Second-line treatment options for metastatic castrate-resistant prostate cancer
Cabazitaxel
Cabazitaxel is a new taxane drug with activity in docetaxel-resistant cancers. In the TROPIC study, a Phase III prospective randomized trial, cabazitaxel plus prednisone was compared to mitoxantrone plus prednisone in 755 mCRPC patients, who progressed after or during treatment with docetaxel2 (Figure 1). Patients received a maximum of ten cycles of cabazitaxel or mitoxantrone plus prednisone. Overall survival (OS) was the primary end-point, being significantly longer in cabazitaxel-treated patients (median: 15.1 vs. 12.7 months p < 0.0001). Progression-free survival (PFS) was significantly improved as well (median: 2.8 vs. 1.4 months, p < 0.0001), and prostate-specific antigen (PSA) response rate was also better (39.2% vs. 17.8%, p < 0.0002). Grade 3-4 adverse events developed more significantly in patients taking cabazitaxel, particularly hematological adverse effects (68.2% vs. 47.3%, p < 0.0002).3 Therefore, cabazitaxel should be given with prophylactic granulocyte colony-stimulating factor and needs to be administered by physicians with expertise in handling neutropenia and sepsis.4 When compared to docetaxel in the first-line setting, cabazitaxel was not shown to be superior.5
Figure 1. TROPIC study design
Abiraterone following docetaxel
The COU-AA-301 was a large Phase III randomized trial with a total of 1,195 mCRPC patients being randomised in a 2:1 ratio to abiraterone acetate plus prednisone or placebo plus prednisone (Figure 2). Abiraterone is an antiandrogen agent which inhibits the 17α-hydroxylase/C17,20-lyase (CYP17) enzyme. Initial positive results of this trial were reported after a median follow-up of 12.8 months6 and confirmed by the final analysis.7 All patients in this trial failed at least one chemotherapy regimen, which included docetaxel. The primary end-point was OS, and in the final analysis, after a median follow-up of 20.2 months there was a clear advantage to the abiraterone arm (median survival of 15.8 vs.11.2 months, HR: 0.74, p < 0.0001). The benefit for abiraterone remained in all secondary endpoints as well (PSA, radiologic tissue response, time to PSA or objective progression). No significant difference between the treatment arms was seen in the rate of grade 3-4 adverse events, aside from a higher rate of mineralocorticoid-related side-effects (mainly grade 1-2 fluid retention, edema, and hypokalaemia).7
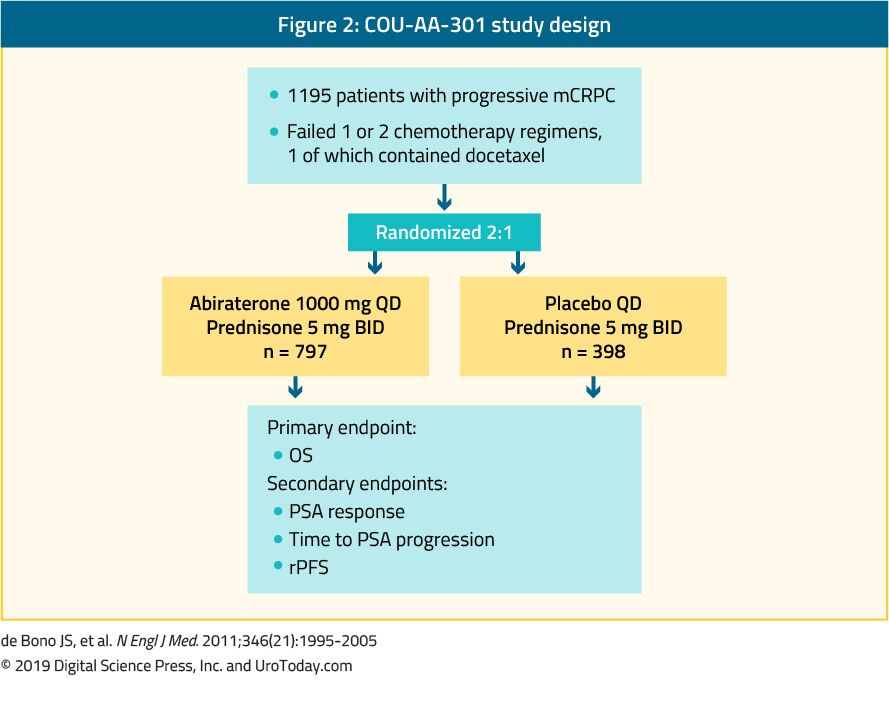
Figure 2. COU-AA-301 study design
Enzalutamide after docetaxel
Enzalutamide after docetaxel
The AFFIRM trial randomized 1,199 mCRPC patients in a 2:1 fashion to enzalutamide, a nonsteroidal antiandrogen, or placebo (Figure 3). All accrued patients had progressed after docetaxel treatment.8 The planned interim analysis of the AFFIRM study was published in 2012 and after a median follow-up of 14.4 months, a clear benefit was shown for the enzalutamide-treated patients (median survival of 18.4 vs. 13.6 months, HR: 0.63, p < 0.001).8 This led to the recommendation to halt and unblind the study. Importantly, the observed benefit occurred irrespective of age, baseline pain intensity, and type of progression. Enzalutamide was also beneficial in patients with visceral metastases. The final analysis with longer follow-up had confirmed the OS results despite the crossover and extensive post-progression therapies. Enzalutamide also conferred a clear advantage in all the secondary endpoints (PSA, soft tissue response, quality of life, time to PSA or objective progression).8 No significant difference in the rate of side-effects was observed in the two groups, with a lower incidence of grade 3-4 adverse events in the enzalutamide arm. Importantly, enzalutamide-treated patients had a 0.6% incidence of seizures compared to none in the placebo arm.8
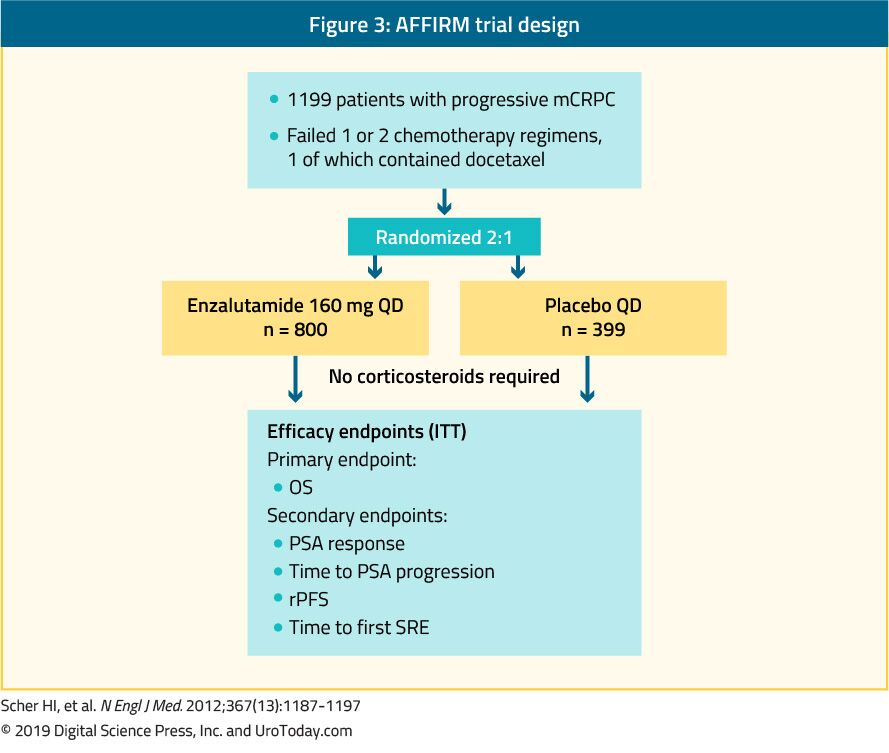
Figure 3. AFFIRM trial design
Apalutamide
Apalutamide
Radium-223
Radium-223 is a targeted alpha therapy and is the only bone-specific drug that has been associated with a survival benefit in the mCRPC space. The ALSYMPCA trial was a large Phase III trial accruing 921 symptomatic mCRPC patients, who failed or were unfit for docetaxel chemotherapy.13 In this trial, patients were randomized to six injections of radium-223 or placebo, plus standard of care in both arms (Figure 4). The primary end-point was OS, and radium-223 significantly improved median OS by 3.6 months (HR: 0.70, p < 0.001).13 Radium-223 also conferred prolonged time to first skeletal event, improvement in pain scores and quality of life.13 No significant difference was noted in the rate of adverse effects between the treatment arms, aside from slightly more haematologic toxicity and diarrhea with radium-223.13 Whether patients were pretreated with docetaxel did not affect the benefit and safety of radium-223.14 Due to safety concerns, the label of radium-223 was restricted to use after docetaxel and at least one AR targeted agent.15 Importantly, the ERA-223 study assessed the effectiveness of early use of radium-223 together with abiraterone acetate and prednisolone (Figure 5). Unfortunately, this trial showed significant safety risks, especially with fractures and more deaths. Therefore, this combination is currently not recommended. These safety risks were more significant in patients without the concurrent use of antiresorptive agents.16
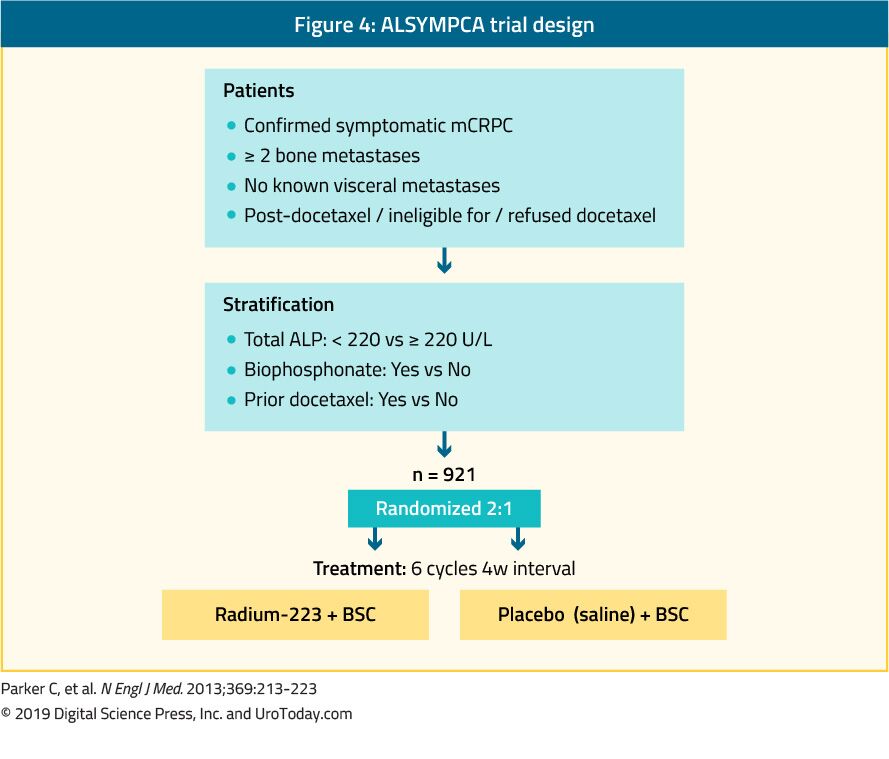
Figure 4. ALSYMPCA trial design
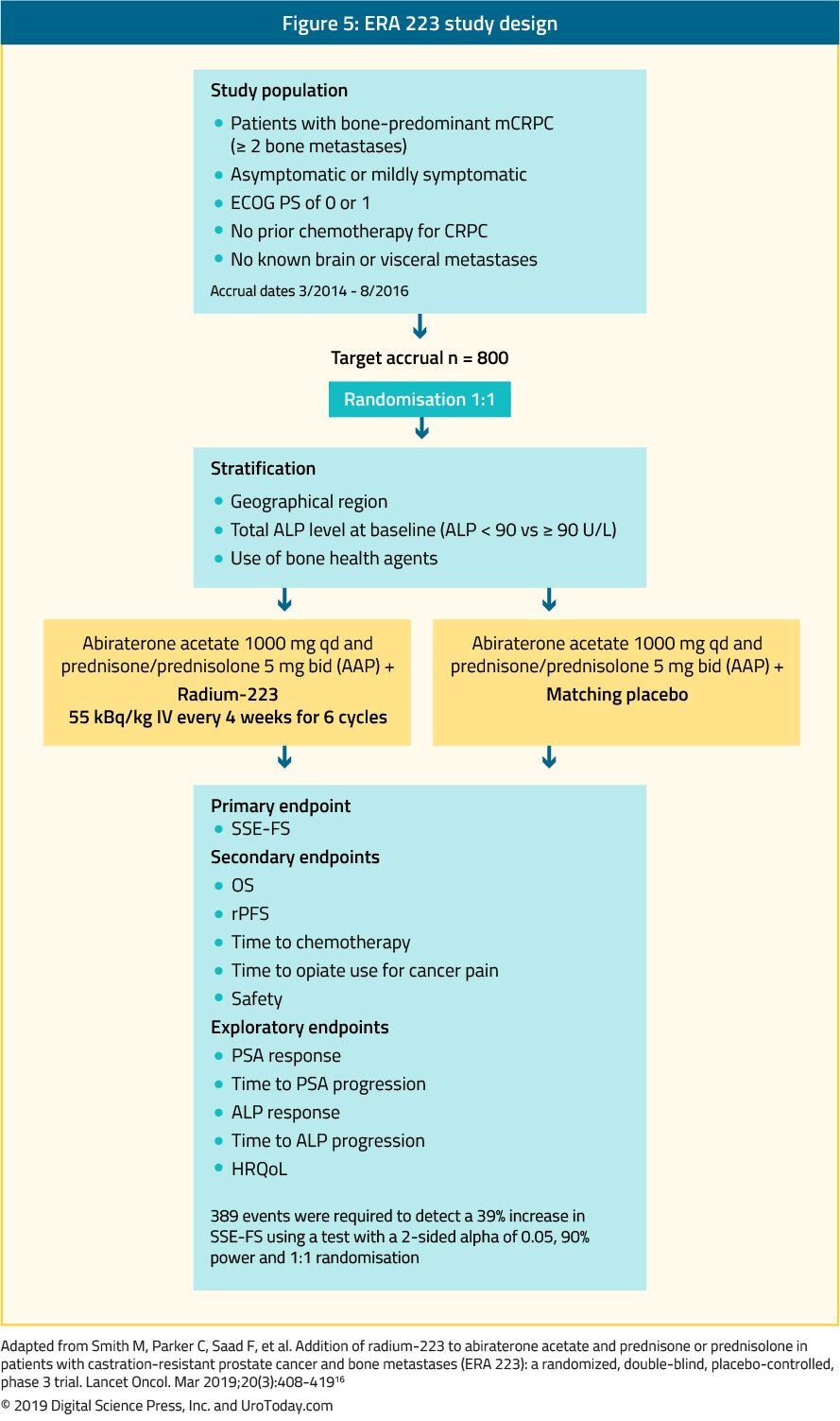
Figure 5. ERA 223 study design
Third line treatment following treatment with docetaxel and one hormonal treatment for metastatic castrate-resistant prostate cancer
Currently, there are no clear guidelines or recommendations regarding which treatment option is appropriate in this setting and this is open for debate. The choice for further treatment after docetaxel and one line of hormonal treatment for mCRPC is unclear.17 The available options include radium-223 or second-line chemotherapy (cabazitaxel). In unselected patients, subsequent treatments are expected to have a lower benefit than with earlier use18. There is also evidence that cross-resistance between enzalutamide and abiraterone exists.19, 20 There is a unique subset of patients worth mentioning with tumors demonstrating homozygous deletions or deleterious mutations in DNA-repair genes. In these patients Poly(ADP-ribose) polymerase (PARP) inhibitors have been reported to confer high rates of response. Therefore, patients who were previously treated with docetaxel and at least one novel hormonal agent; and whose tumors demonstrated homozygous deletions or deleterious mutations in DNA-repair genes showed an 88% response rate to Olaparib, a PAPR inhibitor.21 This represents an example of how treatment can be tailored according to the tumor mutation profile.22 In a randomized Phase II study of mCRPC patients, olaparib combined with abiraterone was compared to placebo and abiraterone. This study demonstrated a clinical benefit in olaparib-treated patients, regardless if mutations in DNA-repair genes existed.23 However, this combination treatment was shown to be toxic with significant side effects reported in 34% of patients vs. only 18% in the placebo arm.23
For patients with mismatch repair deficiency, the PD-1 inhibitor pembrolizumab was approved by the FDA for all tumors, including PCa. More specifically, pembrolizumab demonstrated antitumor activity and disease control with acceptable safety in RECIST-measurable and bone-predominant mCRPC, which was previously treated with docetaxel and novel AR antagonists.24
In the COMET-1 trial 1028 patients with progressive mCRPC after treatment with docetaxel and abiraterone and/or enzalutamide were randomly assigned at a 2:1 ratio to either cabozantinib 60 mg, a tyrosine kinase inhibitor, or prednisone 5 mg twice per day.25 The primary endpoint was OS, and the secondary endpoint included bone scan response after 12 weeks of treatment. Additional exploratory analyses included radiographic PFS (rPFS) and effects on circulating tumor cells, bone biomarkers, serum PSA, and symptomatic skeletal events.25 This trial demonstrated that cabozantinib did not significantly improve OS compared with prednisone in heavily pre-treated mCRPC patients (median OS was 11.0 months with cabozantinib and 9.8 months with prednisone, HR 0.90; 95% CI, 0.76 to 1.06; stratified log-rank P = 0.213).25 Cabozantinib had some activity in improving bone scan response, rPFS, symptomatic skeletal events, and bone biomarkers but not PSA outcomes.25
Changing and sequencing treatment in metastatic castrate-resistant prostate cancer
There are several open questions and dilemmas regarding when to change treatment in mCRPC patients and what is the most appropriate treatment sequence.
The appropriate time to change treatment in mCRPC patients is not entirely clear. No controversy exists regarding the need to change treatment when patients have symptomatic progression of their metastatic disease. Despite the many available treatment options to date, no head to head comparison has been made publicly available, while data assessing the correct sequence of treatment is being assessed. As data are lacking, physicians have been using the ECOG performance score to stratify patients before deciding on the “appropriate” treatment plan. Men with a good performance status are likely to tolerate more treatments as opposed to men with lower performance scores.
The National Comprehensive Cancer Network (NCCN) considers the onset of visceral disease to be a detrimental factor. Patients with liver metastases have especially poor outcomes for as of yet an unknown reason. In a meta-analysis including over 8,000 mCRPC patients who were enrolled in Phase III trials, patients with lymph-node- only disease appeared to have the best OS (median, 31.6 months; 95% CI, 27.9 to 36.6 months), with patients with lung and bone metastases having shorter and similar median OS (19.4 months [95% CI, 17.8 to 20.7 months] vs. 21.3 months [20.8 to 21.9], respectively), and patients with liver metastases demonstrating the worst OS (median, 13.5 months; 95% CI, 12.7 to 14.4 months).26 Therefore, the type of metastases the patient has can be used as a guide to when and how aggressive the treatment strategy should be.
Abiraterone and enzalutamide are highly active agents harboring a substantial effect on PFS, with trials comparing monotherapy with prednisone or placebo.27, 28 However, a subset of patients will not respond to these drugs. A patient who does not respond well will require a change of treatment. It is therefore important to see these patients frequently once starting therapy and assess their response. If no PSA decline is witnessed, the treatment needs to be changed.
When considering the appropriate treatment sequence in mCRPC, there are no clear guidelines or recommendations to date, and our limited knowledge is based mainly on retrospective data. In one non-randomized retrospective study, PFS, OS, and PSA responses from consecutive patients with chemotherapy-naïve mCRPC were compared between those who received abiraterone followed by enzalutamide and those who received enzalutamide followed by abiraterone.29 Initially, a slight improvement in patients who started with abiraterone and transitioned to enzalutamide was seen with improved PFS. An expanded retrospective study confirmed the general trend, showing that patients who started with abiraterone and then transitioned to enzalutamide had better PFS (median, 455 days [95% CI, 385 to 495 days]) than patients who started with enzalutamide and transitioned to abiraterone (median, 296 days; 95% CI, 235 to 358 days).30 However, OS was not significantly different between the groups.30 Furthermore, the authors of an ongoing randomized Phase II study comparing abiraterone vs. enzalutamide in patients with treatment-naïve mCRCP reported their interim results.31 After a median follow-up of 22.3 months, a PSA decline of more than 50% occurred in 34% of abiraterone treated patients compared to 4% in the enzalutamide treated patients (p<0.001).31 Additionally, the median time to PSA progression on 2nd-line therapy was 2.7 vs 1.3 months (HR 0.38, 95% CI 0.26-0.56) in favor of abiraterone.31 Lastly, the median OS was not reached vs 24.3 months (HR 0.82, 95% CI 0.53-1.27) in favor of abiraterone.31 As data regarding appropriate treatment sequencing is still being collected and analyzed, many physicians currently base their decision on which medication to start according to the adverse effects that we want to avoid. Abiraterone is commonly associated with edema, and therefore should be avoided in men with congestive heart failure,27 while enzalutamide is more likely to cause central nervous system toxicity and should probably be avoided in older patients.32
Radioligand therapy for metastatic castrate-resistant prostate cancer patients
PSMA-PET/CT imaging has significantly become more common in recent years. This has led to the emergence of a new field of radioligand directed therapy among heavily pretreated mCRPC patients. PCa metastases express PSMA, making it a promising approach to developing new tracers for targeted radionuclide therapies. PSMA is a non-secreted type II transmembrane protein produced almost exclusively by prostatic tissue and on tumor-associated neovasculature.33 Unlike other biomarkers, such as PSA, which may decrease with increasing neoplastic de-differentiation, PSMA has been shown to be upregulated in high-grade, de-differentiated PCa.34
Since 2015, several institutional studies have reported promising response rates and a favorable safety profile for radioligand therapy with 177Lu-PSMA-617 in mCRPC patients.35-37 However, these studies had small sample sizes and questionable generalizability. To addresses these limitations, a large multicenter German analysis assessed a cohort of patients treated with 177Lu-PSMA-617.38 This study included 145 mCRPC patients treated with 177Lu-PSMA-617 at 12 centers undergoing 1-4 therapy cycles. The study reported an overall biochemical response rate of 45% after all therapy cycles, with 40% of patients responding after a single cycle. Notably, negative predictors of the biochemical response included elevated alkaline phosphatase and the presence of visceral metastases.38
In a large meta-analysis published in 2017, 10 studies were assessed including 369 patients. This meta-analysis assessed the safety and efficacy of 177-Lutetium in mCRPC patients.39 The pooled proportion of patients with any PSA decline was 68% (95% CI: 61–74%); and the pooled proportion of patients with 450% PSA decline was 37% (95% CI: 22–52).39 This meta-analysis suggested promising early results for the treatment of mCRPC patients, especially in patients treated with the more recently developed radioligands, with approximately two-thirds of them showing a biochemical response.39
Although 177Lu-PSMA-617 is the most well-studied radioligand to date, there are additional compounds in development and undergoing initial testing. These include 177Lu-J591, 90Y-J591, 131I-MIP 1095, 177Lu-PSMA-I&T, and 225Ac-PSMA-617.40
Treatment and prevention of skeletal-related events
Patients with mCRPC commonly endure painful bone metastases with external beam radiotherapy (EBRT) being a highly effective treatment.41 Possible complications due to bone metastases include vertebral collapse or deformity, pathological fractures, and spinal cord compression. Cementation can be an effective treatment for a painful spinal fracture, clearly improving both pain and quality of life.42 However, standard palliative surgery can still be offered for managing osteoblastic metastases.43 Impending spinal cord compression is an emergency event that must be recognized as soon as possible. Patients should be educated to recognize the warning signs. If this is suspected, high-dose corticosteroids must be given and an MRI is required. A neurosurgeon or orthopedic surgeon consultation needs to be planned to discuss a possible decompression, followed by EBRT.44
Zoledronic acid, a bisphosphonate, has been evaluated in mCRPC patients in an attempt to reduce skeletal-related events (SRE). 643 mCRPC patients with bone metastases were randomized to receive zoledronic acid, 4 or 8 mg every three weeks for fifteen consecutive months, or placebo.45 The 8 mg dose was poorly tolerated without showing a significant benefit. However, at 15 and 24 months of follow-up, the 4 mg dose conferred fewer SREs compared to the placebo group (44 vs. 33%, p = 0.021), and less pathological fractures (13.1 vs. 22.1%, p = 0.015). Additionally, the time to first SRE was longer in the zoledronic acid group. However, no survival benefit was seen in any prospective trial assessing bisphosphonates.
Denosumab is a fully human monoclonal antibody directed against RANKL (receptor activator of nuclear factor kappa-B ligand). It is a key mediator of osteoclast formation, function, and survival. In non-metastatic CRPC, denosumab has been associated with increased bone-metastasis-free survival compared to placebo (median benefit: 4.2 months, HR: 0.85, p = 0.028).44 Like zoledronic acid, this benefit did not translate into a survival difference and neither the FDA or the EMA had approved denosumab for this indication.46 A Phase III trial compared the efficacy and safety of denosumab (n = 950) with zoledronic acid (n = 951) in mCRPC patients. Denosumab was shown to be superior to zoledronic acid in delaying or preventing SREs, as shown by time to first SRE (pathological fracture, radiation or surgery to bone, or spinal cord compression) of 20.7 vs. 17.1 months, respectively (HR: 0.82, p = 0.008). However, these findings were not associated with any survival benefit, and in a recent post-hoc re-evaluation of end-points, denosumab had actually shown an identical rate of SREs to zoledronic acid.47 It is critical to remember that these medications are associated with substantial toxicity, of 5% and 8.2% in non-metastatic CRPC and mCRPC, respectively.47, 48 All patients are required to be examined by a dentist prior to initiating this therapy, as the risk of jaw necrosis is increased by several risk factors including a history of trauma, dental surgery or dental infection.49 and the number of years the medication is used.
Recently, the randomized, double-blind Phase III trial (COMET-2; NCT01522443) was published, comparing cabozantinib, to mitoxantrone + prednisone in mCRPC patients with narcotic-dependent pain from bone metastases.50 All patients had progressed after treatment with docetaxel and either abiraterone or enzalutamide.50 The primary endpoint was pain response at week 6 and confirmed again at week 12. Enrollment was terminated early because cabozantinib did not demonstrate any survival benefit in mCRPC patients in the companion COMET-1 trial,25 described earlier. At study closure of the COMET-2 trial, only 119 patients were randomized. The trial demonstrated no significant difference in the pain response with cabozantinib versus mitoxantrone-prednisone.50
Future and ongoing trials
There are currently 24 registered ongoing Phase III trials involving mCRPC patients.
Some studies worth mentioning with much-anticipated results include the following:
- The combination of abiraterone and Olaparib as first-line therapy in mCRPC patients (NCT03732820)
- A study assessing the role of Rucaparib (a PARP inhibitor) vs. physician’s choice therapy in mCRPC patients (TRITON3 trial - NCT02975934)
- The combination of pembrolizumab with various other medications including enzalutamide (NCT03834493 - as part of the MK-3475-641/KEYNOTE-641 trial), docetaxel (NCT03834506 - as part of the MK-3475-921/KEYNOTE-921 trial), and olaparib (NCT03834519 – as part of the MK-7339-010/KEYLYNK-010)
- The ACIS trial, which will assess the combination of apalutamide, and abiraterone + prednisone in mCRPC patients (NCT02257736)
- A study assessing Masitinib (a tyrosine kinase inhibitor) plus docetaxel (NCT03761225)
- The combination of Talazoparib (a PARP inhibitor) + plus enzalutamide (NCT03395197),
- The combination of Atezolizumab (an anti-PD-L1 monoclonal antibody) + enzalutamide (NCT03016312)
- The combination of docetaxel and Radium-223 (NCT03574571)
- A study assessing 177Lu-PSMA-617 in mCRPC patients (NCT03511664)
- The IPATential150 trial – assessing the combination of Ipatasertib (an orally administered, ATP-competitive, selective AKT inhibitor) plus abiraterone (NCT03072238)
Conclusions
Substantial progress has been made in the mCRPC space in the last several years. Optimal management of mCRPC patients is a growing challenge as more potential treatments are added to the armamentarium. Choosing the right treatment for the right patient, and the correct sequence and combination of the increasing number of available medications will be the main challenge in the years to come. We currently lack level one evidence regarding the proper sequence and/or combination of current available medications, and physicians are faced with making these decisions without supporting data. Patients will most likely benefit from unique medications with complementary mechanisms of action in order to avoid cross-resistance. An important unmet clinical need thus far consists of acquiring evidence about the efficacy, safety, and tolerability of combination regimens, and optimized approaches for identifying patients most suited for specific treatments.
Published Date: November 19th, 2019