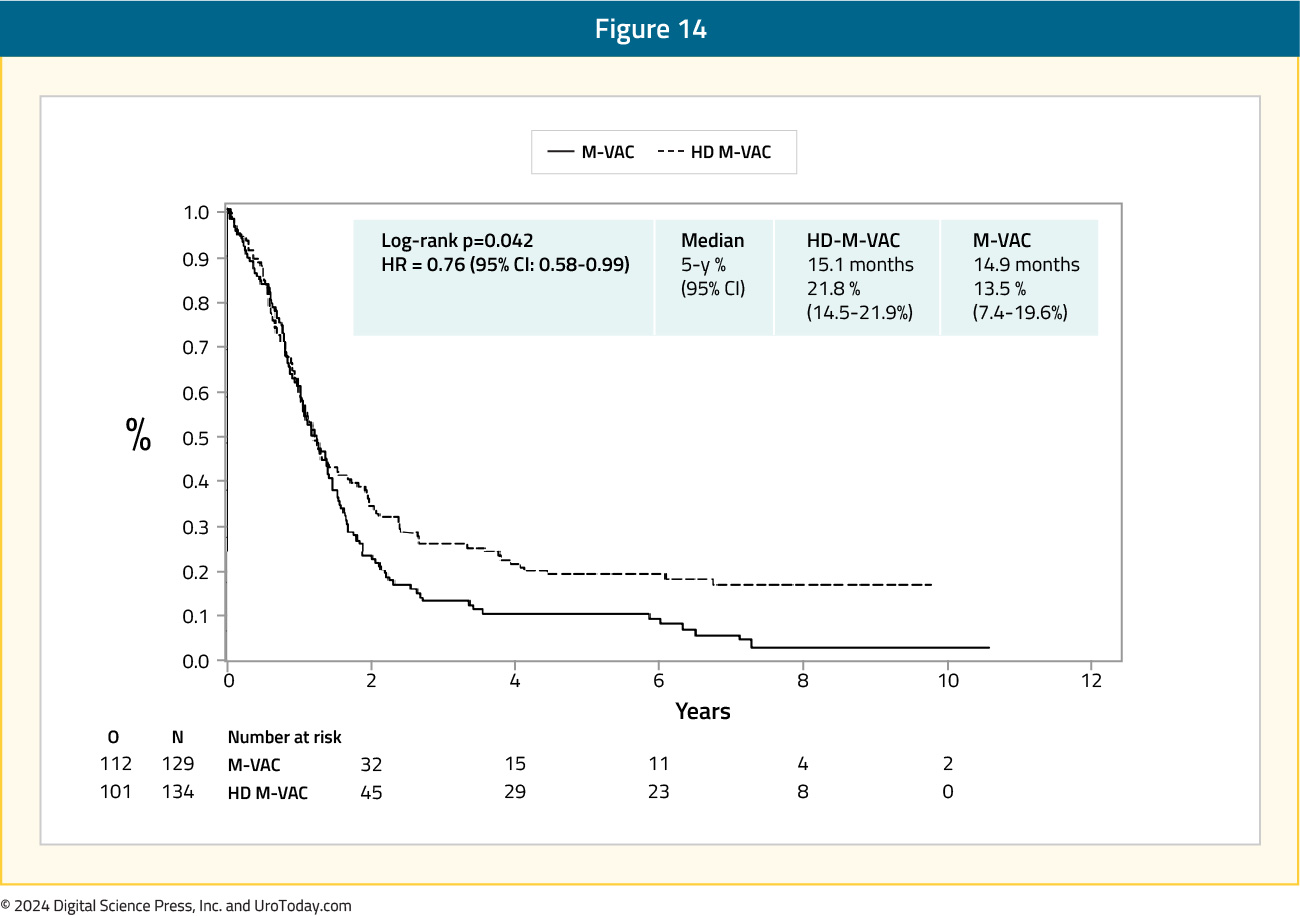
There was one death from toxicity in each arm, and more patients died secondary to malignant disease in the MVAC arm (76%) compared to those in the dose dense MVAC arm (65%). With this longer follow-up for the EORTC 30924 trial, initial results were confirmed showing that dose dense MVAC had a borderline statistically significant relative reduction in the risk of progression and death compared to MVAC.
Real World Evidence of MVAC versus Gemcitabine + Cisplatin
In one of the largest real world evidence assessments of gemcitabine + cisplatin versus MVAC chemotherapy for cisplatin-eligible patients, Lee and colleagues used the Korean National Health Insurance Service database from 2004 to 2016.18 This cohort consisted of 3,108 patients, of which 2,880 received gemcitabine + cisplatin and 228 received MVAC. The use of gemcitabine + cisplatin was the highest in 2013-2016 (37.5%), whereas that of MVAC was highest in 2004-2008 (39.5%). Overall, the 5-year survival rate was 23.4% for the gemcitabine + cisplatin group and 25.0% for the MVAC group, including a median overall survival of 39.6 months and 37 months, respectively:
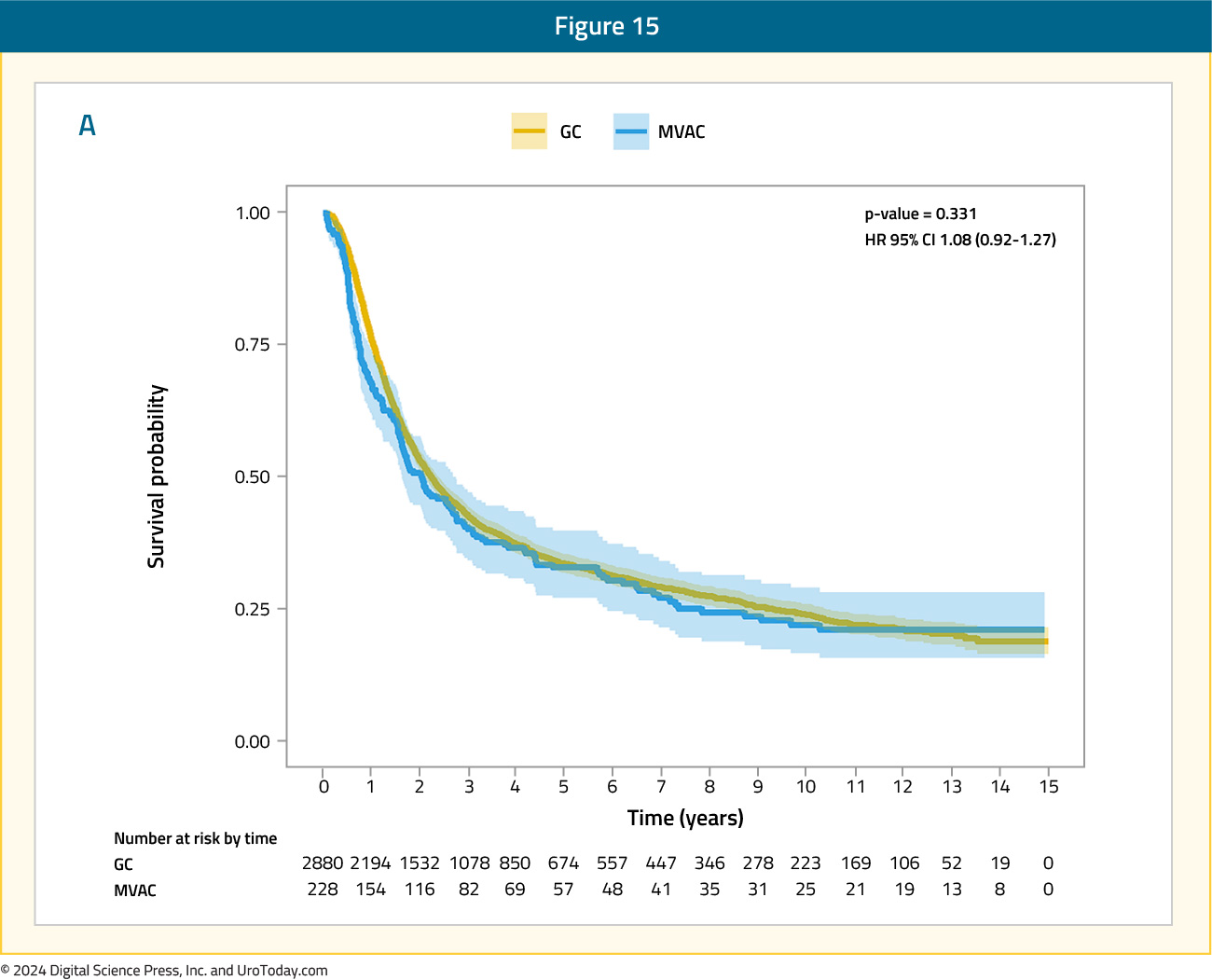
Interestingly, a subgroup analysis revealed that a period of ≥3 months from diagnosis to systemic therapy enhanced the prognostic effects of the gemcitabine + cisplatin regimen (HR: 1.35, 95% CI: 1.04 – 1.74).
Nivolumab + Gemcitabine/Cisplatin
In CheckMate 901, 608 cisplatin-eligible patients underwent 1:1 randomization to either:
- Nivolumab 360 mg on D1 + gemcitabine (1,000 mg/m2) on D1/8 + cisplatin (70 mg/m2) on D1 in 3-week cycles, up to a total of 6 cycles
- Nivolumab maintenance at 480 mg every 4 weeks was continued as maintenance therapy in responders until progression, unacceptable toxicity, withdrawal, or up to 24 months
- Gemcitabine + cisplatin at same doses/schedule/cycles
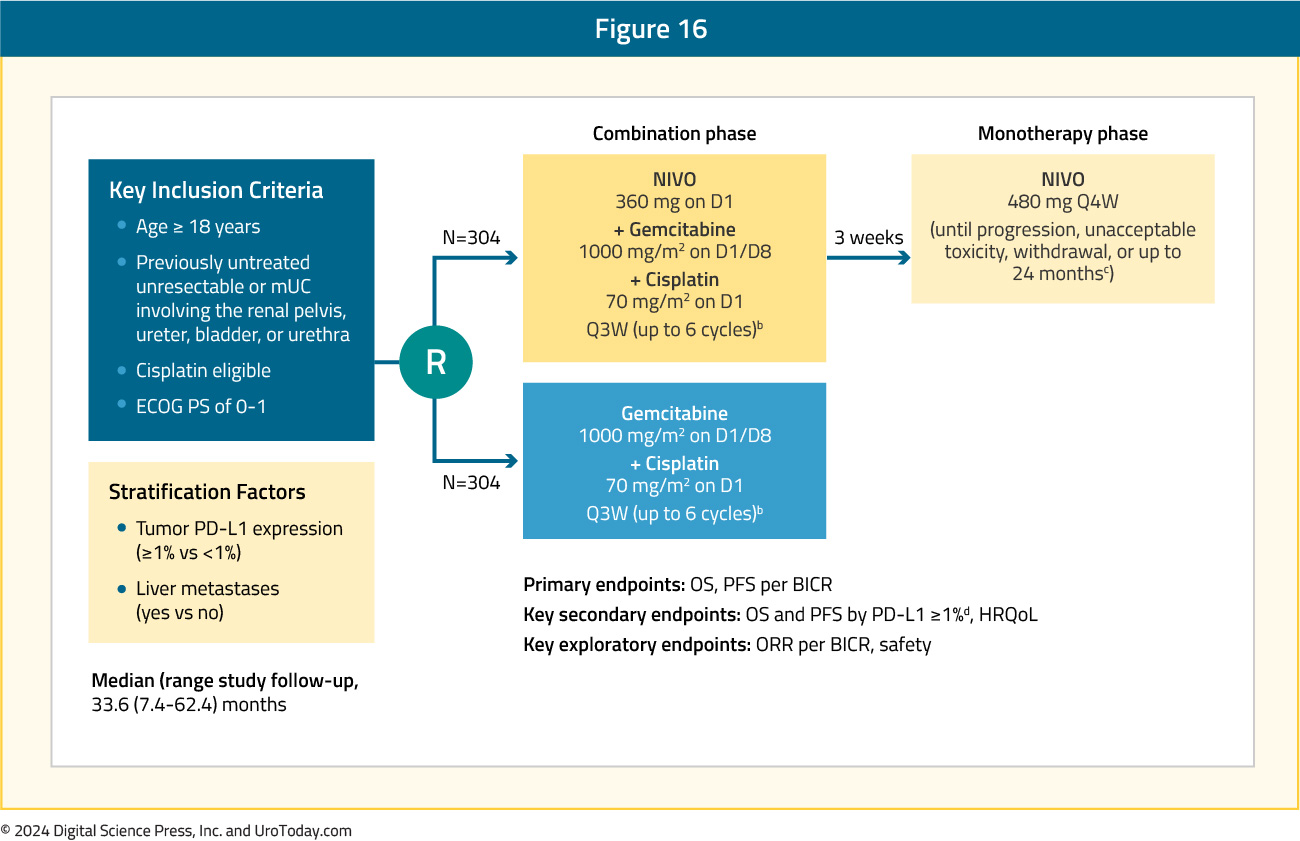
The median patient age was 65 years, and similar to EV-302/KEYNOTE-A39, 25% of patients had upper tract disease. Overall, 37% of patients had a high tumor PD-L1 expression, defined as ≥1%, and 21% of patients had liver metastases.
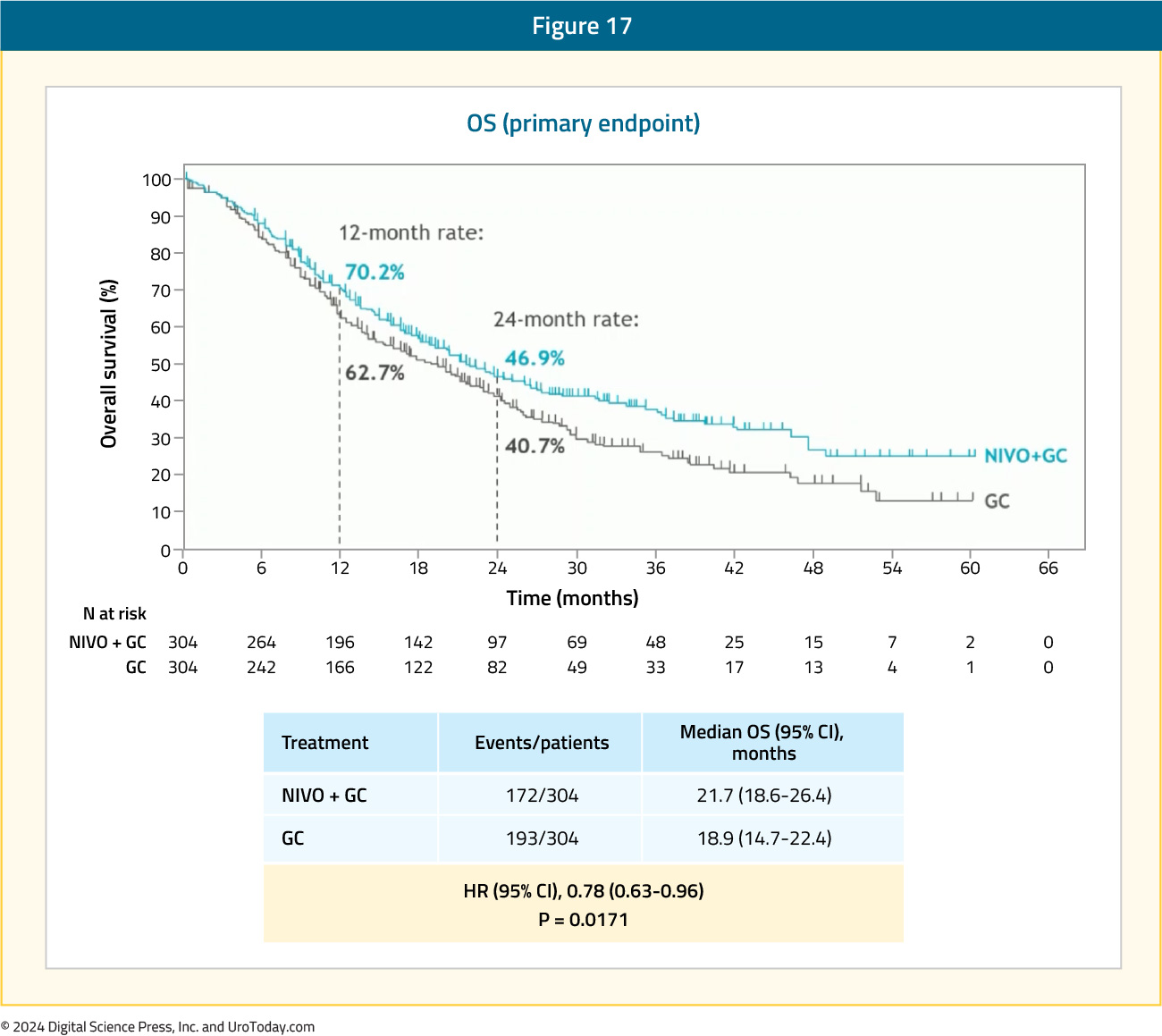
The median study follow-up was 33.6 months, with 74% of patients in the nivolumab + gemcitabine/cisplatin arm completing all 6 cycles of therapy, compared to 55% of those in the control gemcitabine/cisplatin arm. In total, 80% of patients randomized to nivolumab + gemcitabine/cisplatin went on to receive maintenance nivolumab monotherapy.
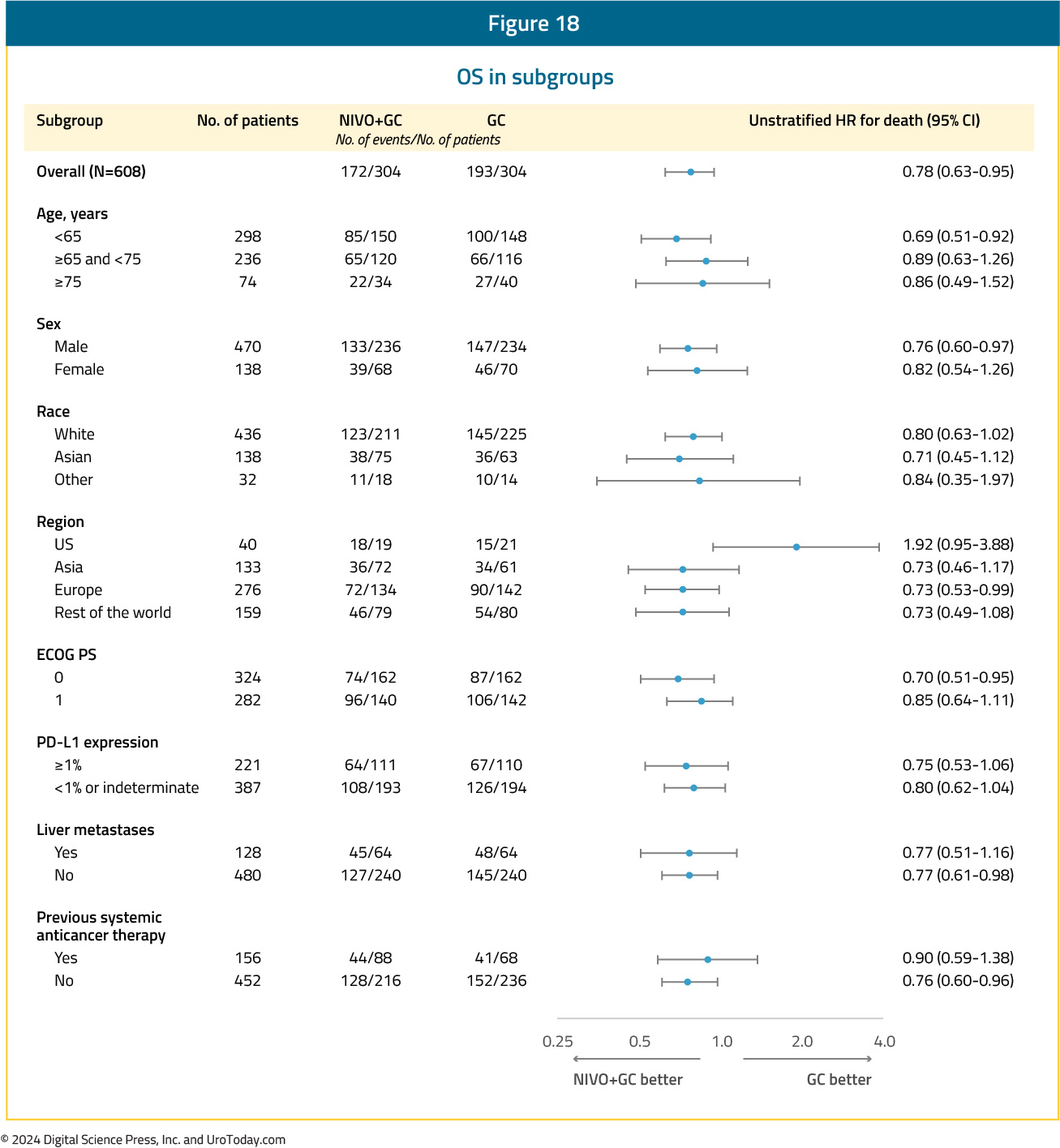
The study met its primary endpoint of OS, with a median improvement of nearly 3 months (21.7 versus 18.9 months; HR: 0.78, 95% CI: 0.63 – 0.96, p=0.017):
OS subgroup analyses favored almost all evaluable subgroups; however, of note, there appeared to be an OS benefit in favor of the gemcitabine/cisplatin control in the US-treated patients (n=40; HR: 1.92, 95% CI: 0.95 – 3.88):
The other co-primary endpoint of PFS per BICR was also significant with improvement in median PFS from 7.6 to 7.9 months (HR: 0.72, 95% CI: 0.59 – 0.88, p=0.0012):

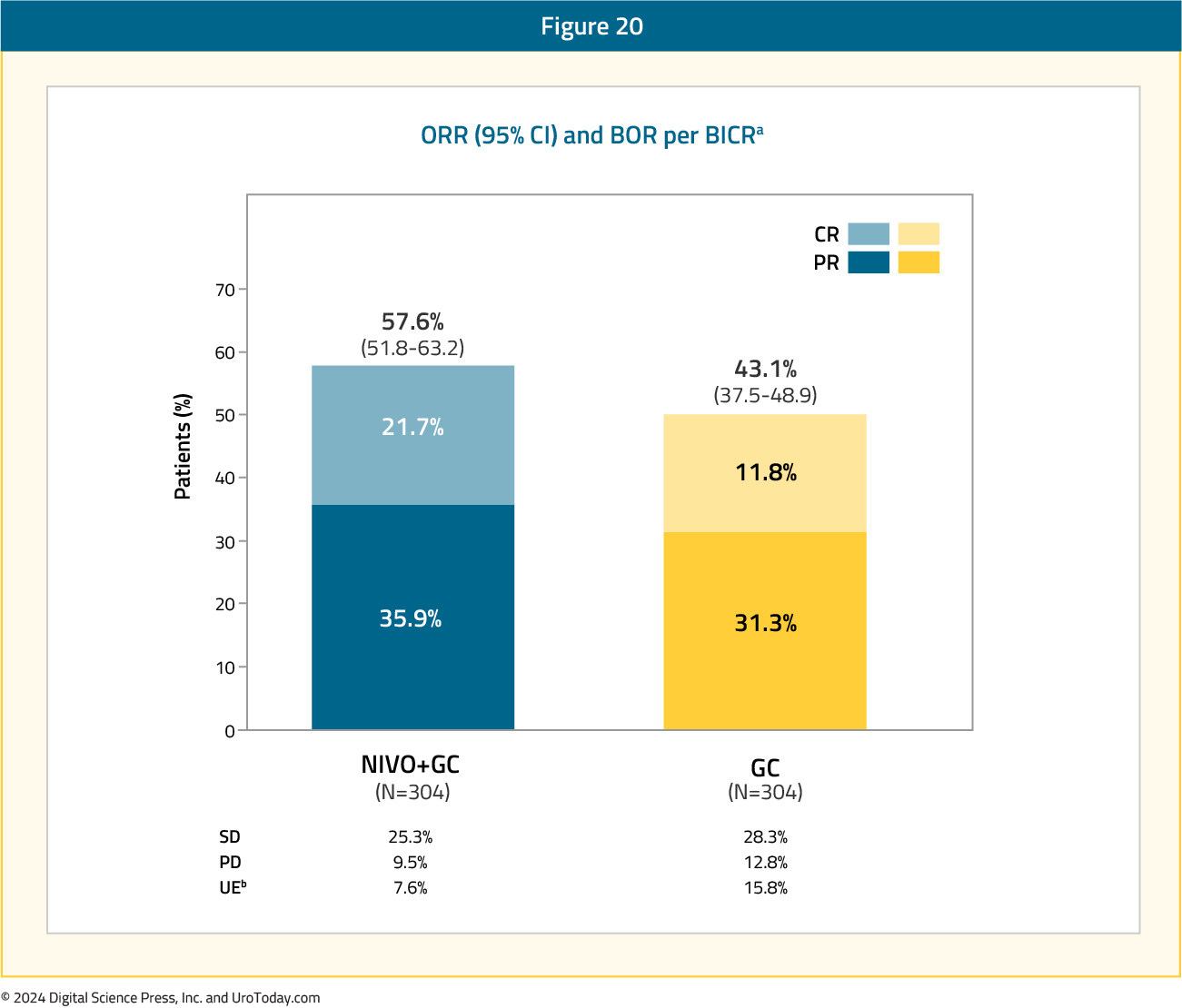
The objective response rate was higher in the experimental arm (58% versus 43%), with a higher proportion of patients achieving a complete response with nivolumab + gemcitabine/cisplatin (22% versus 12%):
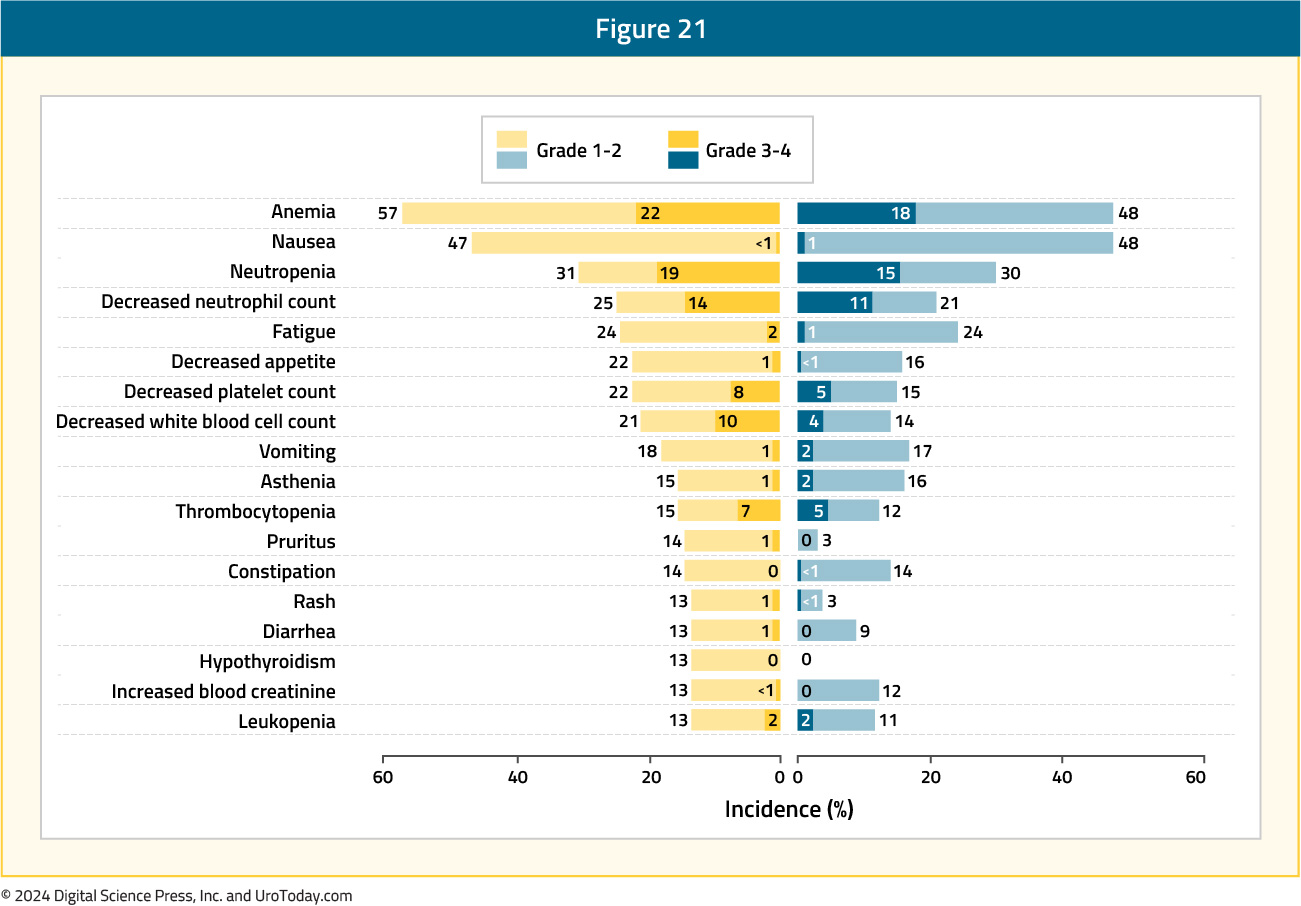
Grade ≥3 TRAEs occurred in 62% and 52% of patients in the experimental and control arms, respectively. Those leading to treatment discontinuation occurred in 11% and 8%, respectively. The most common TRAEs with nivolumab + gemcitabine/cisplatin were anemia (57%), nausea (47%), and neutropenia (31%):
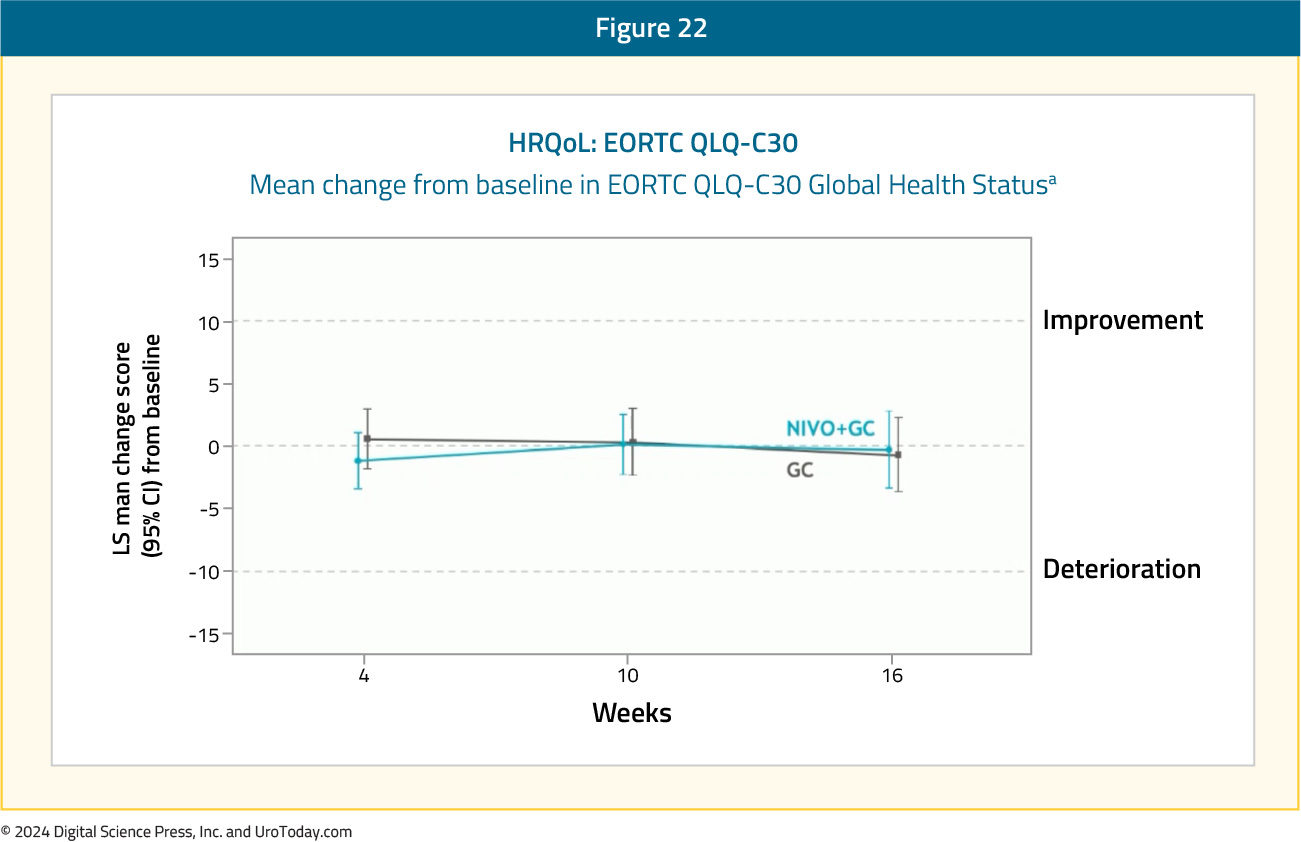
Health related quality of life (EORTC QLQ-C30) was stable and equivalent in both arms:
Avelumab Maintenance Therapy
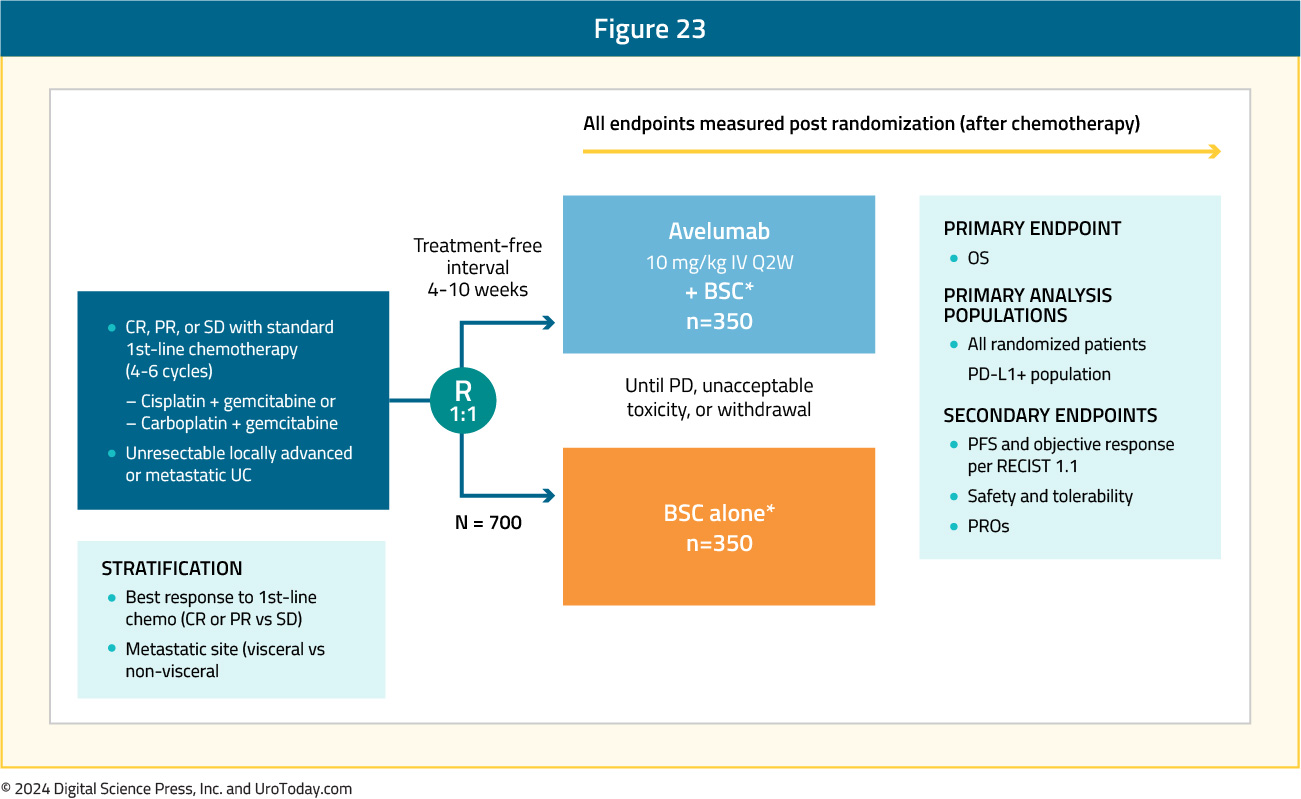
Platinum-based chemotherapy generally shows an objective response in 40-50% of patients and disease control in 75-80% of patients; however, most patients have disease progression in 9 months, with a median overall survival of 14-15 months.2,3 As such, there had long been an unmet clinical need for the treatment of patients who have completed platinum-based chemotherapy (4 – 6 cycles of cisplatin-based chemotherapy) and did not experience disease progression.The JAVELIN Bladder 100 trial was a phase 3 trial that randomly assigned patients with unresectable locally advanced or metastatic urothelial cancer who did not have disease progression with first-line chemotherapy to receive best supportive care with or without maintenance avelumab (10 mg/kg IV every 2 weeks).19 Patients were randomized from May 2016 to June 2019 at 197 sites in 29 countries, with 350 patients in each of the arms. The trial design for JAVELIN Bladder 100 is as follows:
At the time of data cutoff, 24.3% of patients in the avelumab group and 7.4% in the control group were still receiving treatment, with the most common reason for discontinuation being progressive disease (54% in the avelumab group versus 75% in the control group). Furthermore, a subsequent anticancer drug therapy was received by 42.3% of patients in the avelumab group compared to 61.7% of patients in the control group.
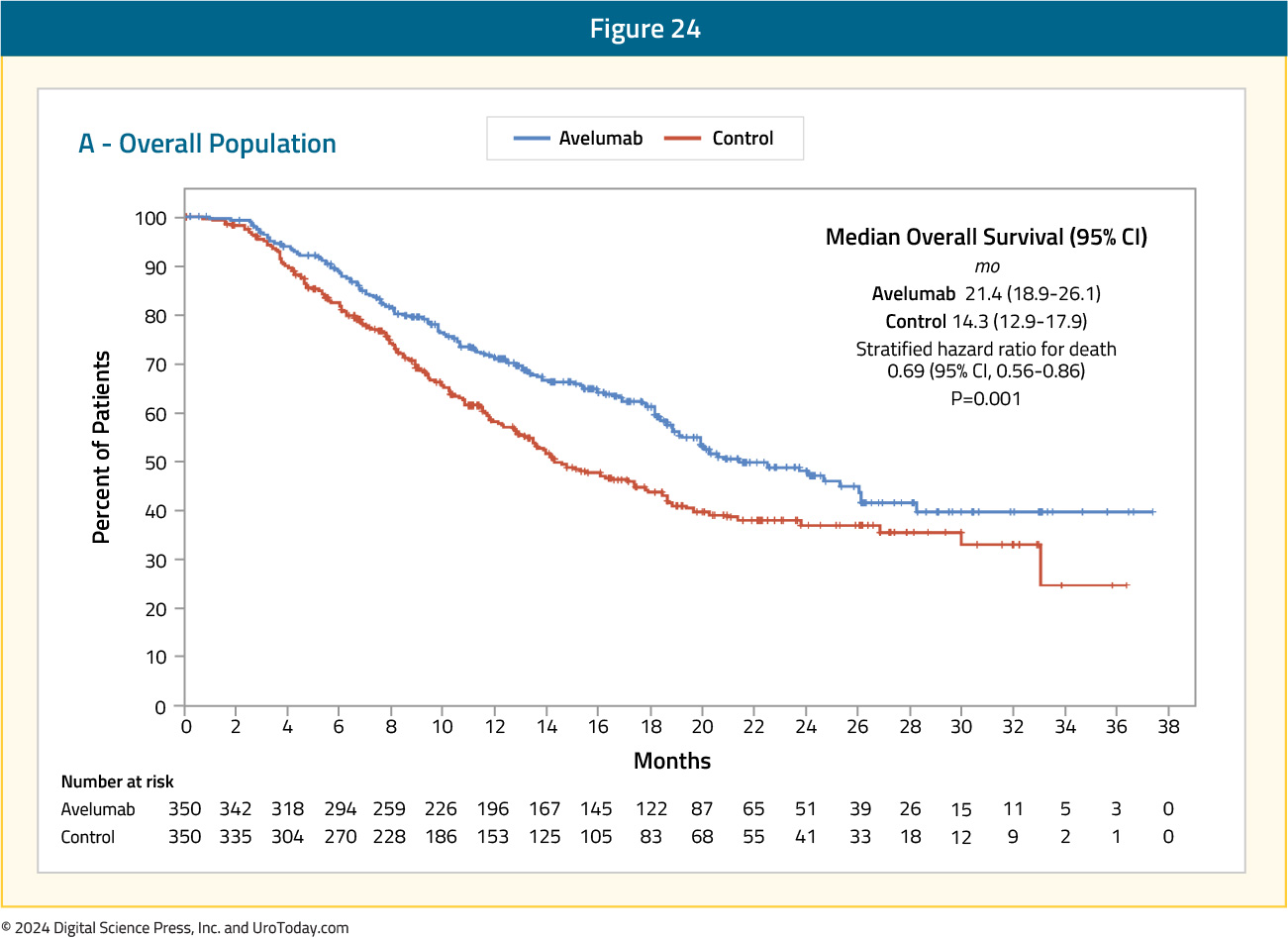
Overall survival at 1 year was 71.3% (95% CI 66.0 – 76.0) in the avelumab group compared to 58.4% (95% CI 52.7 – 63.7) in the control group, with a median overall survival of 21.4 months and 14.3 months, respectively (HR 0.69, 95% CI 0.56 – 0.86):
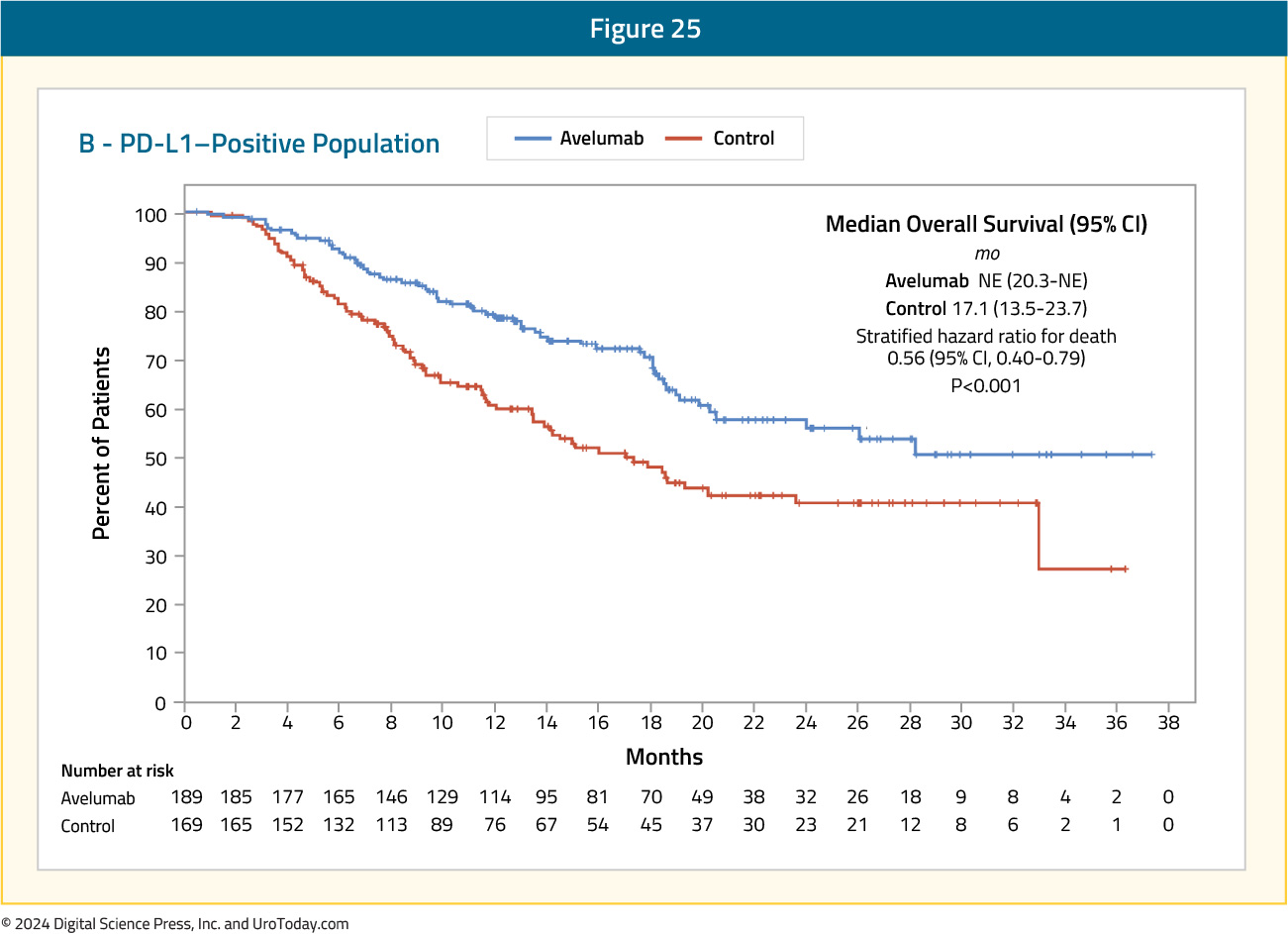
An overall survival benefit favoring avelumab was even more pronounced in the PD-L1 positive population (HR 0.56, 95% CI 0.40 – 0.79):
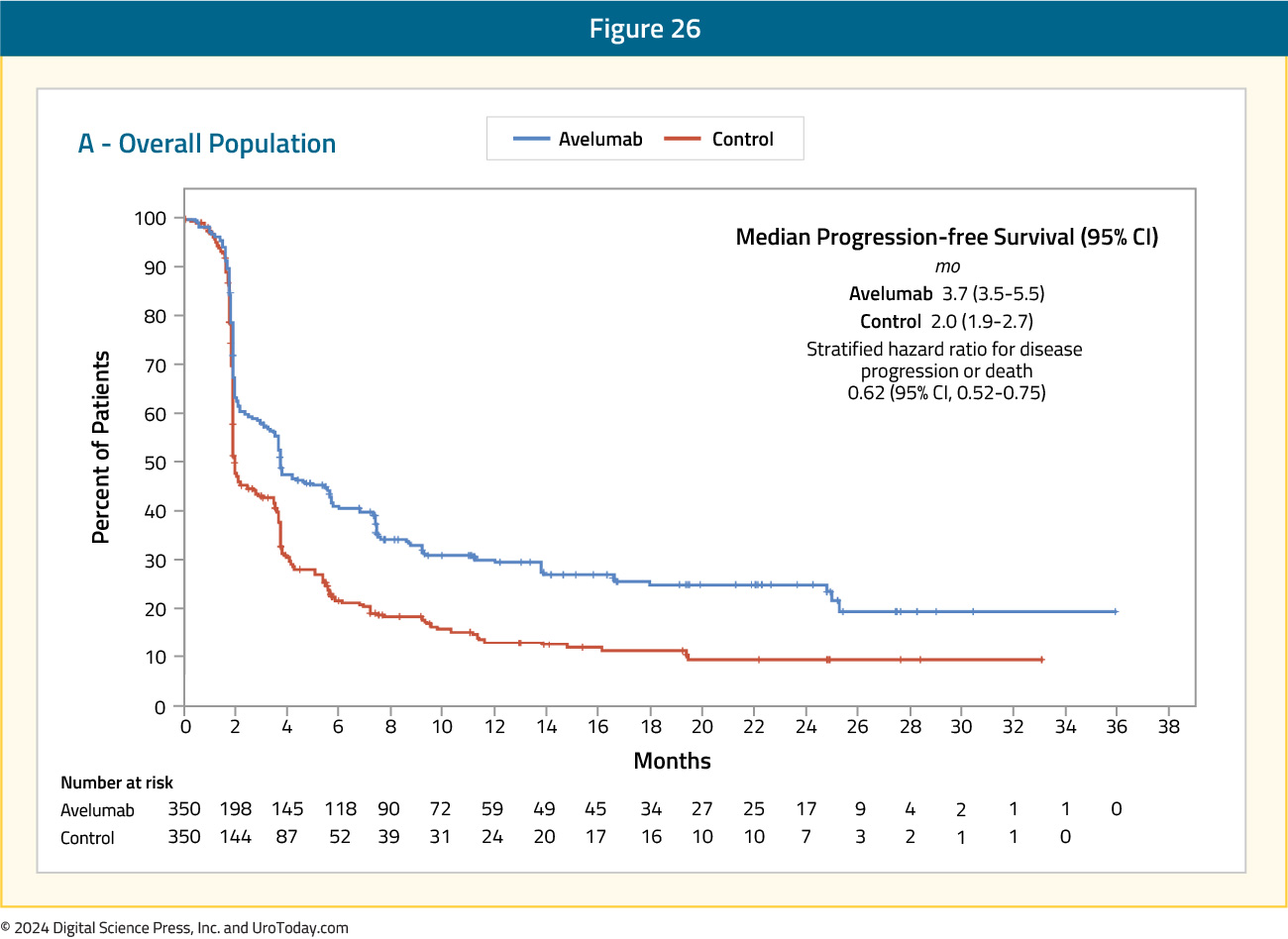
The key secondary endpoint in this trial was progression free survival, which was also longer in the avelumab group, with a median of 3.7 months (95% CI 3.5 – 5.5) compared to 2.0 months (95% CI 1.9 – 2.7) in the control group (HR 0.62, 95% CI 0.52 – 0.75):
This progression free survival benefit for avelumab was also evident in the PD-L1 positive population (HR 0.56, 95% CI 0.43 – 0.73). Grade 3 or worse adverse events occurred in 47% of patients receiving avelumab compared to 25% of patients in the control group, with adverse events leading to discontinuation occurring in 12% of patients in the avelumab group. The most frequent category of immune-related adverse events was thyroid disorders, which occurred in 12% of patients.
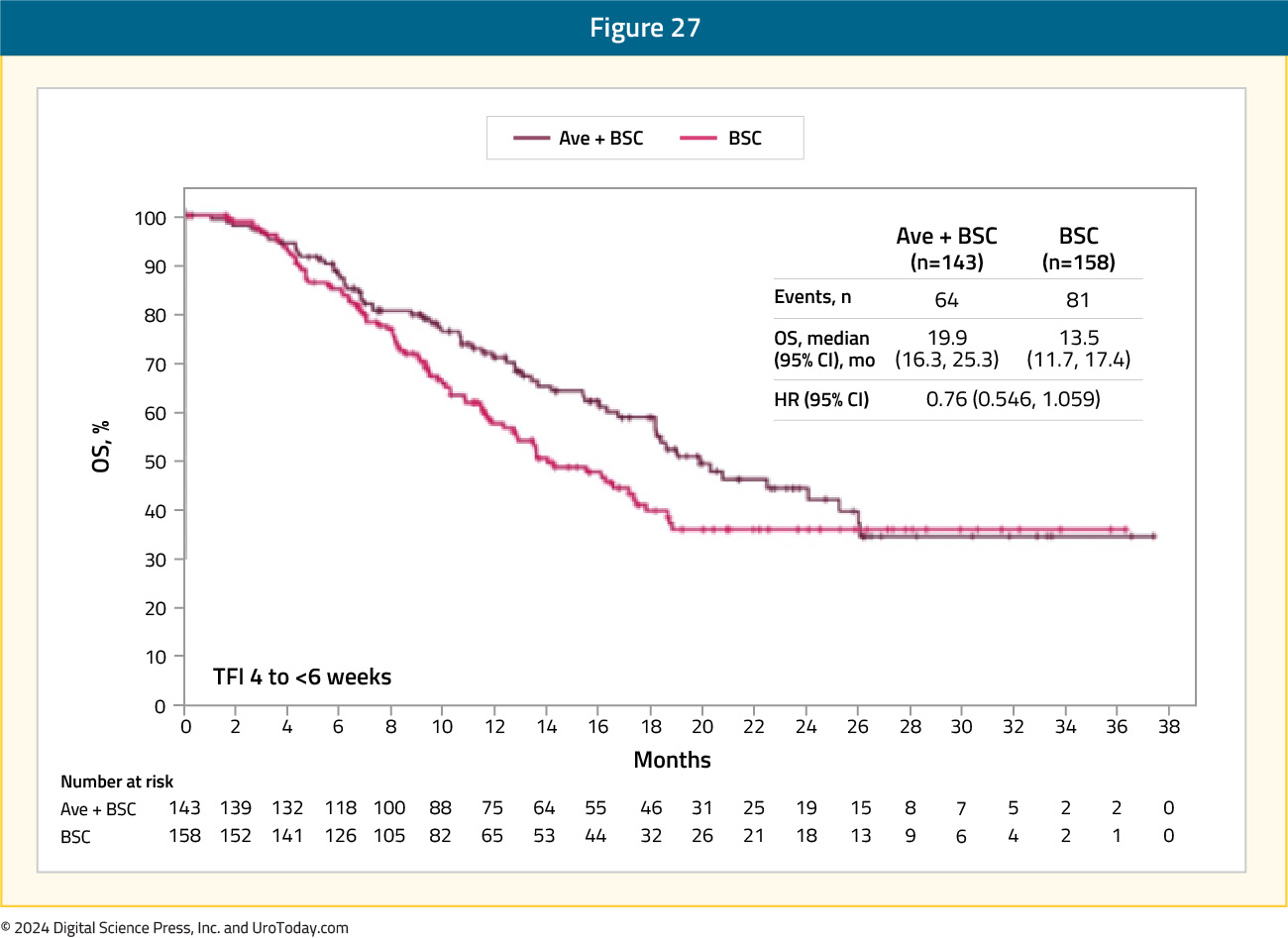
Since the publication of this landmark trial in the New England Journal of Medicine, there have been several additional analyses presented at international conferences. At the ASCO 2021 annual meeting, Dr. Srikala Sridhar presented a subgroup analysis by duration of treatment-free interval from the end of chemotherapy to the start of maintenance. In the avelumab and control group arms, the treatment-free interval was 4 – 6 weeks in 143 and 158 patients, 6 – 8 weeks in 109 and 80 patients, and 8 – 10 weeks in 98 and 110 patients, respectively. For both arms combined, however, the treatment-free interval 4 – 6 weeks subgroup, as compared to the other two subgroups, included significantly more patients with:
- Visceral metastases (58% vs 54% and 50%)
- An objective response with first-line chemotherapy (76% vs 69% and 68%)
- An ECOG performance status of 1 (45% vs 33% and 36%).
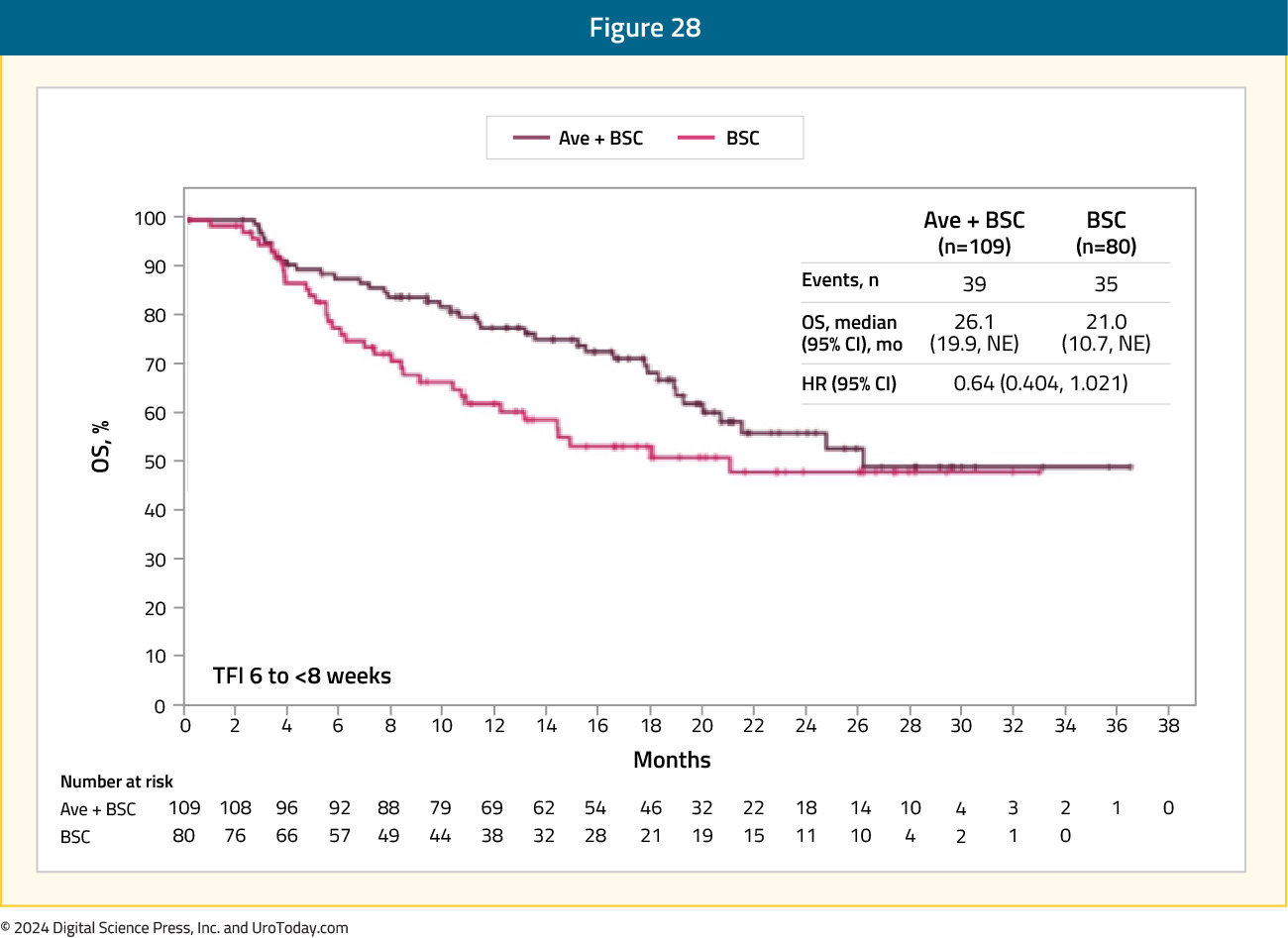
In the 6 – 8 weeks subgroup, the HR was 0.64 (95% CI: 0.40 to 1.02), with median OS of 26.1 and 21 months, respectively:
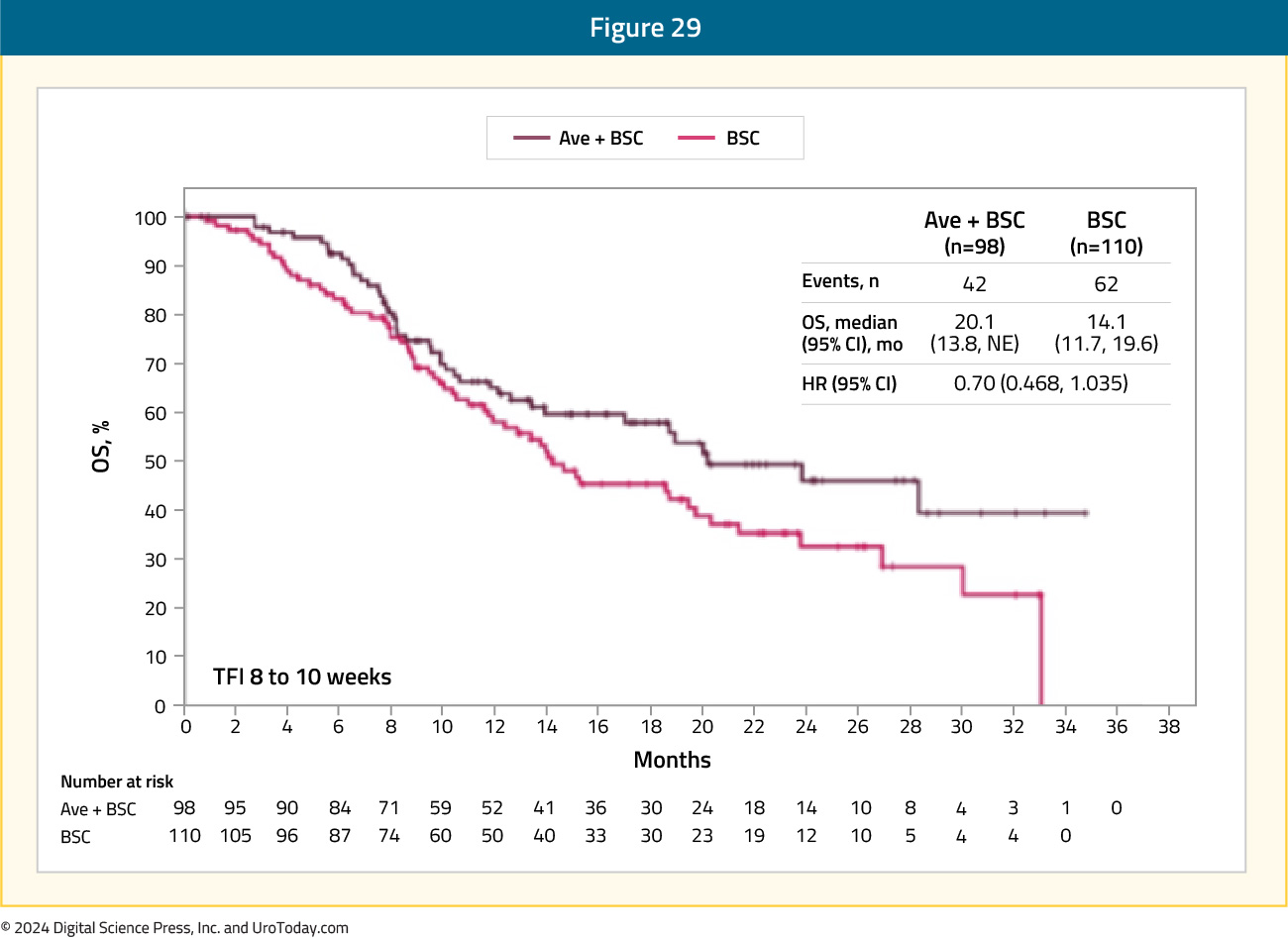
In the 8 – 10 weeks subgroup, the HR was 0.70 (95% CI: 0.47 – 1.04), with median OS of 20.1 and 14.1 months, respectively:
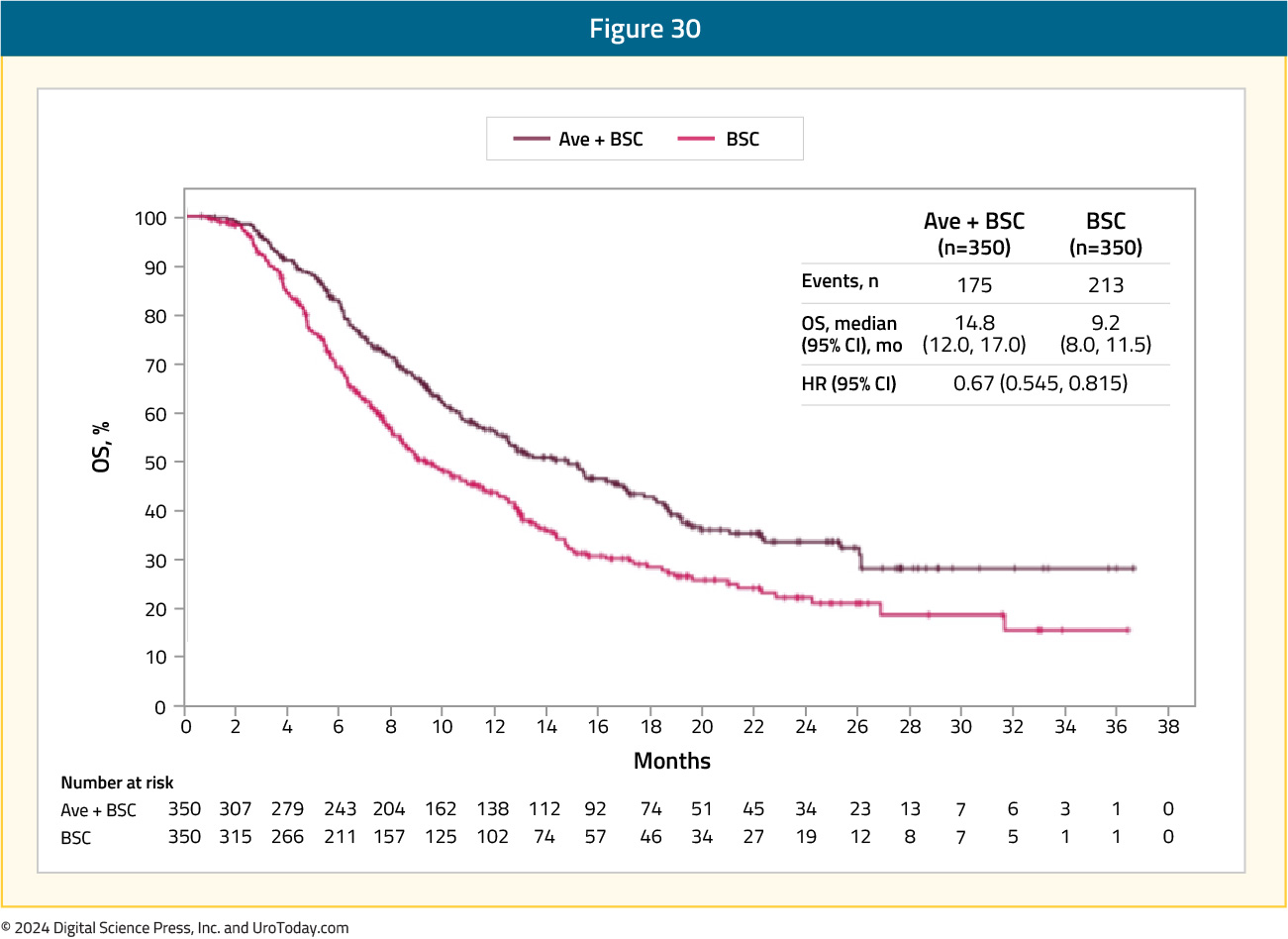
Also presented at ASCO 2021, by Dr. Petros Grivas, was a subgroup analysis of time to end of next-line of therapy. Importantly, time to next-line of therapy was analyzed as an alternative to the second progression-free survival (PFS2) endpoint, which could not be analyzed because progression on next-line therapy was not assessed in the trial population. Among all randomized patients, time to end of next-line therapy was prolonged in the avelumab arm (median 14.8 months) versus the control arm (median 9.2 months; HR 0.67, 95% CI 0.55 – 0.82):
Time to end of next-line therapy was prolonged in the avelumab, irrespective of PD-L1 status:
- PD-L1+: 18.1 versus 9 months (HR 0.61, 95% CI 0.45 – 0.82)
- PD-L1-: 11.9 versus 9.3 months (HR 0.76, 95% CI 0.56 – 1.04)
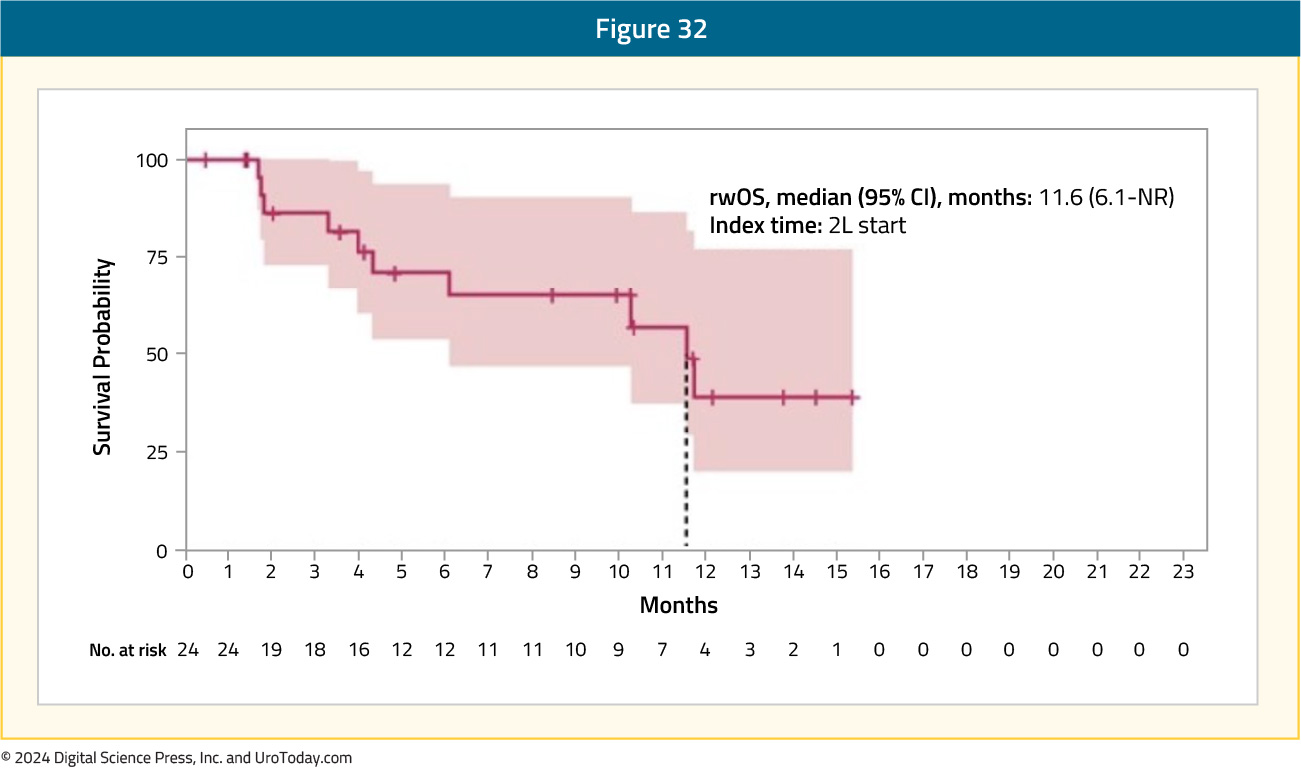
At ESMO 2023, Dr. Kenneth Carson presented real-world outcomes and treatment patterns of avelumab first-line maintenance therapy, using the Tempus database from 2016 to 2023. There were 3,299 patients identified as receiving avelumab, of which 1,939 (59%) received 1st line systemic therapy. Of the 1,939 patients, 974 (50.2%) completed 1st line therapy, with platinum-based chemotherapy the most common 1st line regimen (66%). The median follow-up from the start of 1st line platinum-based chemotherapy was 10.2 months, and the median OS was 13.6 months. Real-world OS landmark analysis from 1st line maintenance initiation demonstrated that 80% of avelumab 1st line maintenance patients were still alive at 6 months and 63% were alive at 12 months. The median PFS from 1st line maintenance start was 6.4 months and the median time on treatment was 3.9 months. After 1st line maintenance avelumab, 35% of patients received 2nd line treatment. 70% of whom received enfortumab vedotin, with a median OS from the start of 2nd line treatment of just under 12 months:
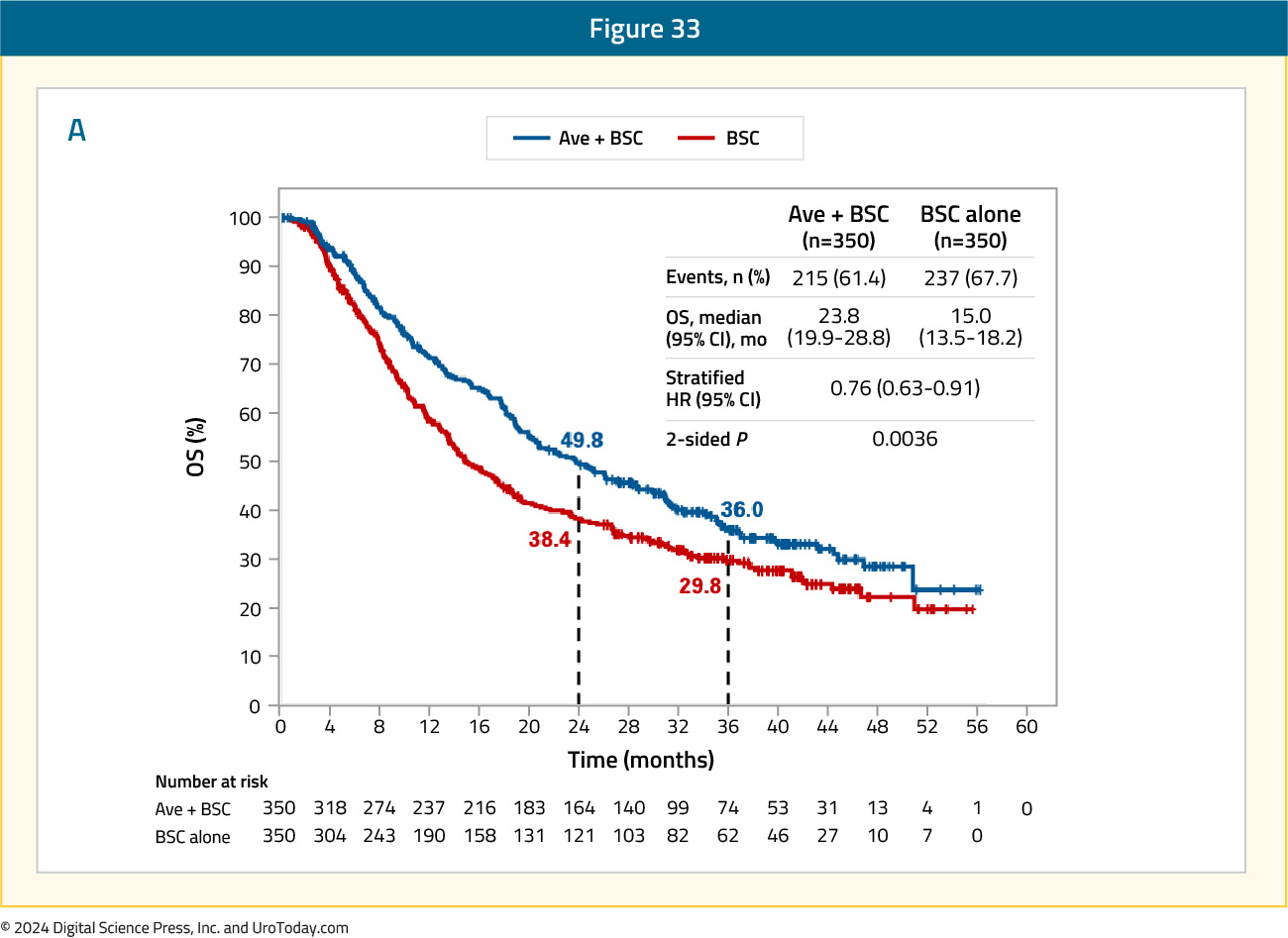
Also presented at ESMO 2023, and subsequently published in the Journal of Clinical Oncology, Powles et al.20 reported results of the JAVELIN Bladder 100 trial after ≥2 years of follow-up. At the time of the data cutoff for this analysis (June 4, 2021), the median follow-up was 38 months for patients receiving avelumab versus 39.6 months for those in the control arm. Of note, almost 20% of patients had received ≥2 years of avelumab maintenance therapy. In this extended analysis, OS remained prolonged with avelumab, with a median survival of 23.8 months (95% CI 19.9 – 28.8) versus 15 months (95% CI 13.5 – 18.2) for the control arm (HR 0.76, 95% CI 0.63 – 0.91):
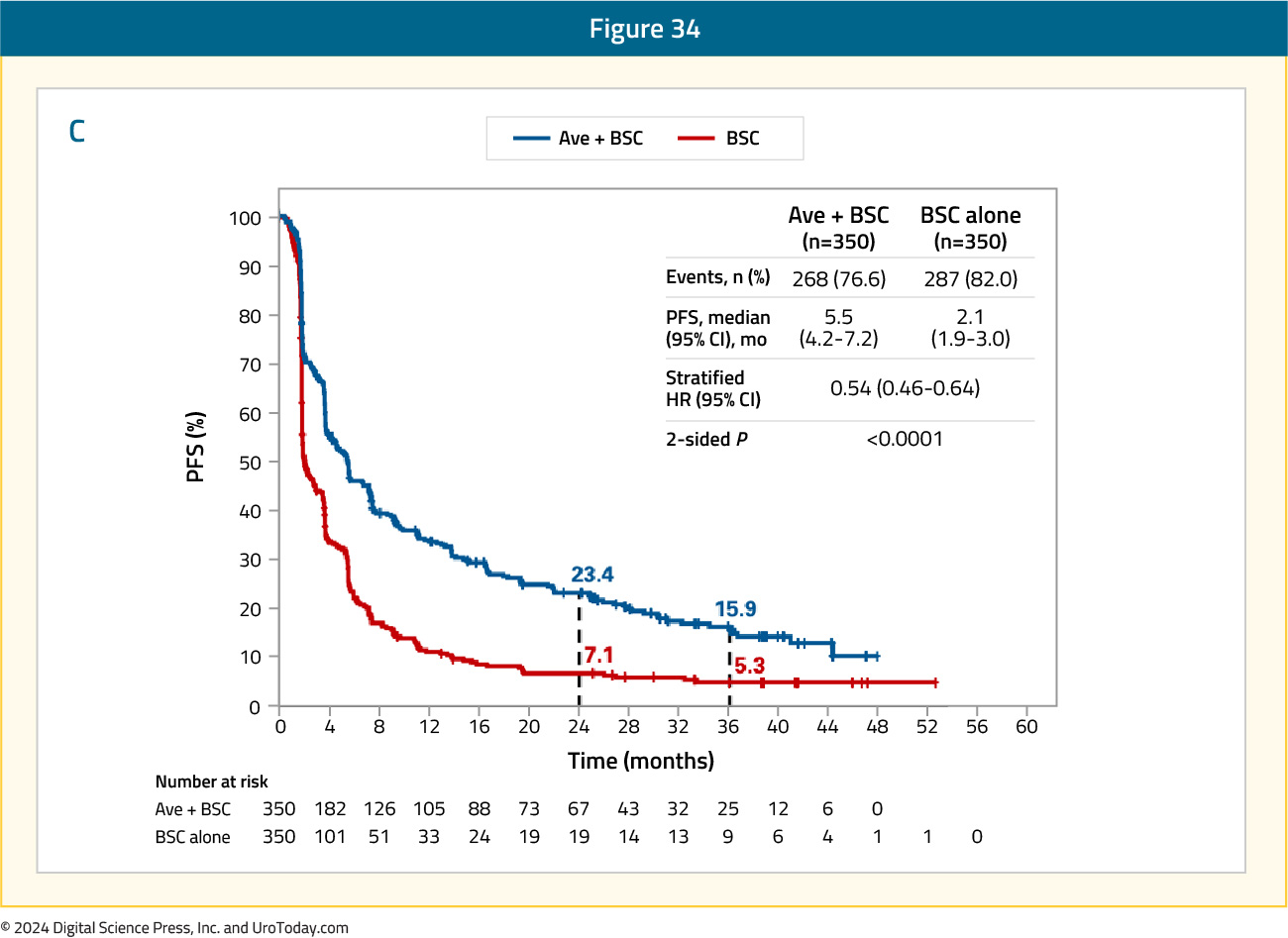
Additionally, investigator-assessed progression free survival remained prolonged for patients receiving avelumab, with a median of 5.5 months (95% CI 4.2 – 7.2) versus 2.1 months (95% CI 1.9 – 3.0) in the control arm (HR 0.54, 95% CI 0.46 – 0.64):
Among responders, the median duration of response was 28.4 months (95% CI 15.9 – 42.3) in the avelumab arm and 26.9 months (95% CI 4.4 to not estimable) in the control arm.
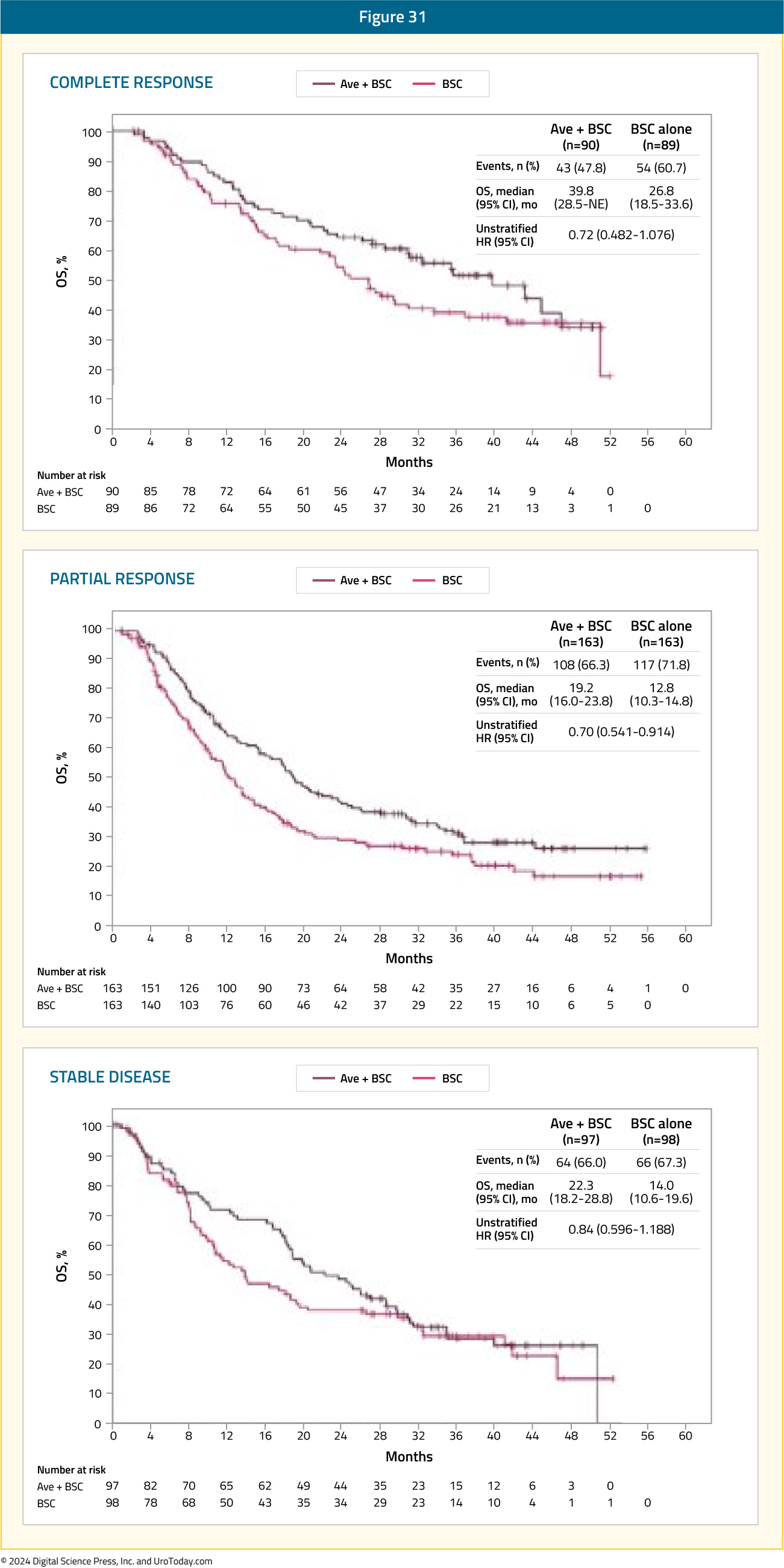
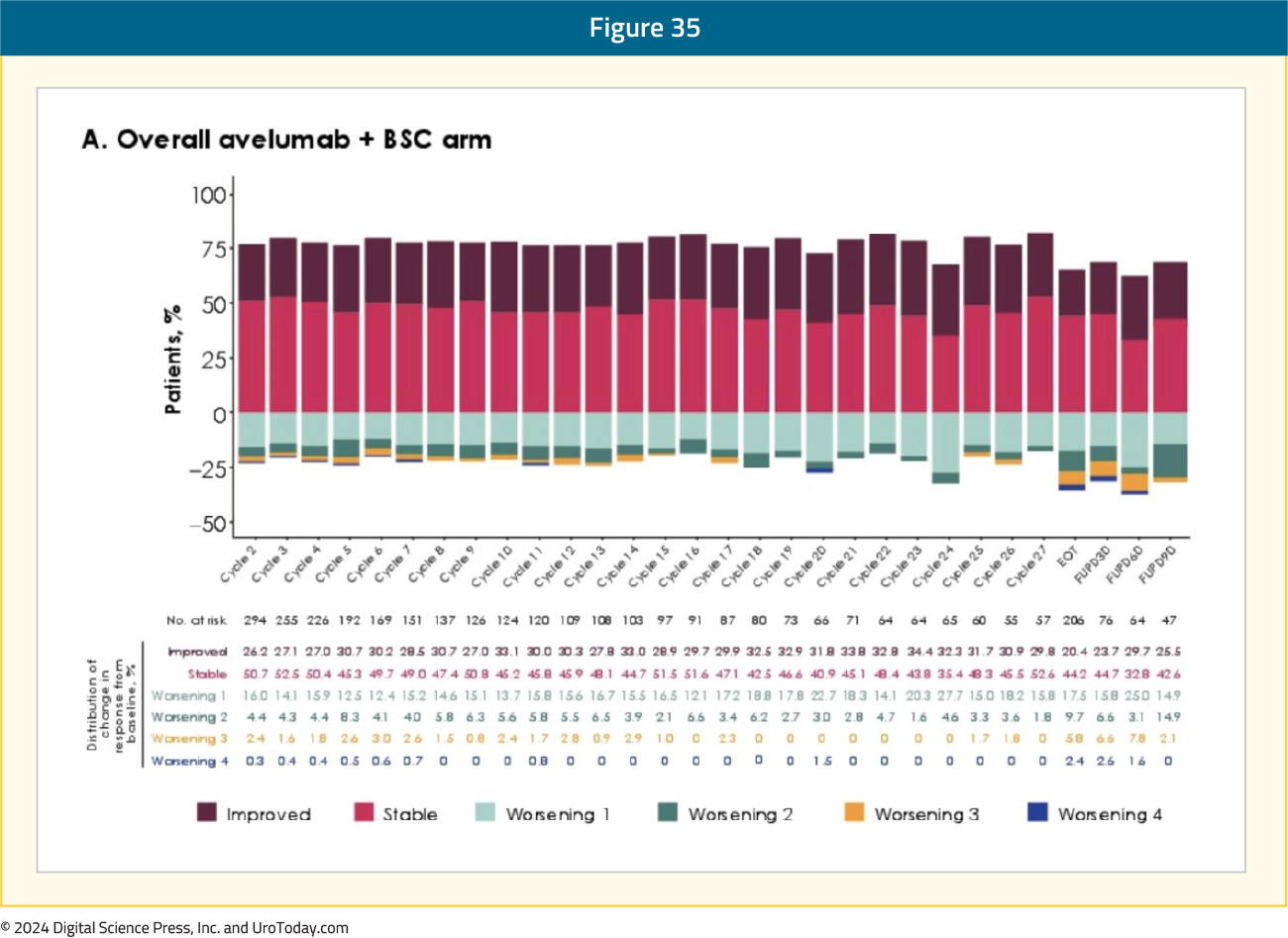
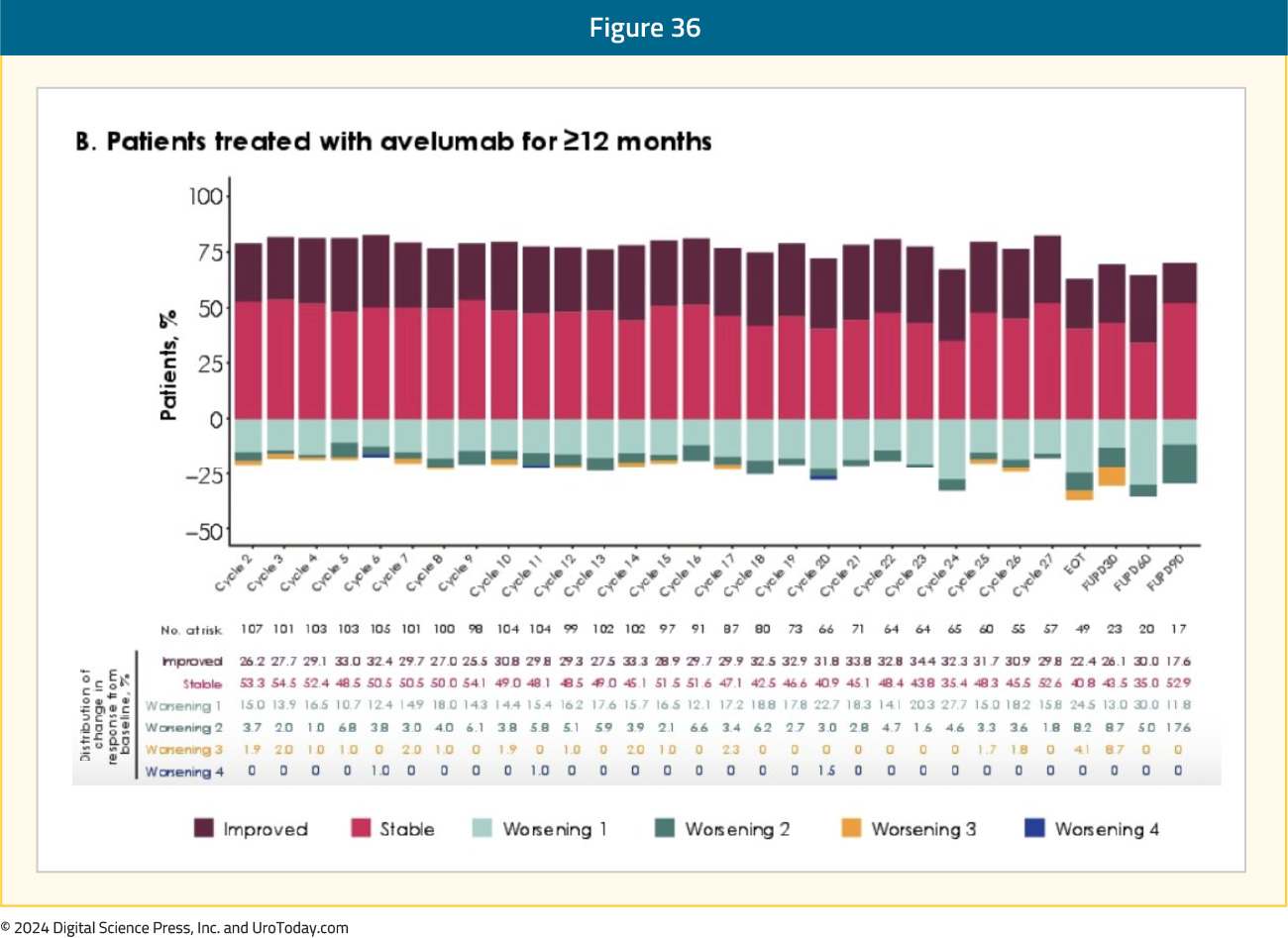
Finally, presented at ASCO GU 2024, Dr. Petros Grivas reported long-term patient reported outcomes from JAVELIN Bladder 100, including a subgroup with ≥12 months of avelumab treatment. In patients treated for ≥12 months (n=118 [34%]]), baseline characteristics were similar to those of patients in the overall avelumab + best supportive care arm, except for a higher proportion with ECOG performance status 0 (70% versus 61%) and PD-L1+ tumors (61% versus 54%), and a lower proportion with visceral metastases (48% versus 55%). On average, PRO scores remained stable throughout treatment, and no clinically important changes from baseline were reported. In the overall avelumab + BSC arm and in patients treated with avelumab for ≥12 months, approximately 75% of evaluable patients reported no change or a decrease in how much they were bothered by treatment side effects throughout 24 months of treatment:
In addition to the efficacy outcomes highlighted above for JAVELIN Bladder 100, this trial also has provided an enriched biomarker population that will hopefully further guide treatment. Powles and colleagues reported that the avelumab survival benefit was associated with PD-L1 expression by tumor cells, tumor mutational burden, APOBEC mutation signatures, expression of genes underlying innate and adaptive immune activity, and the number of alleles encoding high-affinity variants of activating Fcy receptors.21 Although individual biomarkers did not identify patients who may benefit from therapy, this analysis represents new opportunities to enrich patient therapies based on a personalized strategy and inform future clinical trial design.
Conclusions and Future Directions
The combination of enfortumab vedotin + pembrolizumab has emerged as the primary choice for the first line treatment of patients with locally advanced/metastatic urothelial carcinoma patients, regardless of cisplatin eligibility. This combination is associated with a median overall survival of 32 months, which is twice as long as that observed with platinum-based combination chemotherapy regimens. While the addition of nivolumab to gemcitabine/cisplatin does improve overall survival by nearly 3 months in cisplatin eligible patients, this benefit pales in comparison to that observed with enfortumab vedotin + pembrolizumab.The emergence of this novel combination alters the treatment landscape for patients with metastatic urothelial carcinoma and raises some important questions that will be the subject of future research:
- Does platinum-based combination chemotherapy become the treatment of choice in the 2nd line setting following disease progression with enfortumab vedotin + pembrolizumab? The efficacy and safety of platinum-based combination chemotherapy will need to be evaluated in this setting.
- What is the maintenance therapy of choice for patients without evidence of disease progression with enfortumab vedotin + pembrolizumab? Is continued enfortumab vedotin monotherapy the choice in this setting as was performed in EV-302/KEYNOTE-A39?
- Enfortumab vedotin ($30,739.50 per 28-day cycle for 70-kg person) and pembrolizumab ($10,268.72 per 21-day cycle for 200 mg dose) are both considerably more expensive than gemcitabine ($282/cycle) and cisplatin ($87/cycle). Will insurance providers approve these regimens for all patients with metastatic urothelial carcinoma or will approval be limited to those with the most aggressive disease features (e.g., high volume, liver metastases)? Will this combination prove to be cost-effective in future studies and will this drug get approved/adopted in publicly funded, universal healthcare systems?
- What are the implications in the neoadjuvant setting? The Phase 3 KEYNOTE-B15/EV-304 trial (NCT04700124) is randomizing 784 patients with clinically localized, muscle invasive bladder cancer to either peri-operative enfortumab vedotin + pembrolizumab (4 neoadjuvant cycles, radical cystectomy + pelvic lymph node dissection, followed by 5 adjuvant cycles of enfortumab vedotin and 13 cycles of pembrolizumab) versus 4 cycles of neoadjuvant gemcitabine/cisplatin (no adjuvant therapy following surgery).