Dr. Porta began by highlighting that, based on data from CheckMate 214, JAVELIN Renal 101, and KEYNOTE-426, immunotherapy based combination treatments should be considered the standard of care for the first-line treatment of patients with metastatic renal cell carcinoma. However, he emphasized his belief that we should avoid making direct comparisons between studies as a result of differences in agents used, study endpoints, primary efficacy patients’ population, and distribution of patients across risk categories (prognostic groups).
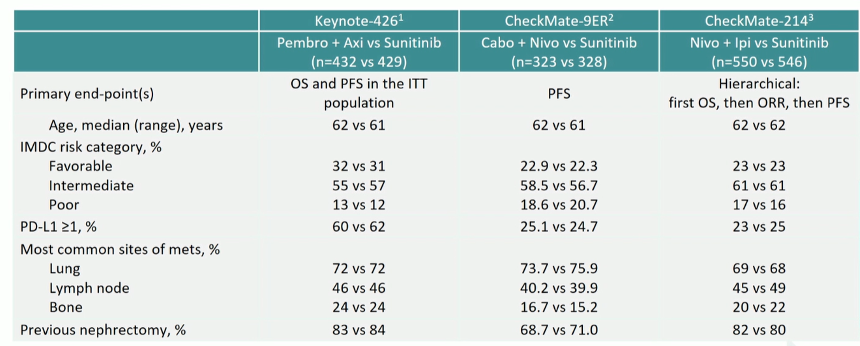
Notably, as highlighted in this table, the proportion of patients with PD-L1 expression >1% differs substantially between these trials. Further, the distribution among IMDC risk categories is somewhat different with KEYNOTE-426 having a lower representation of patients with poor risk criteria. Additionally, CheckMate 9ER had a lower proportion of patients with a history of prior nephrectomy.
Thus, perhaps not surprisingly, there are differences in results between these trials.
Dr. Porta then emphasized the question of “tails”, where these represent the right end of a survival curve with patients experiencing prolonged survival. In melanoma, the first trial of immunotherapy demonstrated a prolonged survival in approximately 20% of patients. Additionally, there was no separation of the curves early during follow-up.

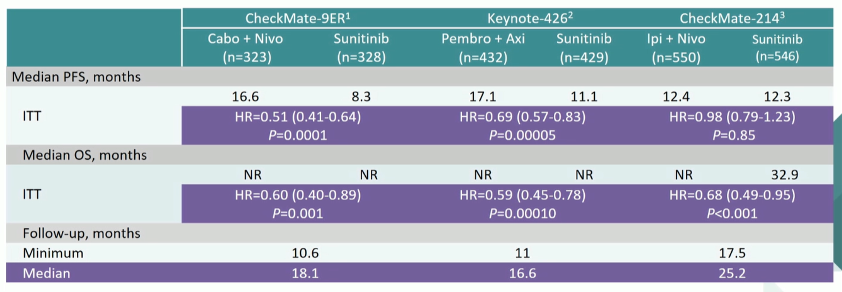
Dr. Porta then highlighted there are differences in follow-up between these trials. However, with prolonged follow-up of CheckMate214 suggests a not insignificant proportion of patients in this tail. Follow-up of the other trials is likely too short thus far to accurately assess this.
In contrast, we can look at the first few months of follow-up. In patients in the CheckMate214 trial receiving two immunotherapy based approaches, separation did not start to occur until at least 6 months while this occurred much early in KEYNOTE-426 and CheckMate-9ER which combined immunotherapy with targeted therapy. Thus, an earlier survival benefit is likely to be achieved by this combination approach.

An alternative way to decide may be to consider the proportion of patients who achieve a complete disease response. Rates of complete response are highest in the CheckMate214 trial (at 9% by first report and 11% at an update), though rates of progressive disease were also highest in this trial.

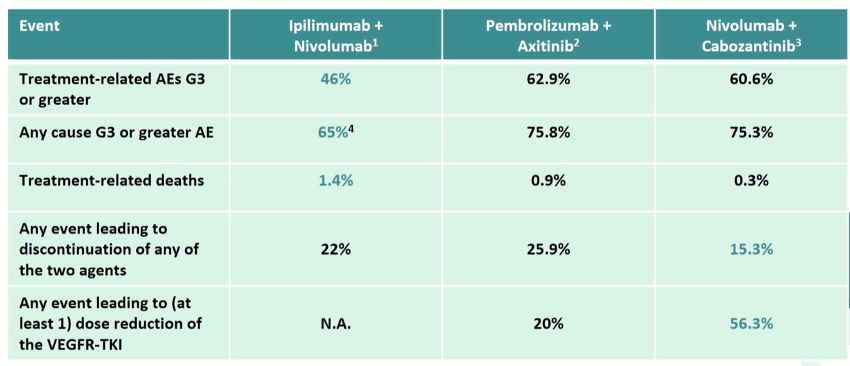
In addition to efficacy endpoints, safety must be considered when deciding between these treatment approaches. As highlighted in the following table, serious treatment-related adverse events and treatment-related deaths were reported in the experimental arm of CheckMate214 somewhat less commonly than in KEYNOTE-426 or CheckMate-9ER while treatment discontinuation and dose reduction due to adverse events were less common in CheckMate-9ER. Notably, in the CheckMate214 trial, the majority of safety issues occur during the early ipi induction phase. In contrast, safety issues continue over time in the other two combination approaches. Finally, these data may be somewhat confounded through the use of full dose axitinib in KEYNOTE-426 and reduced dose cabozantinib in CheckMate-9ER.
Further, quality of life (as measured with FKSI) is an important endpoint. Comparisons are difficult due differences in quality of life effects in the control arm between these trials. However, the combination of nivolumab and ipilimumab appear to have an increasing and long-lasting improvement in quality of life while the combination of nivolumab and cabozantinib is association with quality of life preservation and the combination of pembrolizumab and axitinib does not significantly affect quality of life, compared to sunitinib.
Dr. Porta then offered thoughts on how to make practice treatment decisions, highlighting his perspective that that only driver of our therapeutic decisions should be the biological aggressiveness of the tumor: in patients very aggressive disease, the combination of immune checkpoint inhibitor with VEGFR-TKI seems logical given the ability to have early disease control (from TKI) while awaiting long-term benefits of immunotherapy. In contrast, among those with less aggressive disease, a dual immunotherapy approach to maximize complete response rates and the potential for long-term disease-free survival would be reasonable, given also the ability to avoid long-term toxicity associated with ongoing TKI exposure. We should also consider trade offs between efficacy and safety, with many patients preferring efficacy in an unbalanced ratio.
In closing, he highlighted a number of open questions including:
- Could we use TKIs for only a limited period of time for induction at the beginning of combination therapy? This could spare chronic toxicities associated with these agents.
- What about reinduction of ipilimumab for patients who begin with dual immunotherapy in the case of disease progression?
- If TKIs modulate the tumor microenvironment in a beneficial manner, might it be reasonable to explore different treatment schedules?
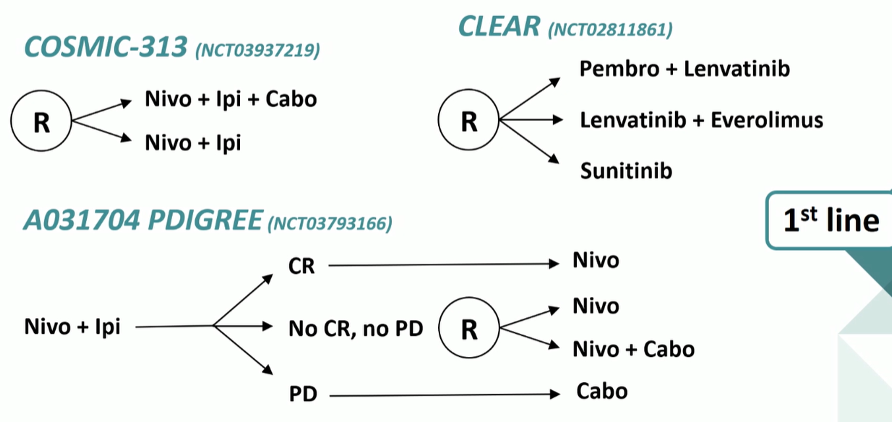
He highlighted the ongoing CLEAR study (NCT02811861) which will assess the combination of pembrolizumab plus lenvatinib and of everolimus plus lenvantinib as compared to sunitinib. However, potentially more informative will be the COSMIC-313 trial (NCT03937219) which is comparing nivolumab and ipilimumab with or without cabozantinib. Even more complex is the A031704 PDIGREE trial which utilizes initial nivolumab and ipilimumab with subsequent therapy determined by initial response. Those with partial responses and stable disease will then undergoing randomization.
Presented by: Camillo Guglielmo Porta, Professor, Department of Internal Medicine and Therapeutics, University of Pavia
Written by: Christopher J.D. Wallis, Urologic Oncology Fellow, Vanderbilt University Medical Center, Contact: @WallisCJD on Twitter at the European Society for Medical Oncology Virtual Congress, ESMO Virtual Congress 2020 #ESMO20, 18 Sept - 21 Sept 2020
Related Content:ESMO Virtual Congress 2020: Nivolumab + Cabozantinib vs Sunitinib in First-line Treatment for Advanced Renal Cell Carcinoma: First Results From The Randomized Phase 3 CheckMate 9ER Trial
ESMO 2020: CheckMate-9ER Study of Nivolumab Combined With Cabozantinib Vs. Sunitinib in Participants With Previously Untreated mRCC - Toni Choueiri