For context, Dr. Gillessen discussed the third-line mCRPC therapy CARD trial3. In CARD, patients who had previously received docetaxel and an androgen-signaling-targeted inhibitor (abiraterone or enzalutamide) were randomly assigned, in a 1:1 ratio, to either cabazitaxel or the other androgen-signaling-targeted inhibitor (either 1000 mg of abiraterone plus prednisone daily or 160 mg of enzalutamide daily). The primary endpoint was imaging-based progression-free survival, and a key secondary endpoint was survival:
Among 255 patients, over a median follow-up of 9.2 months, imaging-based progression or death was reported in 95 of 129 patients (73.6%) in the cabazitaxel group, as compared with 101 of 126 patients (80.2%) in the group that received an androgen-signaling-targeted inhibitor (HR 0.54, 95% CI 0.40 to 0.73). The median progression-free survival was 4.4 months with cabazitaxel and 2.7 months with an androgen-signaling-targeted inhibitor (HR for progression or death, 0.52; 95% CI, 0.40 to 0.68). The median overall survival was 13.6 months with cabazitaxel and 11.0 months with the androgen-signaling-targeted inhibitor (HR 0.64, 95% CI 0.46 to 0.89):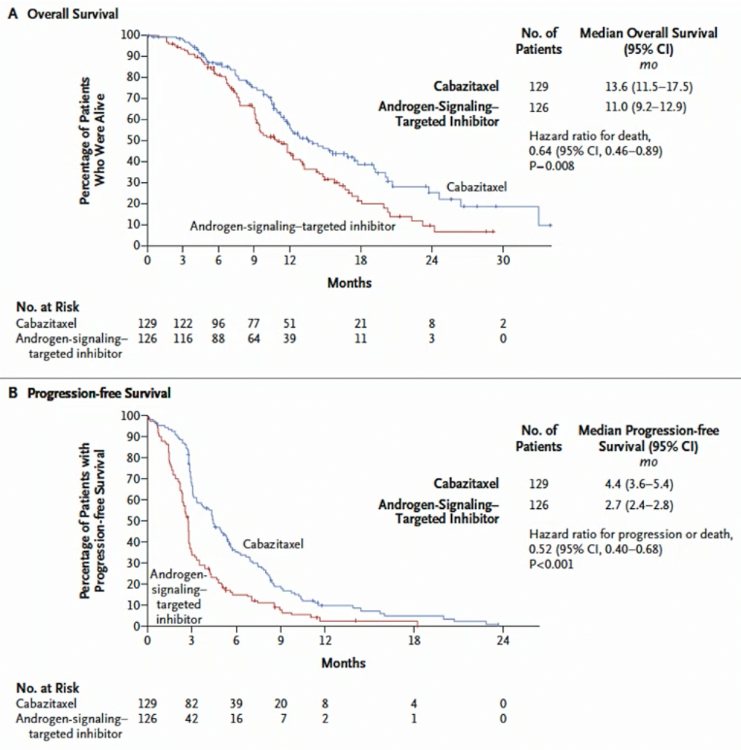
Dr. Silke Gillessen notes that TheraP was a phase 2 trial (n=200), while VISION was a phase 3 trial (n=831). Based on the aforementioned CARD trial, cabazitaxel was an appropriate control arm for the TheraP trial; in VISION, much has been made of the non-standardized protocol permitted standard of care, with no chemotherapy or radium-223 allowed, which resulted in many dropouts early in the study. Based on the PET selection criteria, this was more stringent for TheraP (concordant FDG-PET with PSMA-PET), resulting in 28% of patients being excluded from the study, compared to only 12% of patients being excluded in the VISION trial for PSMA negative metastases. TheraP had a primary endpoint of PSA response, whereas VISION had more robust primary endpoints of radiographic progression-free survival and overall survival. A summary of the comparison between the two trials provided by Dr. Gillessen is as follows: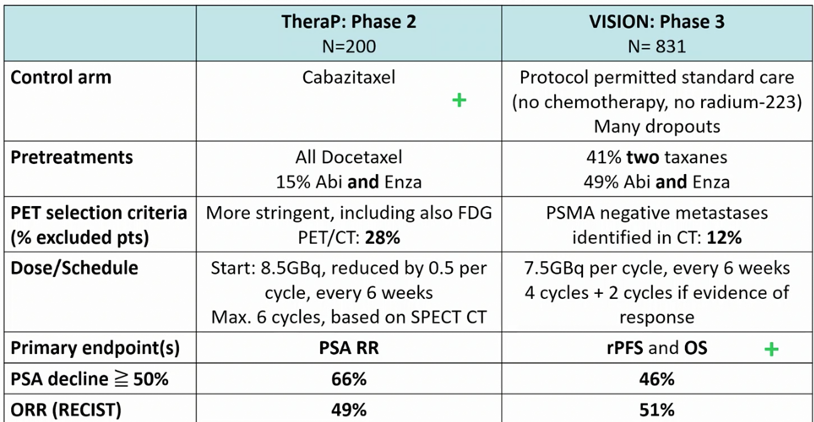
Dr. Gillessen notes that in the 177Lu-PSMA-617 arm of VISION 39.3% of patients had any grade dry mouth, in addition to 13% of patients receiving blood transfusions compared to 5% in the standard of care alone arm. By comparison, in TheraP 60% of patients receiving 177Lu-PSMA-617 had dry mouth, with an additional 30% of patients reporting dry eyes. She notes that xerostomia can be quite bothersome to the patient.
Dr. Gillessen emphasized that there are several points that we have learned from these two trials:
- 177Lu-PSMA-617 has meaningful activity in pretreated patients with mCRPC, but no clear plateau at the end of the survival curve
- Toxicity seems manageable, but longer-term toxicity has not been well evaluated over a median follow-up in VISION of 21 months. It will be important during follow-up to focus on renal function and secondary malignancies. At the 2021 ASCO annual meeting, long-term follow-up (68 months) after 177 Lutetium Octreotate for Neuroendocrine tumors showed a 6.7% incidence of myelodysplastic syndrome and leukemia
To put VISION into context for third-line therapy, Dr. Gillessen compared VISION to CARD and PROfound4-5, focusing on radiographic progression-free survival and overall survival, for which 177Lu-PSMA-617 (VISION) compares favorably to cabazitaxel (CARD) and olaparib (PROfound):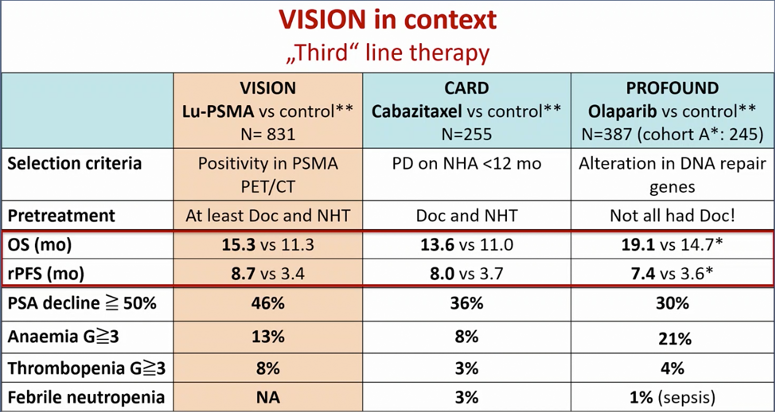
Dr. Gillessen notes that there are several open questions that remain answered:
- What is the optimal space of 177Lu-PSMA-617 in the current mCRPC treatment landscape? Fit patients should be offered docetaxel, and abiraterone or enzalutamide, and cabazitaxel at some stage. Additionally, a subgroup of patients can derive benefit from PARP inhibitors and a subgroup can derive benefit from pembrolizumab. It is likely that 177Lu-PSMA-617 should probably be used in many patients before cabazitaxel, but there may be patients who should receive cabazitaxel first: (i) patients with a super scan on scintigraphy and thus would have been excluded in VISION but not TheraP, and (ii) patients with liver metastases with low PSMA expression.
- How do we select patients? Do we need a 68Ga-PSMA PET/CT alone or in combination with an FDG PET/CT?
- What is the optimal dose and schedule of 177Lu-PSMA-617? Is a rechallenge possible or beneficial?
- How best do we monitor treatment with 177Lu-PSMA-617?
Dr. Gillessen concluded her presentation with the following summary points:
- 177Lu-PSMA-617 is a new therapy that prolongs OS
- When approved, it will add a treatment option for our patients with mCRPC
- Trials with other combinations or in non-chemotherapy-fit patients are planned
- Trials for patients in earlier stages in prostate cancer are also planned
- There are new radiopharmaceuticals on the horizon
Presented by: Silke Gillessen, MD, Professor and Head of the Medical Oncologist Department and Medical and Scientific Director at Inselspital, University Hospital, University of Bern, Bern, Switzerland, and Co-founder of the Advanced Prostate Cancer Consensus Conference (APCCC), previously of the University of Manchester and the NHS Christie Trust, Manchester, United Kingdom
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Association of Urology, EAU 2021- Virtual Meeting, July 8-12, 2021.
References:
- Hofman MS, Emmett L, Sandhu S, et al. [(177)Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): A randomized, open-label, phase 2 trial. Lancet. 2021 Feb 27;397(10276):797-804.
- Sartor O, de Bono J, Chi KN et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Jun 23 [Epub ahead of print].
- de Wit R, de Bono J, Sternberg CN, et al. Cabazitaxel versus Abiraterone or Enzalutamide in Metastatic Prostate Cancer. N Engl J Med 2019 Dec 26;381(26):2506-2518.
- de Bono J, Mateo J, Fizazi K, et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med 2020 May 28;382(22):2091-2102.
- Hussain M, Mateo J, Fizazi K, et al. Survival with Olaparib in Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2020 Dec 10;383(24):2345-2357.
EAU 2021: Phase 3 Study of 177Lu-PSMA-617 in Patients with Metastatic Castration-Resistant Prostate Cancer (VISION)
EAU 2021: TheraP Phase 2 Trial of Lu-PSMA-617 vs Cabazitaxel: Results and Contrasts to the VISION Study