Our findings describe what patients can expect if they elect for nephrostomy insertion. The creatinine will decrease in a highly predictable manner. However, prognosis remains poor and only 30% of our patients were able to have further oncological treatment. Thirty-eight percent remained nephrostomy dependent for the rest of their lives. The average patient following nephrostomy insertion for obstructing pelvic malignancy required two nephrostomy unit re-insertions. Thirty-nine percent had at least one further 30-day admission to the hospital.
This supports the findings of previous studies suggesting 14-26% of patients after nephrostomies developed urinary tract infection and up to 69% of patients spent 20% of their remaining life in the hospital due to nephrostomy or stent-related issues.3-5 With regards to urological malignancies, there was a trend towards prostate cancer patients faring better with nephrostomies than patients with bladder cancer, but we did not find a statistically significant difference.
The decision to insert a nephrostomy is multi-faceted, and often urologists will have to consider first, the prognosis of the malignancy which may not be urological; second, whether improving renal function will allow further treatments such as chemotherapy; and finally, the quality of life implications of nephrostomies. Our predictive model mentioned in the paper is shown below, and allows an estimation with high confidence of the improvement in renal function that is possible following nephrostomy insertion from different creatinine values pre-insertion:
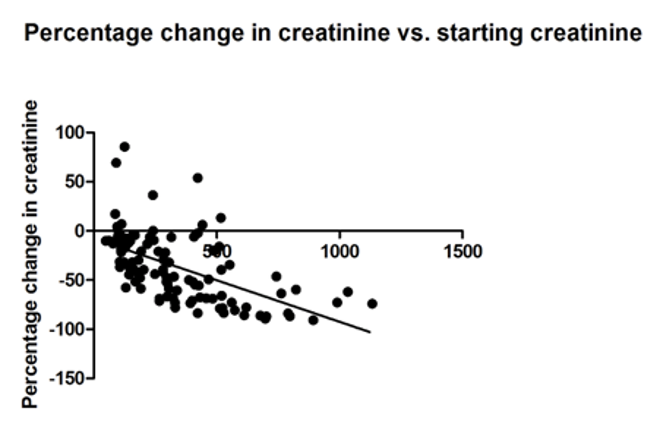
The correlation between creatinine change and starting creatinine was statistically significant (Pearson r -0.5717 p<0.0001)
We recommend the use of this model in a multi-disciplinary team setting including the ‘parent’ surgical and oncology specialty, to first determine what further treatments could be offered following nephrostomy insertion. Taking into account the prognosis of the malignancy and this prediction, the detailed data above can be used to inform our patients of the potential benefits and effects on quality of life of this intervention. We hope this study will help us to reach individually-tailored decisions with our patients as to whether inserting nephrostomies for obstructing pelvic malignancy is in their best interests.
Written by: Samuel S. Folkard, BMBCh, BA, MRCS, NHS England Clinical Entrepreneur Fellow, The Urology Foundation Warrior Programme KSS Deanery, London, England, Twitter: @FolkardSam
References:
- Prentice, Joanna, Tarik Amer, Ali Tasleem, and Omar Aboumarzouk. "Malignant ureteric obstruction decompression: how much gain for how much pain? A narrative review." Journal of the Royal Society of Medicine 111, no. 4 (2018): 125-135.
- Folkard, Samuel Stephen, Srijit Banerjee, Richard Menzies-Wilson, Joseph Reason, Evangelos Psallidas, Elliot Clissold, Ahmad Al-Mushatat, Saurabh Chaudhri, and James Stephen Arthur Green. "Percutaneous nephrostomy in obstructing pelvic malignancy does not facilitate further oncological treatment." International Urology and Nephrology (2020): 1-4.
- Cordeiro, Maurício D., Rafael F. Coelho, Daher C. Chade, Rodrigo R. Pessoa, Mateus S. Chaib, José R. Colombo‐Júnior, José Pontes‐Júnior, Giuliano B. Guglielmetti, and Miguel Srougi. "A prognostic model for survival after palliative urinary diversion for malignant ureteric obstruction: a prospective study of 208 patients." BJU international 117, no. 2 (2016): 266-271.
- Wilson, J. R., G. H. Urwin, and M. J. Stower. "The role of percutaneous nephrostomy in malignant ureteric obstruction." Annals of the Royal College of Surgeons of England 87, no. 1 (2005): 21.
- Dienstmann, Rodrigo, Cristhiane da Silva Pinto, Margarida Tutungi Pereira, Isabele Avila Small, and Carlos Gil Ferreira. "Palliative percutaneous nephrostomy in recurrent cervical cancer: a retrospective analysis of 50 consecutive cases." Journal of pain and symptom management 36, no. 2 (2008): 185-190.