Abstract 4515: Patient-reported outcomes (PROs) in IMmotion150: Atezolizumab (atezo) alone or with bevacizumab (bev) versus sunitinib (sun) in first-line metastatic renal cell carcinoma (mRCC)
In this study, the authors focused on the patient-reported outcomes from the IMmotion150 study of atezo with or without bevacizumab versus sunitinib as a first-line treatment for mRCC. I won’t rehash the primary findings of the study, but the main take-home point is the following: median time to deterioration (in most facets) was significantly longer with atezo monotherapy than atezo/bev or sunitinib alone. In comparison, in the Ipi/Nivo study for the same patient population, the same was true – risk of deterioration in PRO was significantly longer for ipi/nivo compared to sunitinib, albeit with different PRO tools.
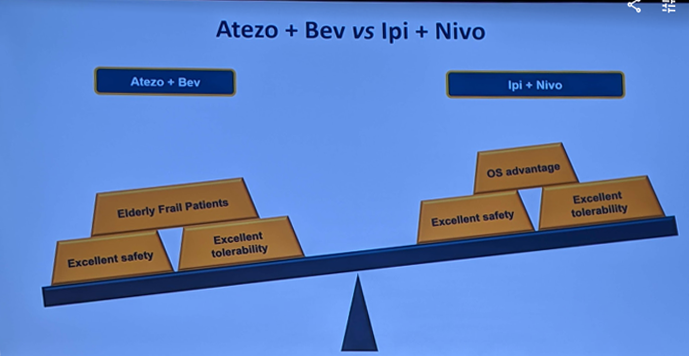
So, when you compare these 2 first-line agents, if you compare what we know, it would seem that due to better OS benefit, ipi/nivo may be favored, as he shows here:

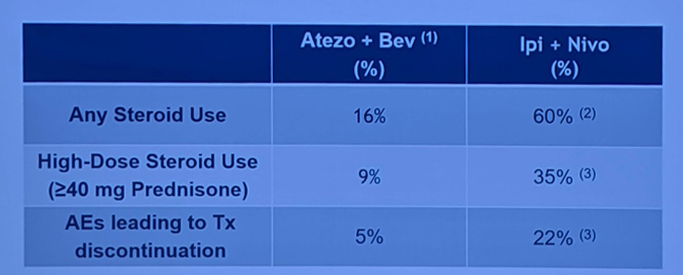
But, his caveat to this, is that if you compare toxicities, as seen below, atezo/bev has significantly less toxicity:
And, as many patients may be elderly or frail, atezo/bev may actually be better for them:
Abstract 4516: Active surveillance in metastatic renal cell carcinoma (mRCC): Results from the Canadian Kidney Cancer information system (CKCis)
In this study, Kushner et al. use the CKCis (Canadian Kidney Cancer information system) to look at active surveillance utilization and outcomes in a large, real-world cohort. It far exceeds the numbers of any other studies that looked at this previously. Harrison et al. looked at the MaRCC registry of 109 patients but had no follow-up – in that group, 45.9% chose AS up front (delayed therapy).1 Rini et al. have previously demonstrated that patients with mRCC put on AS can go a median of 14 months before needing systemic therapy, though their cohort was enriched with favorable and intermediate risk patients (25%, 75%, respectively).2 They also found that patients with IMDC 0-1 and 1-2 organ sites of metastases did best – 22 months median time to systemic therapy.
It should be noted that the study by Kushner et al. was retrospective and in no way randomized – which is demonstrated by the fact that AS patients were enriched for favorable risk disease (27% vs. 11%) and had a much higher rate of metastasectomy (22% vs. 5%), so they were also healthier. Interestingly, 122 patients out of 1833 didn’t get systemic therapy and died within 1 year – likely too sick/comorbid to get any treatment. Similar to the Rini paper, median time on AS was 14 months. 5-year OS was greater with AS – 70% vs. 32%. After adjusting for IMDC and age, OS and 1st line TTF were longer in the AS cohort.
This represents the largest cohort of AS in mRCC analyzed to date. Confirms that a subset of patients can be safely observed without immediate therapy. Looking at the balancing act for this question, if carefully selected, favors AS:

Abstract 4517: Safety and efficacy of nivolumab plus ipilimumab (NIVO+IPI) in patients with advanced renal cell carcinoma (aRCC) with brain metastases: Interim analysis of CheckMate 920
In this abstract by Emamekhoo et al., the authors assess the safety and efficacy of nivolumab plus ipilimumab (NIVO+IPI) in patients with advanced renal cell carcinoma (aRCC) with brain metastases, which is an interim analysis of one-arm (Cohort 3) of the Checkmate-920 study, seen below:

He noted that these patients had non-active brain metastases – so either previously radiated or <1 cm in size. He also noted that the dosing was unique – nivo 3 and ipi 1 is different than in order cohorts, where it is usually nivo 1 and ipi 3.
However, they found that the 6-month PFS rate was 62% and the 6-month OS was 89%, with an ORR of 29%. Prior experiences witk TKI’s such as sunitinib have not had as much success, often with ORR closer to 10-15%. This is demonstrated in his nice summary slide of the efficacy of currently approved therapy in brain metastases:
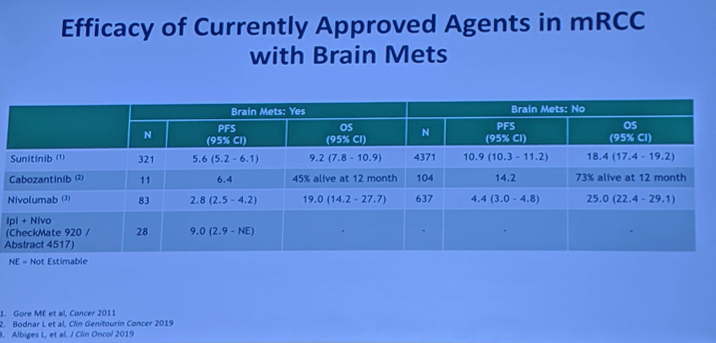
Ipi/Nivo appears to have a longer PFS, but further data is needed. So, the results are encouraging, but this is a small study with a relatively short follow-up. Additionally, these were not clinically relevant metastases (non-target lesions). Until the data is stronger, he still favors VEGF/TKI’s such as sunitinib and cabozantinib.

Presented by: Neeraj Agarwal, MD, Profesor of Medicine, Huntsman Cancer Institute, University of Utah, Salt Lake City, UT
Written by: Thenappan Chandrasekar, MD, Clinical Instructor, Thomas Jefferson University, @tchandra_uromd, @JEFFUrology at the 2019 ASCO Annual Meeting #ASCO19, May 31-June 4, 2019, Chicago, IL USA
References:
- Harrison et al. Front-line management patterns in the prospective metastatic renal cell cancer (MaRCC) registry. JCO 2016 Jan 10 34, no. 2_suppl 617-617
- Rini et al. Active Surveillance in metastatic renal-cell carcinoma: a prospective, phase 2 trial. Lancet Oncology 2016 Sep;17(9):1317-25.