The majority of patients with non-metastatic muscle-invasive bladder cancer are treated with neoadjuvant chemotherapy followed by radical cystectomy and extended lymph node dissection.1 Still, up to 40% of the patients with more advanced disease stage develop a pelvic recurrence.2 These locoregional failures are rarely salvageable and associated with a poor survival.3 In the past, adjuvant external beam radiotherapy (ART) has shown to increase disease free survival, but excessive toxicity hampered enthusiasm for further implementation.4
More recently, an Egyptian and a Belgian phase II trial, both using modern radiotherapy techniques, suggested that ART is a safe and effective treatment for these patients.5,6 To guide the contouring of the clinical target volume (CTV), consensus delineation guidelines were published by Baumann et al. in 2016. These initial guidelines were based on the data of a single institution.7 Subsequently, several other pattern of failure analyses post-cystectomy were conducted, leading to the proposal of some optimizations.8,9 In the pattern of failure analysis by Reddy et al., 40% of the failures outside the CTV were observed in the region of the common iliac nodes and obturator nodes. Including the common iliac nodes up to the aorta bifurcation and extending the internal border of the obturator nodes to 19 mm medial of the obturator internus muscle would lead to the inclusion of all recurrence in both regions.8 Furthermore, in the pattern of failure analysis by Murthy et al. a high cystectomy bed recurrence rate was reported in spite of a low positive surgical margin rate.9
The current article reports the results of an expert panel of radiation-oncologists from the International Bladder Investigator Society that re-evaluated the CTV contouring guidelines in ART bladder cancer. This evaluation was done in 3 consecutive steps. First, the interobserver variability in CTV contouring in clinical practice was assessed. Secondly, a pattern of failure analysis of the Belgian ART trial was performed. Thirdly, the results of the interobserver variability and pattern of failure analysis were discussed in a panel discussion. The panel recommended several adaptations to the in 2016 published guidelines by Baumann et al. The updated consensus contouring guidelines are presented in Table 1. Key adaptations are to include the iliac nodes up to the level of the aorta bifurcation and to include the cystectomy bed in all patients (also in case of a negative surgical margin).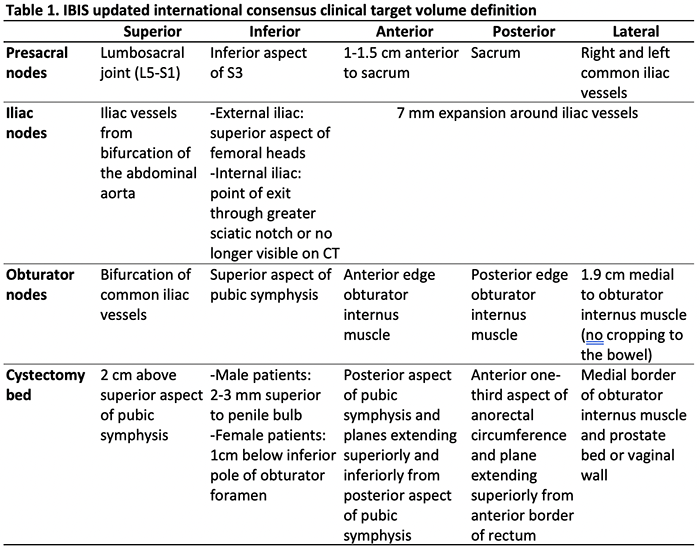
Currently, two randomised controlled phase III trials are being conducted (GETUG-AFU30 (NCT03333356) and BART trial (NCT02951325)) to further determine the place of ART in high risk muscle-invasive cancer patients.
Written by: Flor Verghote, MD1,2 & Valérie Fonteyne, MD, PhD1,2
- Department of Radiotherapy-Oncology, Ghent University Hospital, Ghent, Belgium.
- Department of Human Structure and Repair, Ghent University, Ghent, Belgium.
Funding: the analysed Belgian ART trial was funded by a grant of Kom op tegen Kanker (Stand up to Cancer), the Flemish cancer society. The funding body was further not involved in the design of the study and collection, management, analysis, and interpretation of data and in writing or submitting of the manuscript.
References:
- Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. The New England journal of medicine. Aug 28 2003;349(9):859-66. doi:10.1056/NEJMoa022148
- Baumann BC, Guzzo TJ, He J, et al. A novel risk stratification to predict local-regional failures in urothelial carcinoma of the bladder after radical cystectomy. Int J Radiat Oncol Biol Phys. Jan 1 2013;85(1):81-8. doi:10.1016/j.ijrobp.2012.03.007
- Zaghloul MS, Awwad HK, Akoush HH, et al. Postoperative radiotherapy of carcinoma in bilharzial bladder: improved disease free survival through improving local control. Int J Radiat Oncol Biol Phys. 1992;23(3):511-7. doi: 10.1016/0360-3016(92)90005-3.
- Reisinger SA, Mohiuddin M, Mulholland SG. Combined pre- and postoperative adjuvant radiation therapy for bladder cancer–a ten year experience. Int J Radiat Oncol Biol Phys. 1992;24(3):463-8. doi:10.1016/0360-3016(92)91060-z
- Zaghloul MS, Christodouleas JP, Smith A, et al. Adjuvant sandwich chemotherapy plus radiotherapy vs adjuvant chemotherapy alone for locally advanced bladder cancer after radical cystectomy a randomized phase 2 trial. Article. JAMA Surgery. 2018;153(1)doi:10.1001/jamasurg.2017.4591
- Fonteyne V, Dirix P, Van Praet C, et al. Adjuvant Radiotherapy After Radical Cystectomy for Patients with High-risk Muscle-invasive Bladder Cancer: Results of a Multicentric Phase II Trial. European Urology Focus. 2021/12/08/ 2021;doi:https://doi.org/10.1016/j.euf.2021.11.004
- Baumann BC, Bosch WR, Bahl A, et al. Development and Validation of Consensus Contouring Guidelines for Adjuvant Radiation Therapy for Bladder Cancer After Radical Cystectomy. Int J Radiat Oncol Biol Phys. Sep 1 2016;96(1):78-86. doi:10.1016/j.ijrobp.2016.04.032
- Reddy AV, Christodouleas JP, Wu T, Smith ND, Steinberg GD, Liauw SL. External Validation and Optimization of International Consensus Clinical Target Volumes for Adjuvant Radiation Therapy in Bladder Cancer. Int J Radiat Oncol Biol Phys. Mar 15 2017;97(4):740-746. doi:10.1016/j.ijrobp.2016.11.039
- Murthy V, Bakshi G, Manjali JJ, et al. Locoregional recurrence after cystectomy in muscle invasive bladder cancer: Implications for adjuvant radiotherapy. Urologic oncology. Feb 8 2021;doi:10.1016/j.urolonc.2021.01.015