(UroToday.com) At the 2020 Société Internationale d'Urologie (SIU) virtual annual meeting Dr. Peter Black hosted a multidisciplinary session assessing the management of early-stage bladder cancer with thought leaders including Dr. Jurgen E. Gschwend, Dr. Shilpa Gupta, Dr. Srikala Sridhar, and Dr. Tilman Todenhofer.
Dr. Todenhofer started by discussing the evolving treatment of high-risk non-muscle-invasive bladder cancer. Bacillus Calmette-Guerin (BCG)-unresponsive disease is defined as the following:
- Persistent or recurrent carcinoma in situ (CIS) alone or with recurrent Ta/T1 (noninvasive papillary disease /tumor invades the subepithelial connective tissue) disease within 12 months of completing adequate BCG therapy, defined as one of the following (i) At least five of six doses of an initial induction course plus at least two or three doses of maintenance therapy, (ii) At least five of six doses of an initial induction course plus at least two of six doses of a second induction course.
- Recurrent high-grade Ta/T1 disease within 6 months of completion of adequate BCG therapy
- T1 high-grade disease at the first evaluation following an induction BCG course
Until recently, the only Federal Drug Administration (FDA)-approved agent in the BCG unresponsive setting was valrubicin. In the key study,1 there were 80 patients with CIS, 39% with at least 2 prior courses of BCG. Treatment included 6 or 9 weeks of valrubicin, and at 3 months 35% of patients had no evidence of disease (positive cytology allowed). The complete response rate at 6 months was 18% and the disease-free rate at 2 years was 4%. Gemcitabine has also been used in the BCG unresponsive disease space. The SWOG S0353 phase II trial assessed intravesical gemcitabine for BCG refractory NMIBC, which included 58 patients enrolled in the trial and 47 evaluable for response.2 At the initial 3-month evaluation, 47% of patients were free of disease, at 1 year disease had not recurred in 28% of patients, all except 2 from the high-risk group, and at 2 years disease had not recurred in 21% of patients. More recently, there have been promising results for the combination of gemcitabine plus docetaxel.3 There were 276 patients (38% that were BCG unresponsive) that received treatment and had a median follow-up of 22.9 months. The 1-year recurrence-free survival rate was 60% and the and 2-year recurrence-free survival rate was 46%. Specific to high-grade recurrence, the 1-year recurrence-free survival rate was 65% and 2-year was 52%. Overall, there were 10 patients (3.6%) that had disease progression on transurethral resection, and 43 patients (15.6%) went on to cystectomy (median 11.3 months from induction), of whom 11 (4.0%) had progression to muscle invasion.
Other options include vicinium (oportuzumab monatox), which is being evaluated in several cohorts: (i) Cohort 1: CIS with or without papillary tumors that recurred within 6 months of BCG, (ii) Cohort 2: CIS with or without papillary tumors that recurred >6 months but less than 11 months of BCG. The trial schema is as follows:
The primary endpoint is complete response rate (defined as negative urine cytology, pathology, and local cystoscopy) and duration of response in cohort 1. Key secondary endpoints include event free survival in all subjects, time to disease recurrence, time to cystectomy, progression-free survival, overall survival, safety and tolerability. In the most recent analysis of this data presented at AUA 2020, the complete response rate at 3 months among patients with CIS was 40%, and the median duration of response was 9.4 months.
Another phase III registry trial that was recently presented looked at nadofaragene firadenovec, an intravesical gene therapy. This trial had 157 patients with BCG-unresponsive disease and included a single, one-hour intravesical administration (which may be repeated every 3 months up to 12 months). Among 103 patients with CIS, the complete response rate (primary endpoint) was 53.4%, with all complete responses being achieved within 3 months of treatment, and 24.3% of patients have 12-month high-grade recurrence-free survival. For 48 patients with papillary disease, 72.9% of patients had 3-month high-grade recurrence-free survival, which was durable at 12 months (43.8%).
Checkpoint inhibitors have also been tested in phase II trials in the BCG unresponsive disease space. Presented at ASCO 2020, the SWOG S1605 trial tested systemic atezolizumab (1200 mg IV) every 3 weeks for one year with a primary endpoint of pathological complete response rate at 6 months as defined by mandatory biopsy.4 There were 75 eligible CIS patients enrolled of which 74 were evaluable. A complete response was observed in 41.1% of patients (95% CI 29.7%-53.2%) at 3 months and 26.0% (95% CI 16.5%-37.6%) at 6 months. Also presented at ASCO 2020 was two-year follow-up of the KEYNOTE-057 trial assessing pembrolizumab among patients with BCG unresponsive disease.5 Among 96 patients included in the efficacy analysis the complete response rate was 40.6% (95% CI 30.7-51.1), and median duration of response was 16.2 months (range, 0+ to 30.4+). For the 39 patients with a complete response, 18 (46.2%) had a duration of response of ≥12 months. At 12 months, progression-free survival (PFS) was 82.7% and overall survival (OS) was 97.9%. As follows is a side by side comparison of SWOG S1605 and KEYNOTE-057:
Dr. Todenhofer then highlighted important follow-up data from the KEYNOTE-057 trial, presented as part of the two-year data summary. A total of 36 patients (37.5%) underwent radical cystectomy after discontinuation from study treatment, which included 9 of 22 patients (40.9%) who had recurrence after initial complete response and 27 of 57 (47.4%) nonresponders. Of the 36 who underwent radical cystectomy, 33 (91.6%) had no pathological upstaging to muscle-invasive disease, whereas only 3 (8.3%) patients had at least pT2 disease at the time of cystectomy. Dr. Todenhofer provided the following summary table of the future choices of treatment in BCG-unresponsive non-muscle-invasive bladder cancer:
In addition to these new modalities, there are ongoing trials including targeted therapies in NMIBC. For example, THOR 2 is testing erdafitinib versus investigator choice of intravesical chemotherapy in participants who received prior BCG and recurred with high-risk NMIBC. The trial schema for THOR 2 is as follows:
With the current BCG shortage globally, Dr. Todenhofer notes that there are also ongoing clinical trials assessing immune checkpoint therapy for BCG-naïve patients. Indeed, BCG shortages have an impact on outcome. In a recently published study from Lee et al.,6 among 333 patients, 94 (28.2%) experienced BCG shortage. The 3-year recurrence-free survival rate was significantly lower in the shortage group than that in the control group (38.0% vs. 60.2%, log-rank test, p = 0.010). Furthermore, in multivariable analysis, BCG shortage (HR 1.55, 95% CI 1.09-2.21, p = 0.016) was an independent factor associated with the recurrence of bladder cancer.
The importance of adequate BCG doses has recently been confirmed in the recently published NIMBUS trial.7 The standard BCG schedule was 6 weeks of induction followed by 3 weeks of maintenance at 3, 6, and 12 months (15 instillations), and the reduced frequency BCG schedule was induction at weeks 1, 2, and 6 followed by 2 weeks (weeks 1 and 3) of maintenance at 3, 6, and 12 months (nine instillations). As follows is the trial design for NIMBUS: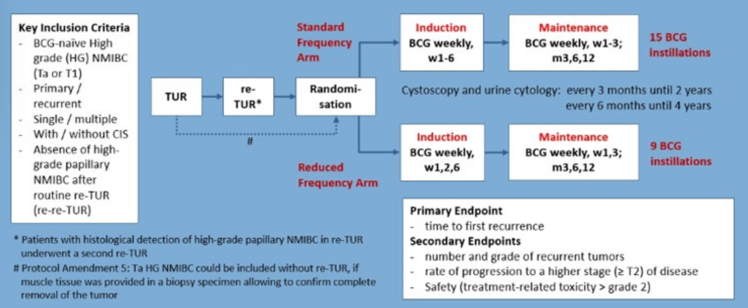
There were 170 patients were randomized to reduced frequency and 175 to standard BCG. After 12 months of median follow-up, the intention-to-treat analysis showed a safety-relevant difference in recurrences between treatment arms: 46/170 (reduced frequency) versus 21/175 patients (standard). Additional safety analyses showed a hazard ratio of 0.40 with the upper part of the one-sided 97.5% confidence interval of 0.68, meeting a predefined stopping criterion for inferiority.
Dr. Todenhofer concluded this presentation of high-risk NMIBC treatment options with the following take-home messages:
- There is significant dynamics in the development of drugs for the treatment of BCG-unresponsive NMIBC
- Systemic immunotherapy agents and novel intravesical drugs provide a meaningful benefit for a subgroup of patients
- Agents with success in the BCG-unresponsive setting may impact treatment of BCG-naïve high-risk NMIBC
- Identification of predictive factors is essential to determine the subgroups of patients that may undergo a bladder sparing approach
Dr. Jurgen Gschwend then presented a case of BCG-unresponsive disease for discussion. First, he notes that there are several indications for cystectomy, with the chance for cure decreasing as the disease progresses, as summarized in the following figure:
This case included a 65-year-old former teacher with no significant medical history and no history of smoking. He subsequently had an episode of gross hematuria and dysuria, with a urinalysis showing 250+ erythrocytes, as well as positive cytology. An office-based flexible cystoscopy was performed, which showed papillary and flat lesions at the right bladder wall mucosa suspicious for Cis or Ta high grade urothelial cancer. The patient then had a fluorescent TURBT with Hexvix instillation one hour before the procedure, pathology demonstrating Ta high-grade urothelial cancer with surrounding Cis, no signs of a submucosal invasion. Muscle fibers were present in the specimen without tumor invasion, thus no second TURBT was planned. Additionally, the upper urinary tract was negative based on contrast-enhanced CT imaging. Dr. Gschwend then posed the following treatment options to the panel:
- BCG induction and re-biopsy?
- BCG maintenance for 1 or 3 years?
- Intravesical chemotherapy?
- Nerve-sparing radical cystectomy and urinary diversion?
Dr. Black noted that he would treat this patient with BCG induction and three years of maintenance therapy. He typically re-biopsies the CIS patients after 6 months (BCG induction plus first round of maintenance), since you do see some delayed responses in these patients.
Regarding the possibility of intravesical chemotherapy, Dr. Gschwend asked Dr. Todenhofer if there is a role for intravesical mitomycin chemotherapy. In this patient’s situation he would favor BCG induction with 3 years of maintenance rather than mitomycin given the superior data for BCG in this high-risk patient. If there was a BCG shortage, he would use mitomycin. Dr. Black notes that there is really no role for immediate nerve-sparing cystectomy for this patient, but suggests that he may do it for a young patient with T1 + CIS disease.
The patient subsequently underwent BCG induction with a weekly instillation schedule and re-biopsy was scheduled for 6 weeks after the last instillation. Dr. Gschwend then posed the following questions to the panel:
- At what time do you plan the first re-biopsy?
- Do you do re-biopsy by TURBT, cold-cup biopsy or both?
- What is the role of cytology or FISH (UroVysion)?
- What maintenance schedule do you recommend?
Dr. Todenhofer stated that he typically re-biopsies after three months, favoring a complete re-induction for those with persistent CIS. However, Dr. Black argues that he does not typically re-induce these patients if the patient has persistent CIS at the time of re-biopsy. Dr. Todenhofer notes that when he does a re-biopsy, he typically does a full re-TURBT whereas Dr. Black may prefer to use cold cup biopsies only. Dr. Gschwend makes the important point that in patients with CIS only disease, he will typically do cold-cup mapping biopsies of the whole bladder. Dr. Todenhofer prefers cytology over UroVysion in follow-up of his patients with CIS, as does Dr. Black who does cytology at each interval cystoscopy (also noting that FISH UroVysion is not available in Canada).
This patient then underwent re-biopsy 6 weeks after the last BCG dose, with cold cup biopsy and TURBT revealing persistent CIS and some papillary tumor with high-grade features. As such the following treatment options were discussed with the patient
- Nerve-sparing radical cystectomy with orthotopic neobladder
- BCG re-induction course and re-biopsy at 3-4 months
- Weekly instillation with gemcitabine
- Inclusion in clinical study KEYNOTE-676: BCG plus pembrolizumab versus BCG
Dr. Gschwend notes that the KEYNOTE-676 trial is a phase II trial studying the efficacy of pembrolizumab in combination with BCG in patients with persistent or recurrent high-risk NMIBC following BCG induction therapy. The trial design for this study is as follows:
For this patient, Dr. Black notes that a nerve-sparing radical cystectomy is likely premature, given that he is not yet BCG unresponsive and it would be reasonable to continue with BCG. If the recurrence were T1 disease he states that he would certainly push for a cystectomy. If there is no available clinical trial, Dr. Gschwend notes that particularly in a young patient, he is quite likely to perform a nerve-sparing radical cystectomy.
Dr. Sridhar then presented on new paradigms in the multimodal management of muscle-invasive bladder cancer. For these patients, staging is important, including a TURBT plus CT of the chest/abdomen/pelvis. Dr. Sridhar notes that understaging remains a major issue and can lead to suboptimal treatment; additionally, novel imaging like PET/CT may also improve the detection of disease. One study ongoing in Ontario is the PETMUSE clinical trial that is assessing the utility of PET-CT in staging of muscle-invasive patients. The trial design for this study is as follows:
The management for muscle-invasive disease is typically either radical cystectomy with lymph node dissection or trimodality therapy. The optimal candidates for bladder sparing trimodality therapy are those with no hydronephrosis, no extensive or multi-focal CIS, tumors <6 cm, and tumors that are amenable to a visually complete or maximally debulked TURBT. In a propensity score analysis of radical cystectomy versus bladder sparing trimodal therapy from the University of Toronto, they found that over a median follow-up of 4.5 years, the death rate was 38% for radical cystectomy compared to 39% for those undergoing trimodal therapy.8 Furthermore, the 5-year DSS rates were 73% for radical cystectomy and 76% for trimodal therapy. Bladder sparing is now recommended by the NCCN guidelines based on a growing body of literature.
With regard to systemic therapy, neoadjuvant chemotherapy is the standard of care. Cisplatin-based regimens improve overall survival, treating both local disease and micrometastatic disease. Furthermore, those patients that get a pathological complete response have better survival outcomes. Dr. Sridhar notes that neoadjuvant chemotherapy uptake is higher in centers with a multidisciplinary approach, optimally with the entire team seeing the patient on the same office visit. However, many patients are not candidates for neoadjuvant chemotherapy, which highlights the need for novel neoadjuvant strategies.
Immune checkpoint inhibitors are approved in the metastatic setting, so there has been interest for their role in the neoadjuvant setting. The phase II ABACUS study was presented at ASCO 2018, which investigated two cycles of atezolizumab (1200mg every three weeks) prior to radical cystectomy among patients with T2-4N0M0 urothelial carcinoma.9 The co-primary endpoints for the study were pathological complete response occurring in ≥20% of patients, and increase in CD8 count as a biomarker analysis. There were 74 patients that received atezolizumab (n=59 received two cycles; n=15 received one cycle). Among these patients, 67 underwent subsequent radical cystectomy. Among the seven patients not receiving surgery was one patient with disease progression (treated with chemotherapy) who was included in the analysis of the primary efficacy endpoint (n=68). The median age of the 68 patients was 71 years (range 53-85), and the baseline pT2 rate was 71%, pT3 was 22%, and pT4 was 7%. The pathologic complete response rates were as follows:
- All patients: 20/68 (29%) – pT0, n=16; pTis, n=4
- PD-L1 positive patients: 10/25 (40%)
- PD-L1 negative patients: 5/31 (16%)
- cT2 patients: 17/48 (35%)
- cT3-T4 patients: 3/20 (15%)
The PURE-01 study recently published updated results in European Urology.10 PURE-01 is a phase II, open-label, single-arm study, assessing three courses of 200 mg pembrolizumab preceding radical cystectomy among patients with T2-4aN0M0 MIBC patients. Among 114 patients were enrolled the pT0 rate was 37% (95% CI 28-46) and the pT ≤ 1 rate was 55% (95% CI 46-65). Importantly, pathologic complete response rates with neoadjuvant immunotherapy are similar to cisplatin-based neoadjuvant chemotherapy, as highlighted in the following figure:
However, whether this will translate similarly to improved survival and whether these agents can be used prior to bladder sparing remains to be seen. Indeed, there is great interesting into incorporating immune checkpoint inhibitors into bladder-sparing strategies, with several ongoing clinical trials: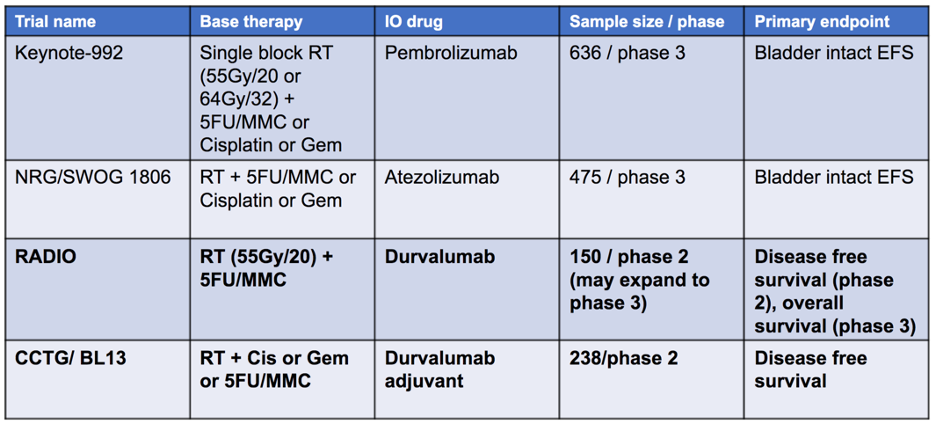
In the adjuvant setting, the IMvigor010 trial was recently presented at ASCO 2020. In this trial, patients with high-risk disease, defined as pathologic ≥T2 disease, or ≥T3 muscle-invasive disease without neoadjuvant chemotherapy, or any patient with node-positive disease were included. Atezolizumab was given every 3 weeks for 1 year in the treatment arm, and patients were assessed with scans every 12 weeks for the first three years, and every 24 weeks for years 4-5. Among 809 patients randomized to treatment or observation, the study did not meet its primary endpoint, as there was no significant difference in DFS between atezolizumab and observation. The median DFS for atezolizumab was 19.4 months, compared with 16.6 months with observation (HR 0.89, 95% CI 0.74-1.08). Although this was a negative study, the pivotal, phase 3 CheckMate-274 trial evaluating nivolumab after surgery in patients with high-risk MIBC met its primary end points of improving DFS versus placebo in both all randomized patients and in patients whose tumor cells expressed PD-L1 ≥1% (press release September 25, 2020).
Dr. Sridhar concluded her presentation of systemic therapy for MIBC with the following key take home messages:
- A multidisciplinary approach to MIBC is critical
- We need to consider both radical cystectomy and bladder sparing approaches
- Neoadjuvant chemotherapy is the standard of care, regardless of local approach
- It remains to be seen in pathologic complete response rates among patients treated with immune checkpoint inhibitors translates to an OS benefit
- Many trials are ongoing and we must keep recruiting to these important clinical trials
Dr. Shilpa Gupta then presented a case of muscle-invasive bladder cancer for discussion. The patient was a 75-year-old male with a history of hypertension, coronary artery disease, who presented with gross hematuria. A TURBT revealed muscle-invasive bladder urothelial carcinoma. His ECOG performance status was 1 and his creatinine clearance was 65 ml/min. He had mild hearing loss and his desire was to pursue bladder sparing options if possible. CT scan showed focal thinking of the bladder but not metastatic disease and no lymphadenopathy. Dr. Gupta asked the panel what the preferred treatment would be for this patient:
- Trimodal bladder preservation?
- Neoadjuvant chemotherapy followed by radical cystectomy?
- Neoadjuvant chemotherapy followed by trimodal bladder preservation?
- Radical cystectomy alone?
- Neoadjuvant immunotherapy followed by radical cystectomy?
- Radical cystectomy followed by adjuvant immunotherapy?
Dr. Black notes that his go-to is neoadjuvant chemotherapy followed by radical cystectomy, whereas Dr. Sridhar would offer neoadjuvant chemotherapy followed by a multidisciplinary discussion as to subsequent radical cystectomy versus trimodal therapy. Dr. Gupta had an extensive discussion of various options with the patient and he was ultimately enrolled in the A031701 trial with an option for bladder-sparing in select patients. This is a phase II study of dose-dense gemcitabine plus cisplatin in patients with muscle-invasive bladder cancer with bladder preservation for those patients whose tumors harbor deleterious DNA damage response (DDR) gene alterations. Ultimately, this patient was not DDR positive, and he ended up receiving four cycles of dose-dense gemcitabine-cisplatin, which was well tolerated. He was then offered radical cystectomy but wanted to further explore bladder sparing options. An MRI showed mild bladder wall thickening along the left lateral and posterior margins of bladder, decreased from baseline. A repeat TURBT showed focal CIS and muscularis propria present and free of tumor. Dr. Gupta then asked the panel, what would be the next step in management:
- Offer concurrent chemoradiation?
- Offer radiation alone?
Dr. Sridhar would offer concurrent chemoradiation with several options available for sensitizing chemotherapy. Dr. Black notes that this is a reasonable approach but suggests that in the setting of CIS, one has to be careful regarding resistance to chemoradiation (but probably is ok in this patient given there is only focal CIS).
The patient underwent concurrent chemoradiation, which was given as 6480 cGy in 36 fractions with weekly cisplatin (35 mg/m2), which was well tolerated. He then underwent a TURBT, which showed left lateral wall resection with fibrosis and substantial necrotic tissue, with no tumor identified. Restaging CT scan showed treatment changes, with no recurrent disease.
The second case discussed by Dr. Gupta was that of a 72-year-old man with hypertension that presented with gross hematuria who subsequently underwent a TURBT showing muscle-invasive urothelial cancer. He had an ECOG performance status of 1, a creatinine clearance of 50 ml/min and severe hearing loss. He was deemed a surgical candidate and did not want to risk permanent hearing loss. Dr. Gupta then posed the following options to the panel:
- Trimodality bladder preservation?
- Gemcitabine-carboplatin followed by radical cystectomy?
- Radical cystectomy alone?
- Neoadjuvant immunotherapy followed by radical cystectomy?
- Radical cystectomy followed by adjuvant immunotherapy?
Dr. Sridhar notes that it is important to discuss all of these options with the patient. She typically does not favor gemcitabine-carboplatin and would rather favor cystectomy or clinical trial. This patient was ultimately enrolled on a perioperative immunotherapy trial KEYNOTE-905/EV-303, which is a randomized phase 3 study evaluating cystectomy with perioperative pembrolizumab versus cystectomy plus perioperative enfortumab vedotin and pembrolizumab versus cystectomy alone in cisplatin-ineligible patients with muscle-invasive bladder cancer. The trial design for this study is as follows: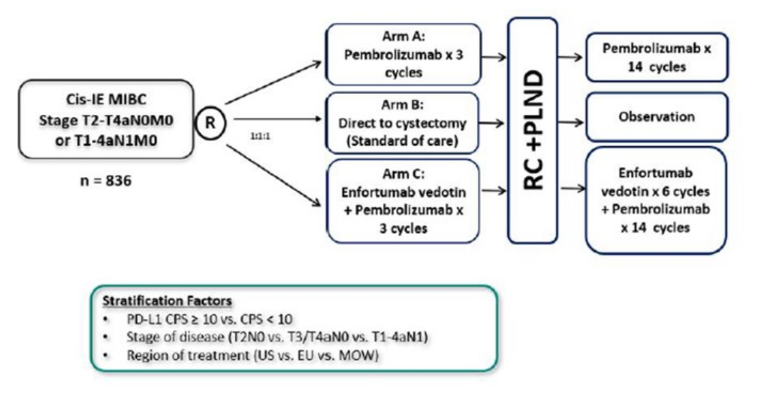
The patient was randomized to three cycles of neoadjuvant pembrolizumab and underwent radical cystectomy plus pelvic lymphadenectomy within 6 weeks of his last treatment, with no surgical complications. Post-operatively he developed elevated AST and ALT, with normal bilirubin and this was attributed to pembrolizumab. He was treated with an oral steroid taper and his LFTs returned to normal within 4 weeks. He was subsequently able to receive further cycles of pembrolizumab when the steroid taper was down to 10 mg per day and no further complications occurred. Dr. Gupta notes that it is crucial for all clinicians to give immune checkpoint inhibitors to understand the management of immune-related adverse events. As follows is a table regarding how to manage these adverse events based on adverse event grade:
Given that more urologists are using immune checkpoint inhibitors, Dr. Gupta made the following points for managing immune-related adverse events for the treating urologist:
- A team base approach is key to safely administering immunotherapy agents
- The adverse event profile and management can be simplified via structured monitoring and treatment protocols
- Patients should be regularly monitored for treatment-related complications
- Patient education and involvement is important to identify immune-related adverse events promptly
References:
1. Dinney CPN, Greenberg RE, Steinberg GD. Intravesical valrubicin in patients with bladder carcinoma in situ and contraindication to or failure after bacillus Calmette-Guerin. Urol Oncol 2013 Nov;31(8):1635-1642.
2. Skinner EC, Goldman B, Sakr WA, et al. SWOG S0353: Phase II trial of intravesical gemcitabine in patients with nonmuscle invasive bladder cancer and recurrence after 2 prior courses of intravesical bacillus Calmette-Guerin. J Urol 2013 Oct;190(4):1200-1204.
3. Steinberg RL, Thomas LJ, Brooks N, et al. Multi-Institution Evaluation of Sequential Gemcitabine and Docetaxel as Rescue Therapy for Nonmuscle Invasive Bladder Cancer. J Urol. 2020 May;203(5):902-909.
4. Black PC, Tangen C, Singh P, et al. Phase II trial of atezolizumab in BCG-unresponsive non-muscle invasive bladder cancer: SWOG S1605. J Clin Oncol 38, no. 15_suppl (May 20, 2020) 5022-5022.
5. Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab for the treatment of patients with BCG unresponsive, high-risk non-muscle-invasive bladder cancer (NMIBC): Over two years follow-up of KEYNOTE-057. J Clin Oncol 38, no. 15_suppl (May 20, 2020) 5041-5041.
6. Lee S, Lim B, You D, et al. Association of Bacillus Calmette-Guerin shortages with bladder cancer recurrence: A single-center retrospective study. Urol Oncol 2020 Aug 12;S1078-1439(20)30338-0.
7. Grimm MO, van der Heijden AG, Colombel M, et al. Treatment of high-grade non-muscle-invasive-bladder carcinoma by standard number and dose of BCG instillations versus reduced number and standard dose of BCG instillations: Results of the European Association of Urology Research Foundation Randomized Phase III Clinical Trial “NIMBUS”. Eur Urol 2020 May 20:S0302-2838(20)30334-1.
8. Kulkarni GS, Hermanns T, Wei Y, et al. Propensity score analysis of radical cystectomy versus bladder-sparing trimodal therapy in the setting of a multidisciplinary bladder cancer clinic. J Clin Oncol 2017;35(20):2299-2305.
9. Powles T, Rodriguez-Vida A, Duran I, et al. A phase II study investigating the safety and efficacy of neoadjuvant atezolizumab in muscle invasive bladder cancer (ABACUS). ASCO 2018 abstr 4506.
10. Necchi A, Raggi D, Gallina A, et al. Updated Results of PURE-01 with Preliminary Activity of Neoadjuvant Pembrolizumab in Patients with Muscle-invasive Bladder Carcinoma with Variant Histologies. Eur Urol 2020 Apr;77(4):439-446.
Chair: Peter Black, MD, B.Sc., University of British Columbia, Vancouver, Canada
Faculty:
Jurgen E. Gschwend, Rechts der Isar Medical Center, Munich, Germany
Shilpa Gupta, Cleveland Clinic Foundation, Cleveland, OH
Srikala Sridhar, Princess Margaret Cancer Centre, Toronto, Canada
Tilman Todenhofer, University Hospital Tubingen, Tubingen, Germany
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Twitter: @zklaassen_md at the 2020 Société Internationale d'Urologie Virtual Congress (#SIU2020), October 10th - October 11th, 2020