(UroToday.com) Following two abstract presentations in the poster discussion session focused on Prostate, Testicular, and Penile at the 2022 American Society of Clinical Oncology Annual Meeting held in Chicago and virtually, Dr. Kelvin A. Moses provided a discussion of equitable care in prostate cancer.
To begin, and give context to his presentation, Dr. Moses defined health disparities which, according to the Health Resources and Services Administration, are “population-specific differences in the presence of disease, health outcomes, or access to health care”. Race-based disparities in prostate cancer have been well documented for a number of decades now. Dr. Moses emphasized that Black men have 2.4x the risk of death from prostate cancer as White men. Further, Black men are diagnosed with more aggressive, higher grade and higher stage disease and develop cancer at a younger age, on average, than White men. Despite this, Black men are less likely to receive prostate cancer staging and, when diagnosed, are more likely to receive radiotherapy or no treatment as compared to surgery.
Given these observations, it is therefore not surprising to realize that Black men experience disparities in all aspects of the prostate cancer continuum, beginning with screening through treatment and treatment outcomes, to clinical trial participation, and mortality. This is, at least in part, driven by a lack of diversity in the physician workforce, in funding agency leadership and study sections, and the drivers of clinical trials who have for many years de-prioritized this public health crisis. In a poignant and well delivered moment, Dr. Moses emphasized that descriptive analyses, which may be productive for individual career advancement, are no longer sufficient in this high-risk population experiencing demonstrably poorer outcomes.
While much of the focus on disparities in prostate cancer care and outcomes has focused on Black men, Dr. Moses provided a somewhat broader view of cancer disparities in society. He noted first that there is an increasingly apparent disparities in outcomes for prostate cancer and other malignancies among Hispanic populations. As the Hispanic population in the United States continues to grow and ages, this will become an increasingly large public health problem. He further noted that Native American and Alaska Native populations have a greater mortality-to-incidence ratio than other racial and ethnic groups for nearly every cancer. This is most pronounced in screen-detected cancer such as prostate, cervical, breast, and colorectal cancers suggesting that health care access and delivery contribute to these disparities. Finally, he noted that health outcomes for LGBTQ individuals are systematically undervalued in our society. These individuals experience disparate rates of breast cancers and HPV related infections and malignancies. This may be mediated by a fear of coming out to their physician (particularly to religiously affiliated physicians or in religiously affiliated facilities) or a pressure to conform to gendered expectations. Additionally, he noted that there is a systemic disregard for fertility concerns in this population and that many LGBTQ individuals experienced legalized discrimination.
Given this context, he noted the two abstracts assessing the value of genetic testing and effective communication for prostate cancer care in Black men.
First, he discussed work presented by Dr. Hwang from the PROMISE group. He specifically noted that this dataset includes a representative proportion of Black men (~20%) which is relatively uncommon in clinical trials or prospective prostate cancer studies. Black men have, historically, been dramatically under-represented in genomic profiling studies in advanced prostate cancer.
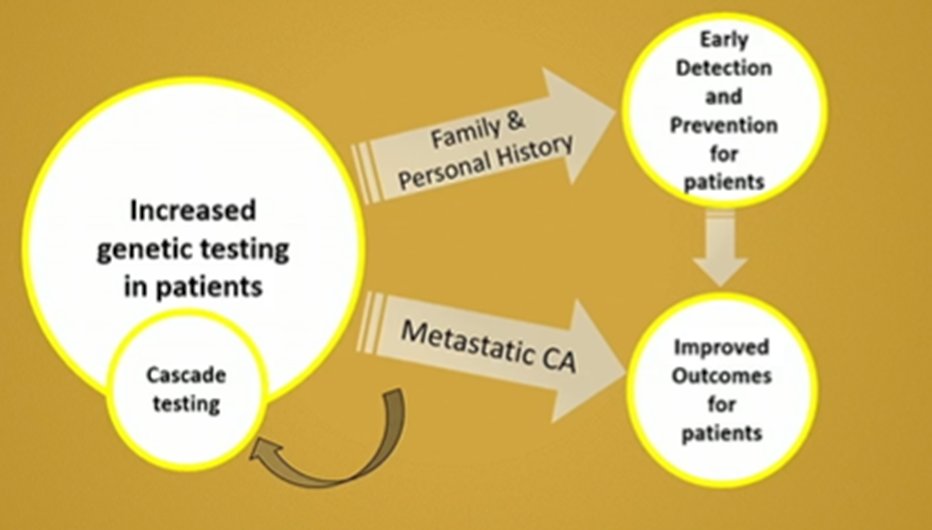
Dr. Moses noted that there are many potential advantages for the introduction of germline genetic testing including the opportunity for novel therapeutic approaches and improved clinical outcomes, for cascade family testing with early diagnosis and treatment also leading to improved clinical outcomes. Thus, the NCCN recommends genomic testing among men diagnosed with high or very-high risk localized and advanced prostate cancers.
In this work from Dr. Hwang, Dr. Moses noted that Black and White men had approximately equal rates of actionable genomic alterations with approximately one-third of men in each racial group having these findings. However, the specific alterations differed: MMR deficiency and MSI-high were more common in Black men while they have a lower frequency of PTEN alterations.
However, harkening back to his initial comments regarding disparities in access to care, Black men in this study were less likely to receive biomarker-directed therapy, a treatment pattern than flies in the face of NCCN guideline recommendations.
He moved then to a discussion of Dr. Loeb’s presentation focused on the effect of presenter race and position (physician vs patient) on trust in health care communication. Dr. Moses emphasized that many if not most of our patients will have sought external sources of information on their care online either before or after consultation. Much of this information lacks diversity and may not be presented at an appropriate level of health literacy to allow for meaningful consumption.
He noted that these randomized data from Dr. Loeb demonstrated higher levels of trust among Black men when the information was presented by a Black presenter, while no difference was noted among White men. This is in keeping with prior work which has shown that overall Black patients have better outcomes, greater trust, and are more likely to be compliant with treatment plans when they are in an ethnically concordant dyad with their physician.
He further noted that this work demonstrated that, in both Black and White men, there was considerably less trust in information about clinical trials than there was in information about screening. Thus, there is a need to improve communication regarding trials in all men.
Moving forward, Dr. Moses posed a variety of thought-provoking comments about how we may take the next steps forward including how we may improve rates of biomarker-directed therapy in Black men, whether use of these approaches will translate to equivalent outcomes in Black and White men, how we may improve our communication strategies to better reach Black men regarding prostate cancer, and how we might overcome historical prejudices in treatment and trials environments to increase trust.
In the discussion that followed his presentation, Dr. Moses made the impassioned statement (met with a round of applause) that it is within our control as physicians to improve care for our patients, each time we step into the voting booth. He noted that, following the Affordable Care Act, states with Medicare Expansion noted improved screening rates, improved treatment rates, and decreased mortality. Thus a (political) solution is well within reach if only we choose to act upon it.
Presented by: Kelvin Moses MD, PhD, Associate Professor Department of Urology, Fellowship Director Urologic Oncology Fellowship, Division of Urologic Oncology, Vanderbilt University Medical Center