- Abstract 4506: SWOG S1314: A randomized phase II study of co-expression extrapolation (COXEN) with neoadjuvant chemotherapy for localized, muscle-invasive bladder cancer
- Abstract 4507: Randomized trial of adjuvant chemotherapy versus adjuvant radiation therapy for locally advanced bladder cancer after radical cystectomy.
- Abstract 4508: Cytoreductive nephrectomy (CN) in metastatic renal cancer (mRCC): Update on CARMENA trial with focus on intermediate IMDC-risk population
Figure 1 – Balance of cancer care forces:

Figure 2 – Bladder cancer: “More is More” force:

In contrast, in kidney cancer, the “less is more” force is being utilized more commonly, where there is an integration of care across a smaller portion of the disease spectrum (Figure 3).
Figure 3 - Kidney cancer: “Less is More” force:

In bladder cancer, approximately 30% of patients receiving neoadjuvant chemotherapy reach the status of pathological stage T0 (2), and 12% of patients reach this status with transurethral resection alone.3 Could this be an untapped “Less is more” opportunity? However, it is noteworthy that clinical T0 is unreliable (4,5). When prospectively assessing these so-called clinical T0 patients using endoscopy evaluation at the time of radical cystectomy, it was found in the final radical cystectomy pathology that 58% of the so-called clinical T0 patients harbored carcinoma, and 29% of them harbored >=T2 disease.6 According to Dr. Kutikov, the COXEN gene expression, discussed in abstract 4506, is still a work in progress, and future studies might help elucidate its role in the utilization of neoadjuvant chemotherapy in bladder cancer.
Next, Dr. Kutikov discussed the implications of abstract 4507, comparing adjuvant chemotherapy to adjuvant radiation therapy for locally advanced bladder cancer, after radical cystectomy. In the results of this abstract it was shown that in patients with >=pT3b/T4, grade 3, or positive nodes, a recurrence rate of over 50% was shown within two years in both adjuvant radiotherapy- and adjuvant chemotherapy-treated patients. However, adjuvant radiotherapy appears to be a valid treatment option, especially if patients are too frail to receive systemic therapy.
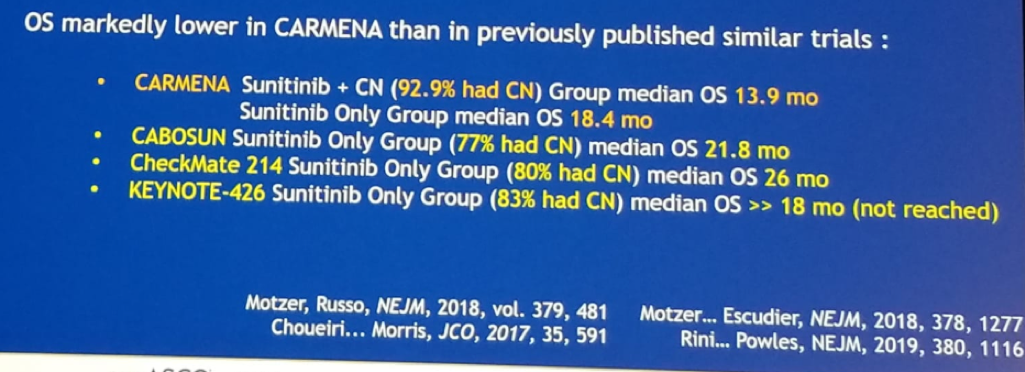
Lastly, Dr. Kutikov discussed the updated CARMENA results, presented in abstract 4508. The CARMENA trial teaches us that upfront cytoreductive nephrectomy can harm patients. However, attention should be paid to the data demonstrating that the overall survival was markedly lower in CARMENA patients than in similar previously published trials (Figure 4). This means that the patients in CARMENA harbor significantly worse disease than patients in other studies. In any case, the conclusion from this study states that upfront cytoreductive nephrectomy is no longer the standard of care, but some cohorts (such as those with one IMDC risk factor) may benefit from surgery. As a result of the CARMENA study, the recommendation of the updated European Urology guidelines,7 are:
- If the plan is to observe the patient without systemic therapy, it is possible to proceed to cytoreductive nephrectomy
- If it is not clear whether to observe the patient or not, then caution is advised with performing cytoreductive nephrectomy
- If the patient needs systemic therapy, it is imperative not to perform cytoreductive nephrectomy
Figure 4: Comparison of overall survival rate between CARMENA and other studies:
Presented by: Alexander Kutikov, MD, Chief of the Division of Urologic Oncology, Fox Chase Cancer Center, Philadelphia, PA
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow (SUO), University of Toronto, Princess Margaret Cancer Centre @GoldbergHanan at the 2019 ASCO Annual Meeting #ASCO19, May 31-June 4, 2019, Chicago, IL USA
References:
- Grossman et al. Neoadjuvant Chemotherapy plus Cystectomy Compared with Cystectomy Alone for Locally Advanced Bladder Cancer. NEJM 2003
- Lavery et al. Impact of stage and comorbidities on five-year survival after radical cystectomy in Poland: single centre experience. J Urol 2014, 191, 898
- Tollefson et al. World J Urol 2012
- deVere White et al. A sequential treatment approach to myoinvasive urothelial cancer: a phase II Southwest Oncology Group trial (S0219). J Urol 2009. 181, 2476
- Reese et al. The Utility of an Extensive Postchemotherapy Staging Evaluation in Patients Receiving Neoadjuvant Chemotherapy for Bladder Cancer. Urology, 2014, 84, 358
- Asghar et al. AUA 2019 Abstract PD66
- Bex et al. Updated European Association of Urology Guidelines for Cytoreductive Nephrectomy in Patients with Synchronous Metastatic Clear-cell Renal Cell Carcinoma. Eur Urol 2018, 74, 805