The detection of recurrent tumor is a benchmark by which the success of intravesical agents is determined. Because the U.S. Food and Drug Administration (FDA) will now consider data from single-arm trials for patients with Bacillus Calmette-Guérin (BCG)-unresponsive bladder cancer, the complete response (CR) rates (i.e. absence of disease on biopsy) is a key factor that impacts the success of many registration studies. 2,3,4 In addition, several trials in the neoadjuvant setting focus on p0 rates, meaning that disease is not detected in the final pathologic specimen.5 Since the extent of disease detected depends on the quality of the cystoscopy and an optimally performed TURBT can achieve P0 in up to 15% of patients even without enhanced cystoscopy,5 – clearly this has the potential to impact result.
But performing high-quality TURBTs is not easy. Urologists must accurately assess tumor grade and stage during visual evaluation. She or he must then make an assessment of prognosis and proceed to appropriately resect tumors and suspicious lesions as completely (and deeply) as is required, safe and feasible, plus collect high-quality biopsies for pathologic review.6 In this article, I share practical tips for doing this while minimizing the risk of adverse events. Because tumor detection is key to TURBT outcomes, I also review current data on enhanced cystoscopic imaging.
Tips for Optimizing TURBT
ANESTHESIA
Options for anesthesia should be discussed with patients during preoperative planning.6 Complete paralysis is preferred to decrease movement, minimize motion from abdominal breathing, facilitate resection of the lateral, posterior, and anterior bladder walls, and decrease the likelihood of obturator reflex (obturator jerk).7,8
Until recently, TURBT patients often received epidural or general anesthesia along with either an obturator nerve block or succinylcholine, a short-acting depolarizing neuromuscular blocking agent (NMBA). Succinylcholine effectively prevents obturator reflex but can cause masseter muscle spasm, hyperkalemia, and rhabdomyolysis and it is short acting.9,10,11 The use of longer acting agents such as rocuronium, a non-depolarizing NMBA, was problematic since rocuronium has a longer duration of action and required patients to be under anesthesia for longer periods of time. Fortunately, anesthesiologists now have a safer option: rocuronium can be reversed rapidly by administering the selective relaxant binding agent sugammadex.12,13
CHECKLISTS
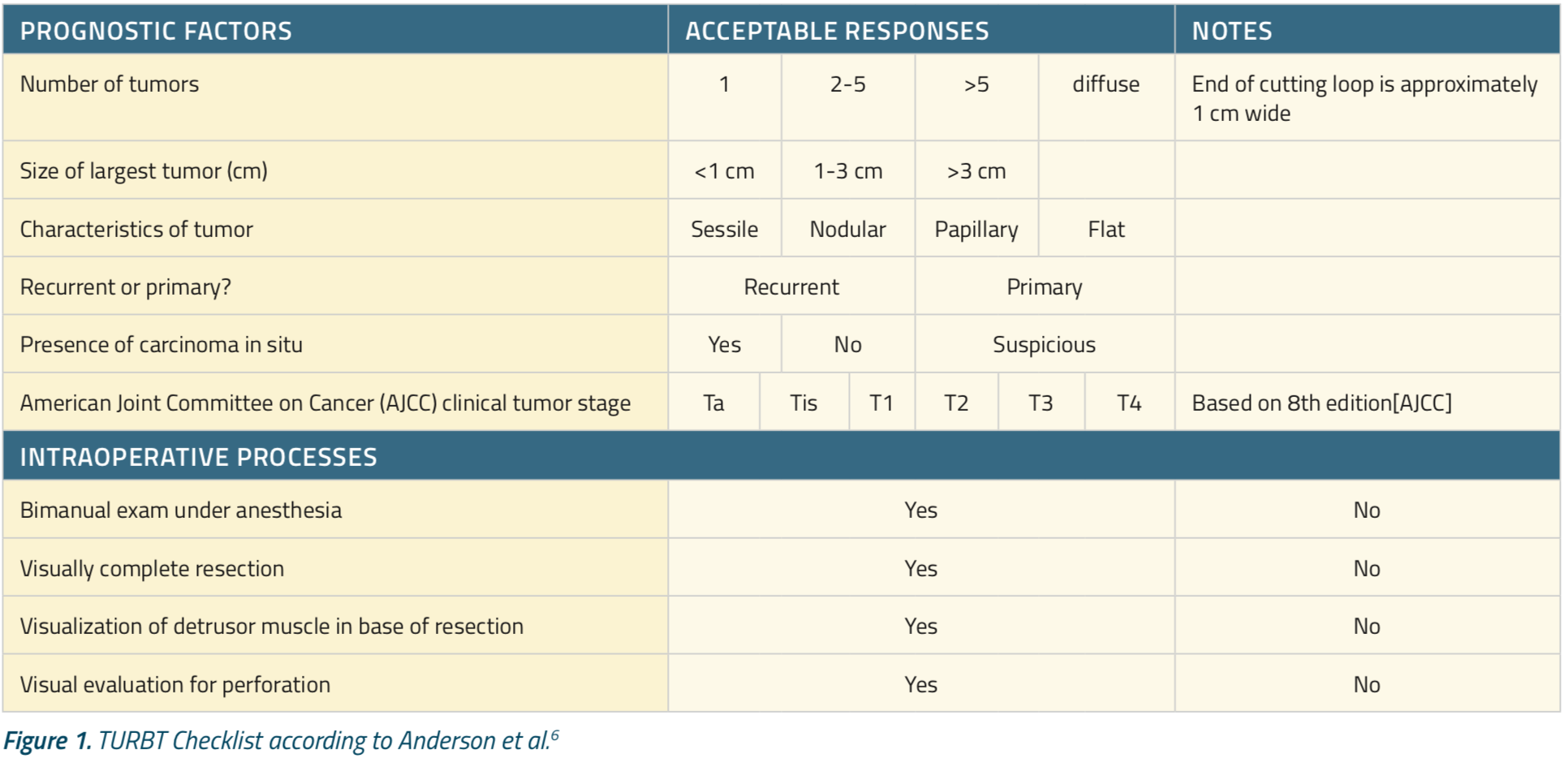
The use of a surgical safety checklist has been found to significantly reduce postoperative complications and 30-day mortality.14,15 For patients with bladder cancer, however, a TURBT-specific checklist also supports procedural quality and the collection and reporting of key information, such as tumor stage and whether intravesical chemotherapy or bimanual examination under anesthesia (EUA) was performed.6,7,16 Such observations and procedural details are vital for planning future cystoscopies.
Robust research supports the use of checklists during TURBT. In a recent large study, implementing a 10-item TURBT checklist markedly improved the documentation of both prognostic and procedural data.6 In another large prospective multicenter study, the implementation of an eight-item TURBT checklist was associated with a significant reduction in the risk of bladder cancer recurrence (P=.02).17 I personally highly recommend using a checklist during every TURBT. An example of a checklist is shown in Figure 1.
Several more tips can help optimize TURBT. First, avoid placing the resectoscope sheath blindly since one can miss a urethral lesion.6 Instead, visualization allows for urethroscopy and collection of non-traumatic urine for cytology at bladder entry. After entering the bladder, if needed, barbotage can increase cellular yield. Once this is done, continue using all the lenses at your disposal: 30 and 70-degree lenses for mapping the bladder, and a 120-degree lens or a flexible cystoscope for the bladder neck.6 This will prevent an unfortunate situation which I see not uncommonly: tumors at the bladder neck and anterior wall that have clearly been ‘missed’. It is important to correctly assess tumor grade and stage to guide decisions about whether to perform deep resection with musclularis propria removed (for high-grade [HG] tumors) or a less aggressive resection with cauterization of the tumor base (for low-grade tumors. In addition, one must often decide on whether to instill perioperative adjuvant therapy with gemcitabine or mitocycin C, which has the most impact in low-grade tumors. We are better at this than you might think. In one study, urologists correctly classified 85 of 86 (99%) LGTa tumors in patients with negative urinary cytology.18 In another study, urologists misclassified only 7% of large HG tumors as LG, while correctly identifying 93% and 85% of non-muscle invasive and muscle-invasive bladder tumors, respectively.19 Keep in mind that the great majority of bladder tumors are TaLG, and many of these patients experience successive tumor events. Thus, it is key to minimize trauma to the bladder by reserving deep resection for high-grade tumors.6 Of course, in the case of high-grade T1 tumors, a deep resection is required. Here, be kind to your pathologist: submit a separate biopsy of the base of large or T1HG tumors so that the depth of muscle invasion can more easily be assessed. Another option for improving pathologic staging of smaller (3 cm or less) tumors is en bloc resection.20,21 This technique uses a needle to mark the tumor borders. The needle is then inserted through the marked borders into the bladder wall, the tumor tissue is pulled away, and the tumor is removed with blunt dissection. Point cautery is acceptable to detach the final fibers, but the tumor base is not cauterized, which conserves its 3-dimensional architecture.21
Some experts posit that en bloc resection also decreases shedding and scattering of tumor cells, which might reduce the risk of early recurrence.22 Unlike monopolar electrocautery, bipolar electrocautery restricts electrical current between two polarized elements, enabling the current to bypass the patient. This allows less ‘charring’ of the tissue.7 Isotonic saline also can be used during bipolar electrocautery, which decreases the risk of complications such as hypotonic (low sodium) syndromes.7 Fortunately, such complications are so rare that the superiority of bipolar versus monopolar cautery is slight in absolute terms.7 Nonetheless, a meta-analysis of six prospective trials and two observational studies comparing monopolar with bipolar electrocautery linked the latter with small but statistically significant reductions in operative and catheterization times, hospital length of stay, blood loss, and rates of obturator nerve reflex and bladder perforation.23 Interestingly, bipolar cautery also was associated with a lower rate of recurrence at 2-year follow-up.
Enhanced Cystoscopy
BLUE LIGHT CYSTOSCOPY
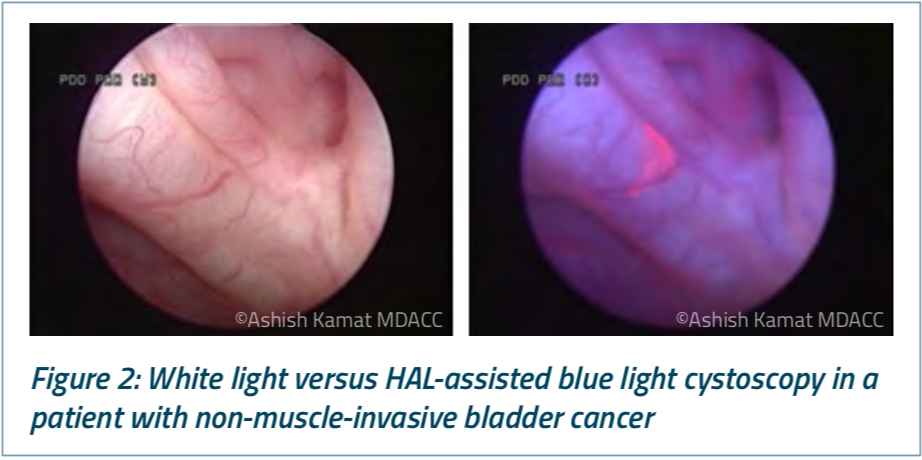
Hexaminolevulinate (HAL; Cysview®), a hexyl derivative of aminolevulinic acid, was approved by the United States Food and Drug Administration (FDA) in 2010 as an adjunct to standard white light cystoscopy for detecting non-muscle invasive bladder cancer, particularly papillary tumors.24 Currently, Cysview® is only approved for use with Karl Storz D-Light C Photodynamic Diagnostic (PDD) systems.
Hexaminolevulinate has been studied in five multicenter phase III trials of more than 1,800 patients with known or suspected bladder cancer.25,26,27,28,29 Among these studies, the pivotal randomized trial leading to the FDA approval of Cysview® included 286 patients with biopsy-confirmed Ta or T1 tumors who underwent white light cystoscopy with or without HAL-assisted blue light cystoscopy.25 In all, 16.4% of tumors were detected only by blue light cystoscopy (P=.001), including 46% of CIS lesions (P< .0001). The frequency of false positives was equal between groups (11%).
Blue light cystoscopy also was evaluated in a recent multicenter, prospective real-world registry study of 533 U.S. patients with known or suspected non-muscle-invasive bladder cancer.30 White light cystoscopy detected 76% of malignant lesions, blue light alone detected 91%, and the two tools together detected 98.5%. Similar to the pivotal trial,25 blue light cystoscopy increased the detection of CIS and papillary lesions by 43% and 12%, respectively.30 Blue light cystoscopy also led to a change in the management of 14% of patients.
EFFECTS OF BLUE LIGHT CYSTOSCOPY ON RECURRENCE AND PROGRESSION
The use of blue light cystoscopy helps us teach, train, and perform better resections. But does it improve longer-term outcomes? In the pivotal trial of Cysview®, similar proportions of patients in each arm received intravesical therapy, but patients in the blue-light arm had a significantly decreased rate of recurrence at 9 months (47%, vs. 56% with white light only; P=.026).31 This effect persisted at 54 months, when 38% and 31.8% of patients remained tumor-free, respectively, for a median recurrence-free survival of 16.4 months versus 9.6 months (P = .04).32 Blue light cystoscopy also showed a trend toward a lower risk of cystectomy.32
Does blue light cystoscopy also prevent or postpone progression? Historically, this endpoint - of progression of NMIBC - was defined inconsistently, imprecisely, and often only applied to the state when NMIBC moved to MIBC or metastatic disease. To rectify this problem, the International Bladder Cancer Group (IBCG) recently defined progression of bladder cancer as any of the following: increase in T stage leading to invasion of the lamina propria (T1 disease), the development of muscle-invasive disease (stage T2 or greater), progression to lymph node (N+) or distant metastasis (M1), or an increase from low to high tumor grade.33
When this definition was subsequently applied to the pivotal trial of Cysview®,32 adjunctive HAL-assisted blue light cystoscopy was found to reduce the risk of progression and the effect approached statistical significance (P = .085). Blue light cystoscopy also was associated with a longer median time to progression (P = .05) and a higher probability of progression-free survival (P=.05), possibly because of bladder cancer was detected and resected earlier.34
Also noteworthy is a meta-analysis of five studies in which 1,301 patients with non-muscle-invasive bladder cancer underwent TURBT with white light with or without HAL-assisted blue light cystoscopy.35 After approximately 28 months of follow-up, rates of progression were 10.7% and 6.8%, respectively, yielding a 64% greater odds of progression with white light cystoscopy only (odds ratio, 1.64, 95% confidence interval [CI], 1.10 to 2.45; P=.01).35
Based on these data, the addition of blue light to white light cystoscopy can be said to potentially have a favorable effect on risk of progression of bladder cancer. However, we need longer-term follow-up and more studies to draw definitive conclusions.
OUTPATIENT AVAILABILITY OF BLUE LIGHT CYSTOSCOPY
Until recently, blue light cystoscopy usually was not performed in outpatient settings because it was not available for use with an FDA-approved non-rigid cystoscope. While many of us remember performing rigid cystoscopies in clinical settings with local anesthesia, with the advent and use of flexible scopes, this practice is uncommon. In February 2018, the FDA approved a supplemental new drug application to extend the indication of Cysview® to include its use with the flexible version of the Karl Storz D-Light C Photodynamic Diagnostic system.24 This effectively expanded the use of HAL-assisted blue light cystoscopy into outpatient settings.
In the randomized phase III clinical trial spurring this new approval, researchers at 17 U.S. sites compared white light flexible cystoscopy alone with adjunctive HAL-assisted blue light flexible cystoscopy for the office-based surveillance of patients with non-muscle invasive bladder cancer at high risk for recurrence.36 Among 63 patients with histologically confirmed malignancies, 13 lesions (20.6%; 95% CI, 11.5% to 32.7%) were only detected by blue light cystoscopy (P<.0001), including one high-grade Ta tumor, six low-grade (LG) Ta tumors, one papillary urothelial neoplasm of low malignant potential (PUNLMP), and five CIS. None of the patients with CIS tumors had positive cytology and had no history of CIS. Furthermore, 34.6% of CIS lesions were only detected by blue light cystoscopy (95% CI, 17.2% to 55.7%).
Importantly, HAL-assisted blue light cystoscopy detected additional tumors in 46% of trial participants.36 This implies that if we opt not to use blue light cystoscopy in patients with negative cytology, we might miss close to half of these additional recurrent bladder tumors. Therefore, I recommend against relying on cytology alone when deciding whether to perform blue light cystoscopy. Instead, one should take all known risk factors for recurrence into account.
NARROW BAND IMAGING
Narrowband imaging is an alternative method of advanced cystoscopic imaging that does not require the use of fluorescent dyes. Instead, optical filters are placed in the light source of the video endoscope system, narrowing the bandwidth of emitted light emitted to between 415 and 540 nm.7 This increases the rel- ative intensity of blue and green light while minimizing red light. Hemoglobin strongly absorbs green and blue light, increasing the contrast between mucosal tissue and surface capillaries and submucosal blood vessels.
In six separate cohort studies, narrow band imaging detected bladder tumors with a sensitivity of 93% to 100%, and with a specificity of 69% to 85%.37,38,39,40,41,42 Notably, 12% to 27% of tumors were only detected with narrow band imaging.
Recently, the single-blind, randomized, multicenter trial Clinical Research Office of the Endourological Society (CROES) trial compared TURBT with either white light or narrow band imaging among 965 patients with non-muscle-invasive bladder cancer.43 Narrowband imaging did not significantly reduce overall rates of recurrence (27.1% vs. 25.4%, respectively). However, among patients at low risk for recurrence (those without CIS and with solitary TaLG tumors measuring less than 30 mm), TURBT with narrow band imaging reduced the rate of recurrence by nearly five-fold (5.6%) compared with white light-assisted TURBT (27.3%; P=.002). Since these are the very patients who typically receive TURBT without additional adjuvant intravesical chemotherapy or BCG, narrow band imaging clearly helps these patients.
Finally, we should consider the multicenter DaBlaCa-7 study, which examined the clinical relevance of narrow band imaging when used with flexible cystoscopy.44 The study included 955 Danish patients with either hematuria or known recurrence of non-muscle-invasive bladder cancer. Patients received white light cystoscopy, a clinical decision was made, and narrow band imaging cystoscopy was then performed. In all, 23% of patients had tumors identified by white light cystoscopy Narrow band imaging detected additional tumors in 7% of these patients and altered clinical decision-making in 1.9% of patients. Among patients with recurrent non-muscle-invasive bladder cancer, narrow band imaging also was significantly more sensitive than white light cystoscopy alone (100% vs. 83.2%; P<.05).44
Narrowband imaging did lead to a higher rate of false positives in this study (respective specificities, 86.5% vs. 92.1% with white light; P<.05). Blue light cystoscopy also has been tied to a small increase in false positives; in the prospective registry study, the rate was 30% versus 25% with white light cystoscopy alone. In my experience, false positives become less with common with experience and do not outweigh the advantages of either technique.
GUIDELINES FOR AND REIMBURSEMENT OF ENHANCED CYSTOSCOPY
Based on all the data available, joint guidelines from the American Urological Association (AUA) and the Society of Urologic Oncology (SUO) state that clinicians should offer blue light cystoscopy with Cysview®, if available, at the time of TURBT to patients with non-muscle invasive bladder cancer to improve rates of detection and recurrence.45 The guideline authors classify this recommendation as moderate based on B-grade evidence.
These joint AUA/SUO guidelines also state that clinicians may consider the use of narrow band imaging to increase detection and decrease recurrence of non-muscle-invasive bladder cancer, based on C-grade evidence. The difference in strength between these recommendations reflects the more abundant and robust evidence supporting the clinical value blue light cystoscopy over white light cystoscopy alone.
In addition to clinical benefits, cost and reimbursement are additional considerations. Studies indicate that HAL-assisted blue light cystoscopy ultimately is more cost-effective than standard white light cystoscopy alone. In a recent analysis of U.S. data, for example, initial TURBT performed with both blue and white light cystoscopy was projected to save more than $4,600 per patient over 5 years, compared with white light cystoscopy only.46 By preventing or postponing the recurrence and progression of bladder cancer, blue light cystoscopy can avoid the cost, pain, and risk of additional operations.47
In keeping with these findings, the Centers for Medicare and Medicaid Services (CMS) has established a new permanent reimbursement code (A9589: “instillation, hexaminolevulinate hydrochloride”) for HAL-assisted blue light cystoscopy performed with a flexible cystoscope.48,49 The CMS also has increased its reimbursement of some (but not all) hospital-based procedures in which Cysview® is used.
SUMMARY
Bladder cancer is a complex disease. The initial step in the diagnosis and management of all patients is a well-performed cystoscopy and tumor resection. When optimally performed, TURBT not only provides the correct diagnosis but also prevents or delays recurrence and progression and reduces the burden of management of successive tumor events. Achieving this standard requires not only technical skill but also due diligence and attention to details. During every TURBT, complete, accurate, and systematic recording of procedural decisions and clinical and prognostic data are paramount.
Multiple studies support the clinical and economic value of enhanced cystoscopy for both bladder cancer surveillance and TURBT. Blue light cystoscopy and narrow band imaging have distinct advantages. I use both techniques regularly in my practice personalizing the choice to the specific patient and situation.
Written by: Ashish M. Kamat, MD, MBBS, is a Professor (Tenure) of Urology and Director of Urologic Oncology Fellowship at M.D. Anderson Cancer Center, and a graduate of the AUA Leadership Program. Dr Kamat has authored over 200 publications, editorials & book chapters in prestigious journals; he is listed in ‘Who’s Who in Medicine’ and ‘Best Doctors in America’ and has won the Compassionate Doctor Award from patient groups. He is an exceptional educator nominated twice for the Robert M. Chamberlain Distinguished Mentor Award and has been invited as a visiting professor to several universities across the world. Dr. Kamat is Co-President, International Bladder Cancer Network, Chair, Bladder Cancer Think Tank (2015), Chair, Bladder Cancer Task Force for SITC, actively participates in various global urologic efforts, and serves on the board of regional and national societies for Urology.
References:
- Fernández MI, Brausi M, Clark PE, et al. Epidemiology, prevention, screening, diagnosis, and evaluation: update of the ICUD-SIU joint consultation on bladder cancer. World J Urol. 2019 Jan;37(1):3-13. doi: 10.1007/s00345-018-2436-y. Epub 2018 Aug 13.
- BCG-unresponsive nonmuscle invasive bladder cancer: developing drugs and bio-
logics for treatment guidance for industry. https:/www.fda.gov/downloads/Drugs/ GuidanceComplianceRegulatoryInformation/Guidances/UCM529600.pdf Accessed November 26, 2018. - Kamat AM, Sylvester RJ, Böhle A, et al. Definitions, end points, and clinical trial designs for non-muscle-invasive bladder cancer: recommendations from the International Bladder Cancer Group. J Clin Oncol 2016 Jun;34(16):1935-1944.
- Klaassen Z, Kamat AM, Kassouf W, et al. Treatment strategy for newly diagnosed T1 high-grade bladder urothelial carcinoma: new insights and updated recommendations. Eur Urol 2018 Nov;74(5):597-608.
- Kassouf W, Spiess PE, Brown GA, et al. P0 stage at radical cystectomy for bladder cancer is associated with improved outcome independent of traditional clinical risk factors. Eur Urol 2007 Sep;52(3):769-774.
- Anderson C, Weber R, Patel D, et al. A 10-Item Checklist Improves Reporting of Critical Procedural Elements during Transurethral Resection of Bladder Tumor. J Urol 2016 Oct;196(4):1014-1020.
- Black P, Gontero P. Bladder Cancer: A Joint SIU-ICUD International Consultation. Lisbon, Portugal: Société Internationale d’Urologie (SIU). 2017.
- Panagoda PI, Vasdev N, et al. Avoiding the obturator jerk during TURBT. Curr Urol. 2018 Oct;12(1):1-5.
- Cesur M, Erdem AF, Alici HA, et al. The role of succinylcholine in the prevention of the obturator nerve reflex during transurethral resection of bladder tumors. Saudi Med J 2008 May;29(5):668-671.
- Martyn JA, Richtsfeld M. Succinylcholine-induced hyperkalemia in acquired pathologic states: etiologic factors and molecular mechanisms. 2006 Jan;104(1):158-169.
- Schaller SJ, Fink H. Sugammadex as a reversal agent for neuromuscular block: an evidence-based review. Core Evid 2013 Sep;8:57-67.
- Magorian T, Flannery KB, Miller RD. Comparison of rocuronium, succinylcholine, and vecuronium for rapid-sequence induction of anesthesia in adult patients. Anesthesiology. 1993 Nov;79(5):913-918.
- Naguib M, Brull SJ. Sugammadex: a novel selective relaxant binding agent. Expert Rev Clin Pharmacol 2009 Jan;2(1):37-53.
- Haynes AB, Weiser TG, Berry WR, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med 2009 Jan;360(5):491-499.
- van Klei WA, Hoff RG, van Aarnhem EE, et al. Effects of the introduction of the WHO "Surgical Safety Checklist" on in-hospital mortality: a cohort study. Ann Surg. 2012 Jan;255(1):44-49.
- Pan D, Soloway MS. The importance of transurethral resection in managing patients with urothelial cancer in the bladder: proposal for a transurethral resection of bladder tumor checklist. Eur Urol 2012 Jun;61(6):1199-1203.
- Suarez-Ibarrola R, Soria F, Abufaraj M, et al. Surgical checklist impact on recurrence-free survival of patients with non-muscle-invasive bladder cancer undergoing transurethral resection of bladder tumour. BJU Int 2018 Sep 24. [Epub ahead of print]
- Herr HW. Pathologic evaluation of radical cystectomy specimens. Cancer 2002 Aug;95(3):668-669.
- Mariappan P, Lavin V, Phua CQ, et al. Predicting grade and stage at cystoscopy in newly presenting
bladder cancers-a prospective double-blind clinical study. Urology 2017 Nov;109:134-139. - Ukai R, Kawashita E, Ikeda H. A new technique for transurethral resection of superficial bladder
tumor in 1 piece. J Urol 2000 Mar;163(3):878-879. - Ukai R, Hashimoto K, Iwasa T, et al. Transurethral resection in one piece (TURBO) is an accurate tool for pathological staging of bladder tumor. Int J Urol 2010 Aug;17(8):708-714.
- Sznurkowski JJ. En bloc pelvic resection for advanced ovarian cancer preceded by central ligation of vessels supplying the tumor bed: a description of surgical technique and a feasibility study. World J Surg Oncol 2016 Apr;14:133.
- Zhao C, Tang K, Yang H, et al. Bipolar versus monopolar transurethral resection of nonmuscle-invasive bladder cancer: a meta-analysis. J Endourol. 2016 Jan;30(1):5-12.
- Highlights of prescribing information. Cysview (hexaminolevulinate hydrochloride), for Intravesical Solution. https:/www.accessdata.fda.gov/drugsatfda_docs/label/2018/022555s005lbl.pdf Accessed December 5, 2018.
- Stenzl A, Penkoff H, Dajc-sommerer E, et al. Detection and clinical outcome of urinary bladder cancer with 5-aminolevulinic acid-induced fluorescence cystoscopy: A multicenter randomized, double-blind, placebo-controlled trial. Cancer 2011 Mar;117(5):938-947.
- Hermann GG, Mogensen K, Carlsson S, et al. Fluorescence-guided transurethral resection of bladder tumours reduces bladder tumour recurrence due to less residual tumour tissue in Ta/T1 patients: a randomized two-centre study. BJU Int 2011 Oct;108(8 Pt 2):E297-E303.
- Grossman HB, Gomella L, Fradet Y, et al. A phase III, multicenter comparison of hexaminolevulinate fluorescence cystoscopy and white light cystoscopy for the detection of superficial papillary lesions in patients with bladder cancer. J Urol 2007 Jul;178(1):62-67.
- Schmidbauer J, Witjes F, Schmeller N, et al. Improved detection of urothelial carcinoma in situ with hexaminolevulinate fluorescence cystoscopy. J Urol 2004 Jan;171(1):135-138.
- Jocham D, Witjes F, Wagner S, et al. Improved detection and treatment of bladder cancer using hexaminolevulinate imaging: a prospective, phase III multicenter study. J Urol 2005 Sep;174(3):862-866.
- Daneshmand S, Bazargani ST, Bivalacqua TJ, et al. Blue light cystoscopy for the diagnosis of bladder cancer: Results from the US prospective multicenter registry. Urol Oncol. 2018 Aug;36(8):361. e1-361.e6. doi: 10.1016/j.urolonc.2018.04.013. Epub 2018 May 30.
- Stenzl A, Burger M, Fradet Y, et al. Hexaminolevulinate guided fluorescence cystoscopy reduces recurrence in patients with nonmuscle invasive bladder cancer. J Urol. 2010 Nov;184(5):1907-13. doi: 10.1016/j.juro.2010.06.148. Epub 2010 Sep 17
- Grossman HB, Stenzl A, Fradet Y, et al. Long-term decrease in bladder cancer recurrence with hexaminolevulinate enabled fluorescence cystoscopy. J Urol 2012 Jul;188(1):58-62.
- Lamm D, Persad R, Brausi M, et al. Defining progression in nonmuscle invasive bladder cancer: it is time for a new, standard definition. J Urol 2014 Han;191(1):20-27.
- Kamat AM, Cookson M, Witjes JA, et al. The impact of blue light cystoscopy with hexaminolevulinate (hal) on progression of bladder cancer - a new analysis. Bladder Cancer 2016 Apr;2(2):273-278.
- Gakis G, Fahmy O. Systematic Review and meta-analysis on the impact of hexaminolevulinate- versus white-light guided transurethral bladder tumor resection on progression in non-muscle invasive bladder cancer. Bladder Cancer 2016 Jul;2(3):293-300.
- Daneshmand S, Patel S, Lotan Y, et al. Efficacy and safety of blue light flexible cystoscopy with hexaminolevulinate in the surveillance of bladder cancer: a phase III, comparative, multicenter study. J Urol. 2018 May;199(5):1158-1165.
- Bryan RT, Billingham LJ, Wallace DM. Narrow-band imaging flexible cystoscopy in the detection of recurrent urothelial cancer of the bladder. BJU Int 2008 Mar;101(6):702-705.
- Cauberg EC, Kloen S, Visser M, et al. Narrow band imaging cystoscopy improves the detection of non-muscle-invasive bladder cancer. Urology 2010 Sep;76(3):658-663.
- Shen YJ, Zhu YP, Ye DW, et al. Narrow-band imaging flexible cystoscopy in the detection of primary non-muscle invasive bladder cancer: a "second look" matters? Int Urol Nephrol 2012 Apr;44(2):451-457.
- Herr HW, Donat SM. A comparison of white-light cystoscopy and narrow-band imaging cystoscopy to detect bladder tumour recurrences. BJU Int 2008 Nov;102(9):1111-1114.
- Tatsugami K, Kuroiwa K, Kamoto T, et al. Evaluation of narrow-band imaging as a complementary method for the detection of bladder cancer. J Endourol 2010 Nov;24(11):1807-1811.
- Chen G, Wang B, Li H, et al. Applying narrow-band imaging in complement with white-light imaging cystoscopy in the detection of urothelial carcinoma of the bladder. Urol Oncol 2013 May;31(4):475-479.
- Naito S, Algaba F, Babjuk M, et al. The Clinical Research Office of the Endourological Society (CROES) Multicentre Randomised Trial of Narrow Band Imaging-Assisted Transurethral Resection of Bladder Tumour (TURBT) Versus Conventional White Light Imaging-Assisted TURBT in Primary Non-Muscle-invasive Bladder Cancer Patients: Trial Protocol and 1-year Results. Eur Urol 2016 Sep;70(3):506-515.
- Drejer D, Béji S, Munk Nielsen A, et al. Clinical relevance of narrow-band imaging in flexible cystoscopy: the DaBlaCa-7 study. Scand J Urol 2017 Apr;51(2):120-123.
- American Urological Association. Diagnosis and Treatment of Non-Muscle Invasive Bladder Cancer: AUA/SUO Joint Guideline. http:/www.auanet.org/guidelines/bladder-cancer-non-muscle-inva- sive-(2016) Accessed December 9, 2018.
- Garfield SS, Gavaghan MB, Armstrong SO, et al. The cost-effectiveness of blue light cystoscopy in bladder cancer detection: United States projections based on clinical data showing 4.5 years of follow up after a single hexaminolevulinate hydrochloride instillation. Can J Urol 2013 Apr;20(2):6682-6689.
- Witjes JA and Hendricksen K. Intravesical pharmacotherapy for non-muscle-invasive bladder cancer: a critical analysis of currently available drugs, treatment schedules, and long-term results. Eur Urol. 2008 Jan;53(1):45-52. Epub 2007 Aug 20.
- Centers for Medicaid & Medicare Services. Centers for Medicare & Medicaid Services (CMS) Healthcare Common Procedure Coding System (HCPCS) Application Summaries for Drugs, Biologicals and Radiopharmaceuticals. https:/www.cms.gov/Medicare/Coding/MedHCPCSGenInfo/ Downloads/2018-05-15-HCPCS-Application-Summary.pdf Accessed December 9, 2018.
- Centers for Medicaid & Medicare Services. 2019 HCPCS Alpha-Numeric Index. https:/www.cms. gov/Medicare/Coding/HCPCSReleaseCodeSets/Downloads/2019-HCPCS-Index.pdf Accessed December 9, 2018.
- American Joint Committee on Cancer. Urinary Bladder. Amin MB, Edge S, Greene F, Byrd DR, Brookland RK, et al, eds. AJCC Cancer Staging Manual. 8th ed. New York: Springer; 2017.