In addition, the characterization of the risks involved has not been defined regarding the specific situation of the individual patient. This point is clinically relevant since the well documented heterogeneity of PCa may well translate into widely discrepant responses to testosterone therapy (TTh) among patients, as reported by us and others.
Nevertheless, long established principles have, justifiably been challenged but the emerging concepts are not mature enough to allow wide generalizations.
For instance, those successfully treated for PCa are in a category very different from those with low-risk disease on active surveillance. The former are candidates for testosterone therapy not much different than for men without a history of PCa, while the latter are also potential candidates for TTh but demand closer follow-up.
Much different is the situation for men suffering from disabling hypogonadism and harboring intermediate- and high-risk PCa. These require stricter criteria for considering TTh and must commit to regular and competent follow-up.
A more challenging cohort comprises those with recurrent PCa or at high risk of recurrence. These men, although potential candidates for TTh are not suitable for management by the occasional general urology practice and should be handled at a center with expertise in the field.
Considering the significance of the controversy and the fact that different professional associations provide inconsistent and sometimes conflicting guidelines we are offering a set of basic and practical proposals for urologists.
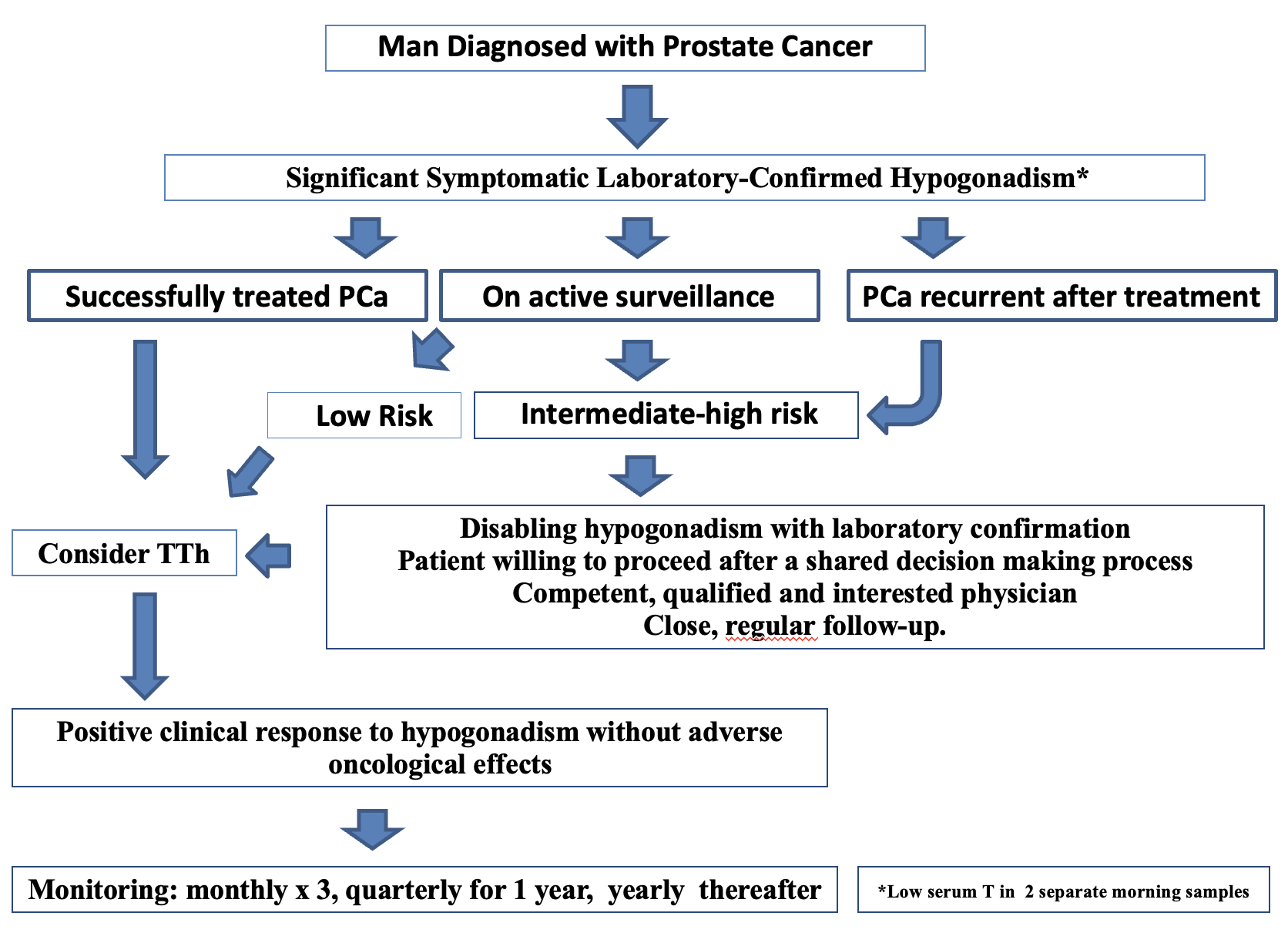
Criteria to consider before initiating TTh in a patient with TD and PCa
- An experienced, qualified, and interested physician
- A patient able and willing to provide informed consent
- An engaged patient committed to a shared-decision making process
- A clinical picture supporting the diagnosis of significant hypogonadism
- Serum T levels confirming the diagnosis of TD
- Absence of spinal metastases with risk of cord compression
- Absence of contraindications for TTh (e.g. erythrocytosis, congestive heart failure)
- Favor short acting T formulations in the early period of treatment
- A priori settlement of benchmarks for cessation of TTh (e.g. PSA velocity/increase ≥ 20% within first 3 months)
- Evaluation of functional response to TTh at 3 and 6 months. In the absence of response seek other causes and consider cessation of TTh
- Baseline hematology and biochemistry (serum T, hematocrit, hemoglobin, PSA)
- Imaging for documentation of loco-regional or metastatic disease depending on the specific oncological scenario
- Follow-up hematology and biochemistry monthly for initial 3 months and every 3-6 months thereafter, if stable
Read the Abstract