As all three abstracts noted, 10-20% of patients with advanced disease are thought to harbor sarcomatoid histology and have a limited response to targeted therapies. They are almost predominantly found in stage IV tumors. As such, it has long been an independent predictor of poor survival. However, there has been some data to suggest improved outcomes with immune checkpoint inhibitors (ICIs).
To start with, Dr. Brugarolas compares the 3 studies, and also includes the Keynote-426 study presented by Dr. Brian Rini at ASCO 2019, as all relate to this topic:
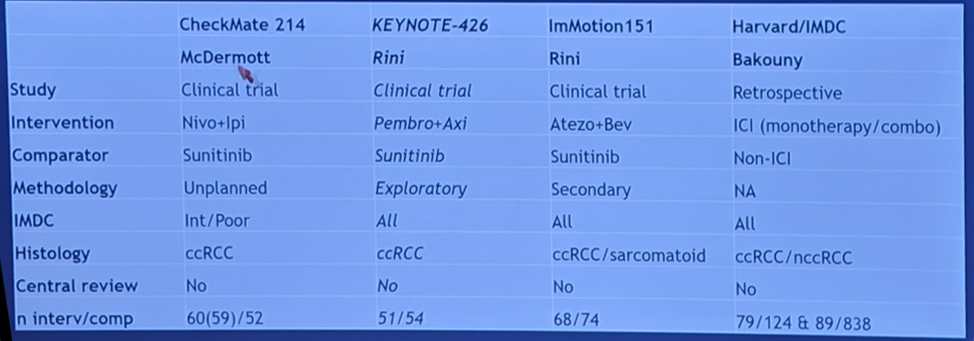
This specifically focused on patients with sarcomatoid histology (including rhabdoid in the Bakouny cohort). The McDermott abstract, from CheckMate-214, only included intermediate/poor risk patients. They all focused primarily on clear cell renal cell carcinoma (ccRCC), except for the Bakouny study. None of them had a central review.
On these next 2 slides, he compares the primary outcomes of the 3 trials and the retrospective study:
- Progression-free survival (PFS) in sarcomatoid RCC

At 12 months, all 3 are pretty similar, with 40-60% PFS. Much improved compared to TKI treated patients.
- Overall Survival in sarcomatoid RCC
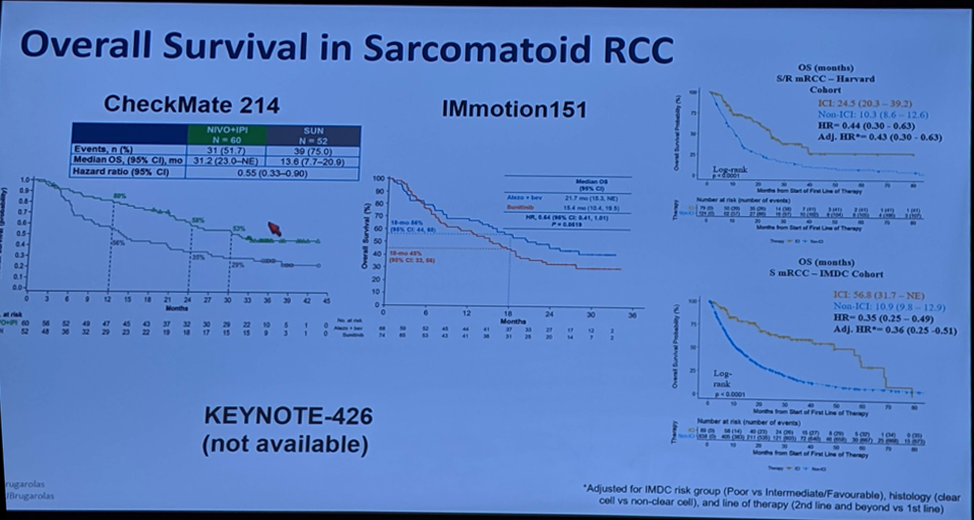
Again, much-improved overall survival (OS) compared to non-ICI treated patients. It was not statistically significant in the IMmotion-151 trial, however. The difference is particularly prominent in the retrospective review by Bakouny et al. (with inherent selection bias).
He did take a minute to look closer at the OS curve of the Checkmate-214 trial, stratified by sarcomatoid histology (and entire cohort) and by treatment.

While patients treated with nivo/ipi did better than those treated with sunitinib in all patients and those with sarcomatoid RCC, the difference was more pronounced in those with sarcomatoid histology. However, the nivo/ipi curves begin to separate at ~21 months – and with longer follow-up, perhaps the sarcomatoid RCC patients will do worse?
The clinical trials all focused on ccRCC. The retrospective study, however, did delve into the non-ccRCC patients with and without sarcomatoid differentiation. There was suggested benefit regardless of ccRCC or nccRCC. He also notes that in the Keynote-427 study (specifically for patients with nccRCC) assessing pembrolizumab in the first line for mRCC, there was a cohort of patients with sarcomatoid histology – and ORR was 45% for those patients (compared to 25% for the entire cohort). All of these suggest that sarcomatoid differentiated RCC (ccRCC or nccRCC) does well with ICI.
The efficacy results from the clinical trials are summarized below:

No new safety signals were identified in all the studies, different than the non-sarcomatoid patients.
All of these studies presented showed consistent and remarkable activity of ICI-containing regimens against RCC tumors with sarcomatoid differentiation. Greater efficacy was noted across all endpoints (ORR, PFS, and OS). Sarcomatoid tumors were also found to be characterized by an inflamed stroma (increased PD-L1 and T-eff signature), reduced angiogenesis, and mutations in TP32 – which may explain their poor response to TKIs, but improved response to ICIs.
Presented by: James Brugarolas, MD, PhD, Director of the Kidney Cancer Program, UT Southwestern Medical Center, Dallas, Texas, United States
Written by: Thenappan Chandrasekar, MD, Clinical Instructor, Thomas Jefferson University, @tchandra_uromd, @JEFFUrology at the 2019 ASCO Annual Meeting #ASCO19, May 31- June 4, 2019, Chicago, IL USA