The OSTRICh trial enrolled patients with poor-prognosis mCRPC (defined as visceral metastases or < 12 months responsive to androgen deprivation or progression during or within 6 months after docetaxel completion) to an open-label, multicenter, phase IIb study (NCT03295565). Following enrollment, patients were randomized 1:1 between cabazitaxel (25 mg/m2 IV Q3W and prednisone) and androgen receptor-targeted agent (daily abiraterone 1000 mg and prednisone OR enzalutamide 160 mg). Life prolonging therapy between docetaxel and randomization was not allowed.
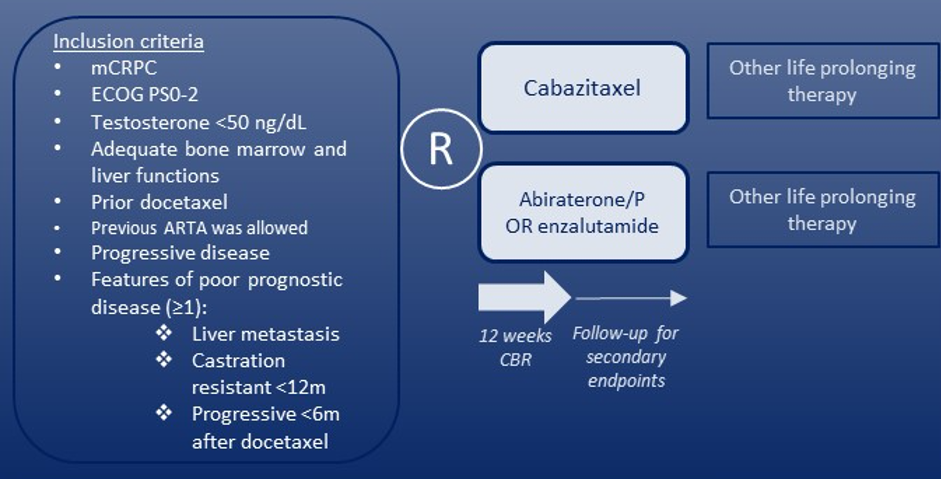
The authors defined their primary endpoint as the Clinical Benefit Rate (CBR) defined as no radiotherapy, no ECOG PS increase ≥2, no change of therapy, AND no radiological progression at 12 weeks in the study arms. A formal comparison of the CBR between treatment groups was a secondary endpoint. The Fisher Exact test was used to assess differences in CBR between groups and the log-rank test was used to assess differences in progression-free and overall survival. All-time to event endpoints were estimated with the Kaplan-Meier method and censored at last follow-up.
A total of 106 patients were randomized, with 53 patients allocated to each arm. At baseline, the median age was 70 (IQR 67-75) years and median PSA was 79.4 (IQR 29.0 - 160) ng/ml. The vast majority of patients had an ECOG PS score of 0 or 1 (n=99, 93%) while 7 (7%) had an ECOG PS of 2. All patients fulfilled the criteria for poor prognosis disease. Thirty-six (34%) patients had received docetaxel in the metastatic hormone-sensitive disease space while 41 (39%) previously received an androgen receptor-targeted agent.
Twenty-six of 43 evaluable patients in the cabazitaxel arm had clinical benefit at 12 weeks (CBR: 60%, 95% CI: 44%-75%) and 20 of 39 of patients in the androgen receptor targeted agent arm had clinical benefit at 12 weeks (CBR: 51%, 95% CI: 35%-68%), a difference which was non-significant (p = 0.50). At 12 weeks, 30 of 34 (88%, 95% CI: 73% - 97%) patients in the cabazitaxel arm and 24 of 36 (67%, 95% CI: 49% - 81%) patients in the androgen receptor targeted agent arm had no radiological progression, a difference which was statistically significant (p = 0.046).
After a median follow-up of 16.4 months (95% CI: 13.6–27.8), a serum PSA decrease ≥ 50% from baseline was observed in 12 patients (23%, 95% CI: 12% - 36%) treated with cabazitaxel and 26 patients (49%, 95% CI: 35% - 63%) treated with an androgen receptor targeted agent (p = 0.008). Median radiological progression free survival (rPFS) was 6.0 months (95%CI: 4.11-14.5) in the cabazitaxel arm and 5.8 months (95% CI: 5.22-10.2) months in the androgen receptor targeted agent arm (p = 0.5), while median overall survival was similarly not statistically significantly different between treatment groups: 15.3 months (95%CI 9.49-22.4) and 13.8 months (95%CI 11.7-16.4) in cabazitaxel and androgen receptor targeted agent treated patients, respectively (p = 0.8).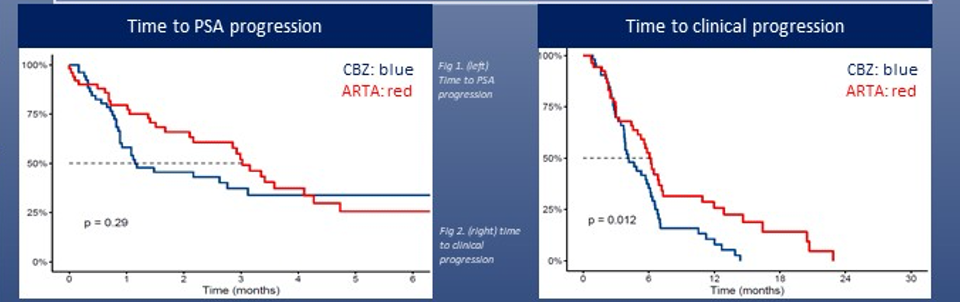
Grade ≥3 adverse events (AEs) were somewhat more common in patients treated with cabazitaxel (n=15, 29%) than those treated with androgen receptor-targeted agents (n=8, 15%).
The authors concluded that there was no significant difference between the clinical benefit of cabazitaxel and androgen receptor-targeted agents in this population of patients with poor-prognosis mCRPC though radiographic assessment favored patients treated with cabazitaxel and PSA-based metrics favored patients treated with androgen receptor-targeted agents.
Presented By: Kim van der Zande, Ph.D. Student, Netherlands Cancer Institute
Written By: Christopher J.D. Wallis, MD, Ph.D., Urologic Oncology Fellow, Vanderbilt University Medical Center, Twitter: @WallisCJD at the 2021 American Society of Clinical Oncology (ASCO) Annual Meeting #ASCO21, June, 4-8, 2021