The earliest renal biopsies were obtained by open surgical techniques performed by urologists or transplant surgeons, or by pathologists at the time of autopsy. In 1951, physicians in Copenhagen published the first clinical report of percutaneous renal biopsy.1 They placed patients in a seated position and used intravenous pyelogram (IVP) as the imaging guide. Not surprisingly, both the yield and quality of biopsy tissue samples were low by contemporary standards, with only about half to two-thirds of specimens permitting histologic examination.
Advances in imaging and biopsy techniques have improved this picture, and percutaneous renal biopsy is now a standard practice to help evaluate suspected disorders of the kidney.2,3 Biopsy of the native kidney is performed through the back, with the patient in a prone position. Ultrasonic guidance is used to localize the lower pole of the kidney (unless there is another area of interest). Patient safety and specimen size and quality are both key. Historically, most percutaneous renal biopsies have been performed by nephrologists and radiologists, but many urologists are well-equipped to adopt this procedure into their ambulatory surgery practices. This article is a primer for those who wish to do so.
Indications, patient selection, and precautions
Our urology patients commonly present with a variety of indications for diagnostic renal biopsy. Imaging may identify a renal mass or lesion that requires a focal biopsy to obtain tissue for pathologic evaluation. Patients also may need nonfocal biopsies to evaluate various uropathies, nephropathies, or a suspected rejection of a renal allograft. In all these cases, percutaneous renal biopsy in the ambulatory setting is feasible if patients are carefully selected in order to minimize complications and maximize the likelihood of a successful biopsy. With this in mind, the most common complications of percutaneous renal biopsy include minor bleeding (gross hematuria, subcapsular perinephric hematoma, and capsular hematoma), which affects approximately 21% of patients, and major bleeding, which occurs in approximately 1.5% of cases.2 For this reason, uncorrectable bleeding disorders should be considered an absolute contraindication for percutaneous renal biopsy.
Additional contraindications include poorly controlled hypertension (because this increases the risk of bleeding), an active renal infection, or a solitary kidney (because post-biopsy hemorrhage can lead to the need for nephrectomy).4,5,6 It is important to note that patients with contraindications for percutaneous renal biopsy may be eligible for renal biopsy by means of alternative methods, such as open biopsy, laparoscopic biopsy, or transjugular biopsy.4 These procedures are generally considered safer, although they do introduce potential risks associated with general anesthesia, perioperative complications, and postprocedural recovery, and patients should be educated accordingly.4,6
Studies of post-biopsy complications have utilized a range of follow-up times, which has created some uncertainty about how long to monitor patients following percutaneous renal biopsy in the ambulatory setting.6,7,8 Research also indicates that patients are at highest risk for complications during the first 4 hours after the procedure and that almost 90% of complications occur within the first 24 hours.7 It is important to monitor for hematuria, flank pain, hypotension, and acute renal obstruction,8 and to tell patients and caregivers to watch for relevant signs and symptoms at home.
In my practice, we monitor patients for one hour in the recovery room and also inspect their first voided urine specimen for evidence of gross hematuria.
Equipment costs and reimbursement
The cost of equipment needed to perform a percutaneous renal biopsy in an ambulatory surgery center is fairly low, particularly because most centers already have an ultrasound machine. At the center where I practice, we perform an ultrasound-guided percutaneous renal biopsy with a 16-gauge, 20 or 25-centimeter biopsy gun (which costs approximately $15/gun). Patients receive local anesthesia (1% lidocaine HCl) together with light sedation that is administered by our anesthesia team.
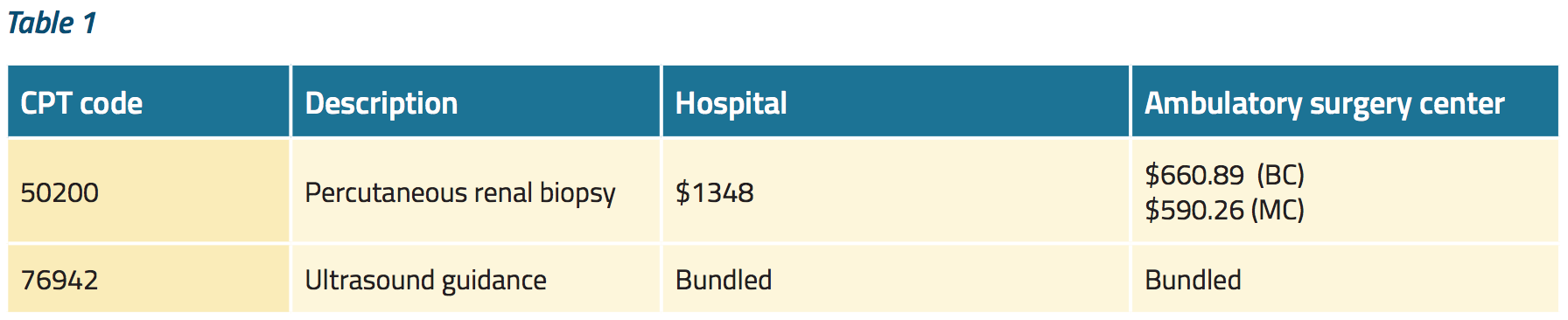
Table 1 shows the relevant reimbursement data for 2018. Note the typical disparity in reimbursement amounts in the hospital and ambulatory surgery settings.
Summary
While percutaneous renal biopsy is not a leading generator of revenue for ambulatory surgery centers, it is a generally quick and safe procedure that many urologists can readily offer their patients. I encourage fellow urologists to consider doing so, especially because we regularly manage patients with obstructive uropathy and other indications for renal biopsy.
Written by: Ashley Baker, MD, University of Mississippi Medical Center, Jackson, Mississippi
References:
1. Iversen, Poul, and Claus Brun. "Aspiration biopsy of the kidney." The American journal of medicine 11, no. 3 (1951): 324-330.
2. Kitterer, Daniel, Katharina Guerzing, Stephan Segerer, M. Dominik Alscher, Kerstin Amann, Niko Braun, and Joerg Latus. "Diagnostic impact of percutaneous renal biopsy." Clinical nephrology 84, no. 6 (2015): 311-322.
3. Wiseman, David A., Ralph Hawkins, Leonard M. Numerow, and Kenneth J. Taub. "Percutaneous renal biopsy utilizing real time, ultrasonic guidance and a semiautomated biopsy device." Kidney international 38, no. 2 (1990): 347-349.
4. Bandari, Jathin, Thomas W. Fuller, I. I. Turner, D. RM, and L. A. Agostino. "Renal biopsy for medical renal disease: indications and contraindications." Can J Urol 23, no. 1 (2016): 8121-8126.
5. Shetye, K. R., L. R. Kavoussi, S. Ramakumar, O. E. Fugita, and Thomas W. Jarrett. "Laparoscopic renal biopsy: a 9‐year experience." BJU international 91, no. 9 (2003): 817-820.
6. Brachemi, Soumeya, and Guillaume Bollée. "Renal biopsy practice: What is the gold standard?." World journal of nephrology 3, no. 4 (2014): 287.
7. Whittier, William L., and Stephen M. Korbet. "Timing of complications in percutaneous renal biopsy." Journal of the American Society of Nephrology 15, no. 1 (2004): 142-147.
8. Maya, Ivan D., and Michael Allon. "ASDIN: Percutaneous renal biopsy: outpatient observation without hospitalization is safe." In Seminars in dialysis, vol. 22, no. 4, pp. 458-461. Oxford, UK: Blackwell Publishing Ltd, 2009.
Related Content:
Download: Everyday Urology: Volume 5, Issue 1