The definition and implementation of specific QIs in the field of renal cell carcinoma (RCC) present distinct challenges.1,2 The main issues associated with contemporary diagnostic and treatment pathways for patients with RCC include the overdiagnosis of benign/indolent renal masses (with consequent overtreatment, despite stable mortality rates), rapid evolution of treatment patterns, increasing need for a multidisciplinary approach for both localized and metastatic disease,3 and unwarranted variation in RCC care across Institutions and nations. In this scenario, the development and integration of standardized and common QIs in RCC care remain an unmet need, with a lack of consensus across guidelines and international societies.3,4
In this review, we summarized the available QIs for RCC, focusing on their characterization throughout the care pathway and the potential areas for further development.
The PICOS framework for this review was the following:
- P: adults (age 18 years) with nonmetastatic or metastatic renal mass/RCC
- I: surgery (partial nephrectomy or radical nephrectomy), thermoablation, active surveillance, and systemic therapy
- C: either comparative or noncomparative studies
- O: QIs/quality metrics for renal cancer care
- S: prospective or retrospective studies
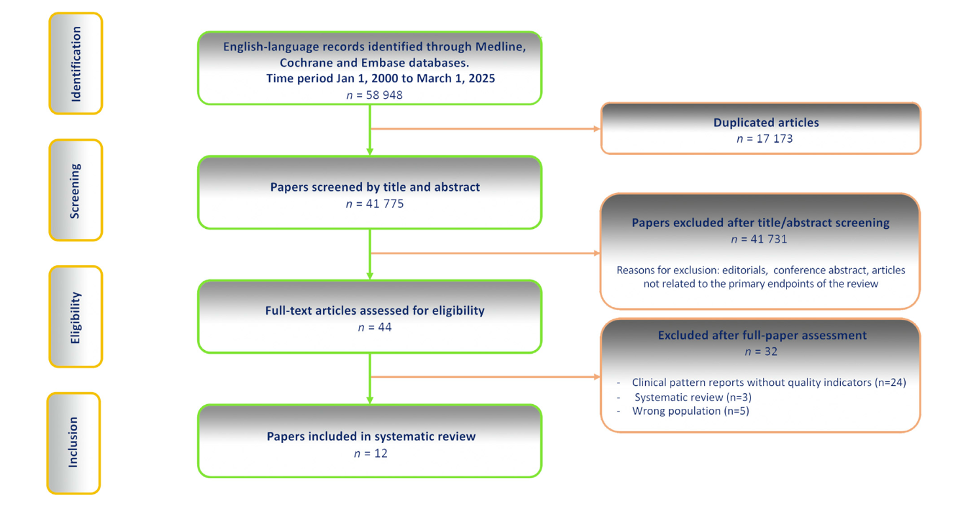
Fig. 1
A detailed overview of the methodological appraisal (according to the Appraisal of Indicators through Research and Evaluation (AIRE) items) is reported in Fig. 2. QI sets had a large variation in the development strategy and quality.

Fig. 2
Although ten (83%) of the 12 QI sets have been piloted in practice, none of these has been fully externally validated.
Overall, 95 QIs were identified from the 12 included studies (12 sets of QIs; Table 1). The number of proposed QIs varied significantly across studies, ranging from 1 to 25 QIs. Notably, only a few studies explicitly specified the target population.

The QIs addressed different stages of RCC care pathways, which are summarized graphically in Figs. 3 and 4 into three main categories: structure, process, and outcomes indicators.
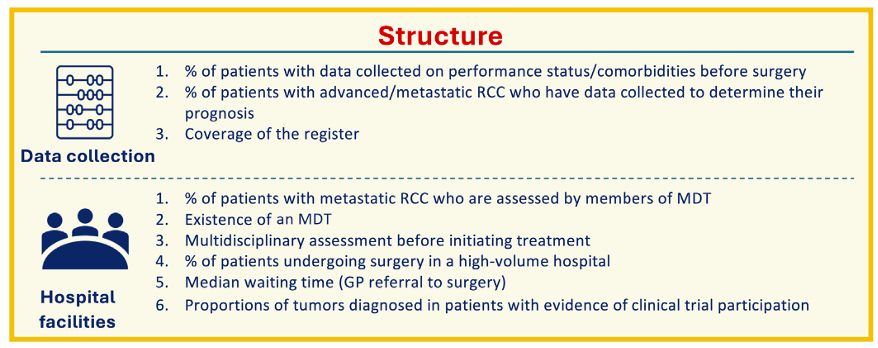
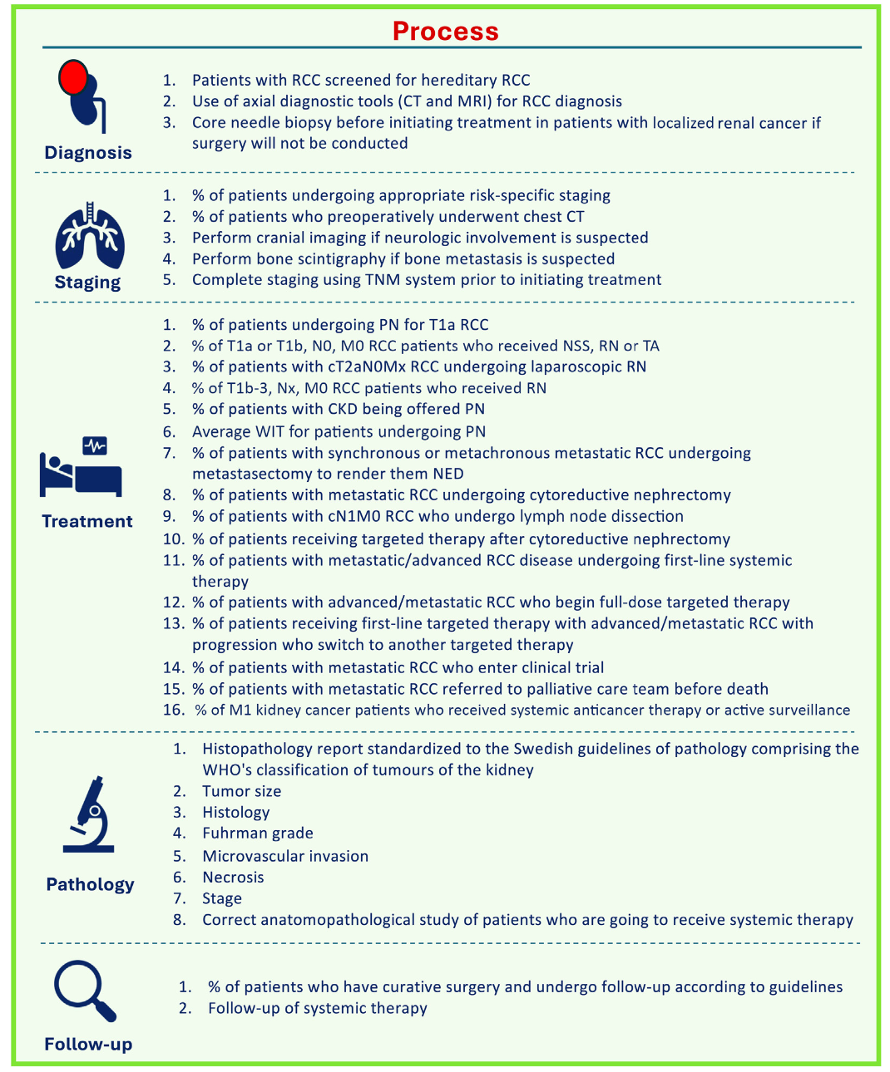
Fig. 3
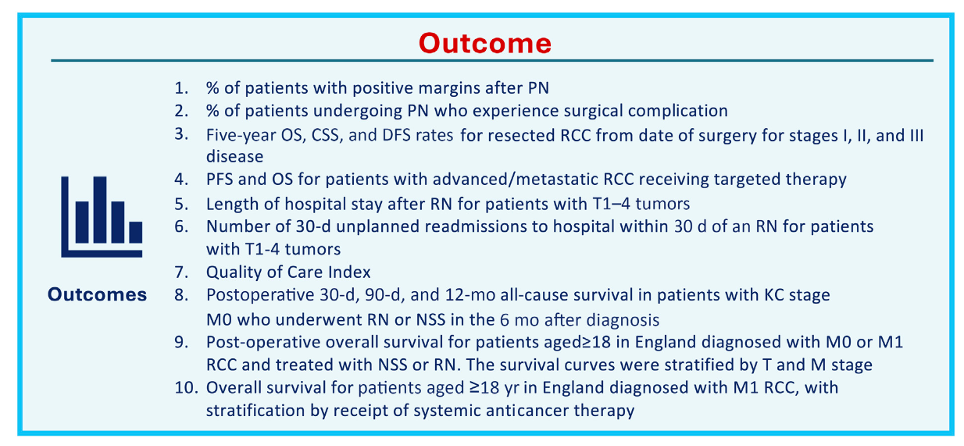
Fig. 4
After categorizing the QI sets into these eight domains, we found that diagnosis was addressed in 33% of the studies, staging and data collection in 25%, treatment in 67%, pathology in 42%, outcomes in 83%, hospital facilities in 25%, and follow-up in 17% of the studies (Fig. 5).
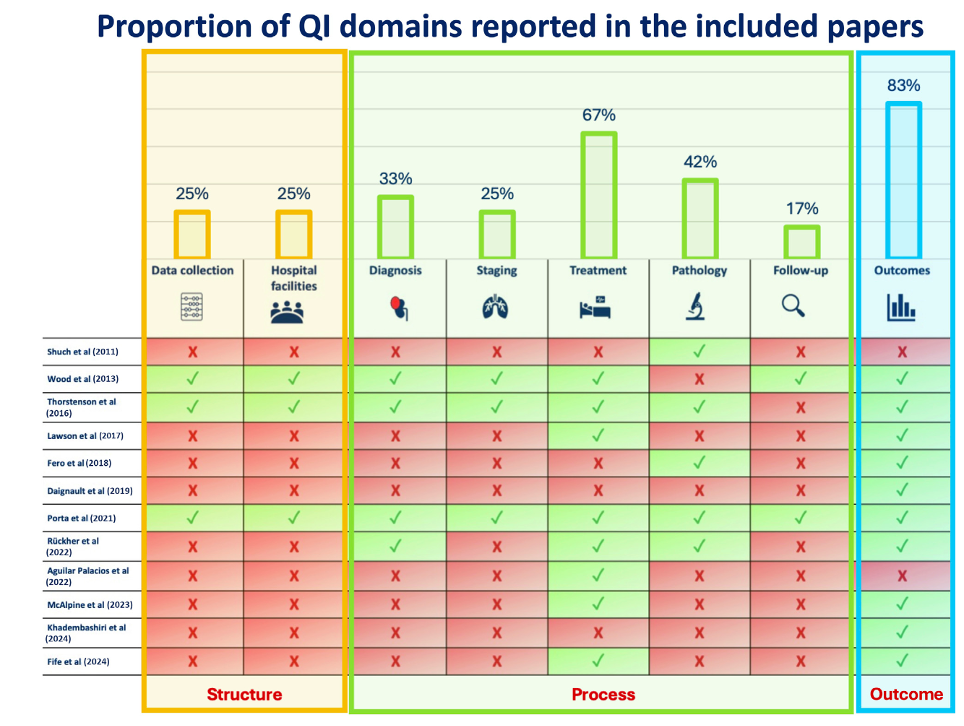
Fig. 5
Notably, regardless of the specific domain, most studies did not specifically report any cutoff value to evaluate whether the proposed QIs were fulfilled or not. In this regard, only three studies reported specific targets for the proposed QIs (Table 1), and none offered any methods of QI improvement.
To the best of our knowledge, this is the first systematic review assessing the available quality indicators (QIs) for renal cell carcinoma (RCC) care designed to provide clinicians, researchers, and policymakers a benchmark to improve the utility of contemporary diagnostic and therapeutic pathways.
Our review found that only a few studies have proposed QIs specifically tailored for RCC care and underscores the importance of a more structured approach to data collection at hospital, regional, and national levels to improve the comprehensiveness of QIs in renal cancer care. This study underscores the need for standardized, easy-to-collect QIs covering the entire RCC care pathway, emphasizing the potential for improving outcomes through a centralized, data-driven national approach. Our work offers leading international organizations a robust foundation for finding consensus on a shared, comprehensive set of QIs for RCC care, encompassing the entire care pathway, from diagnosis to long-term follow-up.
Written by: Riccardo Campi, MD, Ph.D, FEBU, Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy; Unit of Urology and Renal Transplantation, Oncology Department, Careggi University Hospital, Florence, Italy.
On behalf of all co-authors
- Alessio Pecoraro, Sara Costagli, Lorenzo Masieri, Sergio Serni, Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy; Unit of Urology and Renal Transplantation, Oncology Department, Careggi University Hospital, Florence, Italy
- Andrea Minervini, Department of Experimental and Clinical Medicine, University of Florence, Florence, Italy; Unit of Urology and Andrology, Oncology Department, Careggi University Hospital, Florence, Italy
- Laura Marandino, Skin and Renal Units, The Royal Marsden NHS Foundation Trust, London, UK;
- Raghav Varma, Clinical Effectiveness Unit, Royal College of Surgeons, London, UK; Faculty of Public Health and Policy, London School of Hygiene & Tropical Medicine, London, UK
- Maarten Albersen, Department of Urology, University Hospitals Leuven, Leuven, Belgium
- Umberto Capitanio, IRCCS San Raffaele Scientific Institute, Urological Research Institute, Milan, Italy; University Vita-Salute San Raffaele, Milan, Italy
- Michael Jewett, International Kidney Cancer Coalition and Clinician Investigator, Princess Margaret Cancer Centre and University Health Network, Department of Surgery (Urology), University of Toronto, Toronto, Ontario, Canada
- Alexander Kutikov, Division of Urologic Oncology, Department of Surgical Oncology, Fox Chase Cancer Center, Philadelphia, PA, USA
- Steven MacLennan, Academic Urology Unit, University of Aberdeen, Aberdeen, UK
- Grant D. Stewart, Department of Surgery, University of Cambridge, Cambridge Biomedical Campus, Cambridge, UK; CRUK Cambridge Centre, Cambridge Biomedical Campus, Cambridge, UK
- Patricia Zondervan, Department of Urology, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands; Cancer Center Amsterdam, Imaging and Biomarkers, Amsterdam, The Netherlands
- Axel Bex, Specialist Centre for Kidney Cancer, Royal Free Hospital, London, UK; Division of Surgery and Interventional Science, University College London, London, UK; The Netherlands Cancer Institute, Antoni van Leeuwenhoek Hospital, Amsterdam, The Netherlands
- Beyer K, Widdershoven C, Wintner LM, et al. A systematic review of heterogeneity in outcome definition and reporting in localised renal cancer. Eur Urol Open Sci 2023;48:1–11.
- Bukavina L, Bensalah K, Bray F, et al. Epidemiology of renal cell carcinoma: 2022 update. Eur Urol 2022;82:529–42.
- Bex A, Ghanem YA, Albiges L, et a. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2025 Update. Eur Urol. 2025 Jun;87(6):683-696. doi: 10.1016/j.eururo.2025.02.020. Epub 2025 Mar 20. PMID: 40118739.
- MacLennan S, Wintner LM, Beyer K, et al. A protocol for the development of core outcome sets for effectiveness trials and clinical audits in renal cell cancer (R-COS). BJUI Compass 2023;4:504–12.