In 2016, the manufacturer of the Connaught strain of bacillus Calmette-Guerin (BCG) announced that it would discontinue BCG production effective 2017. This left a single manufacturer of BCG, and when they had a batch contamination in 2012, there was no available BCG for a period of time leading to rationed use and lower doses.
In this abstract, the authors utilize the National Cancer Database to evaluate utilization trends of BCG for NMIBC during this time frame, to examine its impact on BCG utilization. They included patients with urothelial carcinoma, stages Ta, T1, or CIS, without nodal or metastatic disease.
They identified 292,446 patients with NMIBC from 2004-2014. Overall, 13.8% of patients with NMIBC received intravesical BCG during the study period. BCG utilization was highest among patients with CIS and HG pT1 disease. The figures below demonstrate trends in BCG utilization over time and by pT stage.
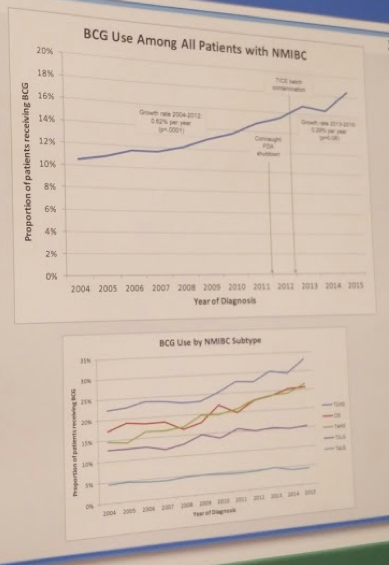
There was a notable decrease in the rate of rise of BCG utilization following major supply interruptions in 2011 and 2012 (2004-2012: 0.47% increase per year [p<.0001]; 2012-2014: 0.03% increase per year [p=0.83]).
As appropriate they highlight the need for increased supply of BCG, in the event of another shortage, as there is a large bottleneck in the supply chain. This, again, would leave a large volume of patients with HG NMIBC without effective therapy.
Presented by: Abhinav Khanna, MD
Co-Authors: Abhinav Khanna MD MPH¹, Nitin Yerram MD¹, Hui Zhu MD PhD², Simon Kim MD MPH³ and Robert Abouassaly MD MSc²
Affiliation: ¹Cleveland Clinic; ²Cleveland Clinic and Louis Stokes VA Medical Center; ³University Hospital Medical Center
Written by: Thenappan Chandrasekar, MD, Clinical Fellow, University of Toronto, twitter: @tchandra_uromd at the 18th Annual Meeting of the Society of Urologic Oncology, November 20-December 1, 2017 – Washington, DC