Prostate cancer is the leading incident cancer among men, and population growth and aging have fueled a 40% rise in global case burden since 2006.1,2 Despite recent improvements in treatment, patients with locally advanced and advanced prostate cancer experience significant emotional distress, diminished quality of life, and increased risk of cancer-specific mortality.1,2,3 Orchiectomy and androgen-deprivation therapy (ADT) have been mainstays for treating advanced and metastatic prostate cancer since the groundbreaking work of Huggins in the early 1940s.4 Today, ADT remains the leading systemic therapy for locally advanced and metastatic disease, with up to half of the patients receiving it sometime during their disease course.5
Gonadotrophin-releasing hormone (GnRH) agonists, such as leuprolide, goserelin, histrelin, or triptorelin, are most often used and induce responses in approximately 85% of men with metastatic hormone-sensitive prostate cancer.6,7 Unfortunately, these drugs are associated with clinically significant toxicities, many of which overlap, such as cardiovascular disease, hypertension, adiposity, sarcopenia, and a variant of metabolic syndrome.6,7 In response, researchers are studying alternative mechanisms of medical castration as well as behavioral strategies to reduce the cardiometabolic risks of ADT.
At the same time, our treatment armamentarium has expanded and is shifting toward the earlier use of docetaxel, second-line ADT, and combinations. This diversifying treatment landscape heightens the need to understand the cardiovascular and metabolic risks of ADT and how best to manage them.
Evaluating cardiovascular and metabolic risk
Older age is associated with diabetes, cardiovascular disease, and prostate cancer, so it’s not surprising how often these conditions overlap. Indeed, cardiovascular disease is the second leading cause of death in men with prostate cancer and the primary cause of death in men with T3 or lower-stage disease.8
We have known since the 1970s that estrogens such as diethylstilbestrol (DES) are associated with cardiovascular risks.9 More recently, studies have linked bilateral orchiectomy, GnRH agonist therapy, and combined androgen blockade to increased risk of cardiovascular morbidity and mortality.5,10
We have the most data on GnRH agonists since they are most often prescribed. Most studies have found that these drugs carry a greater cardiovascular risk than other types of ADT. In a recent review, GnRH agonist therapy was associated with a 20% to 25% increase in the risk of cardiovascular morbidity compared with no ADT.11 In another study of Surveillance, Epidemiology, and End Results (SEER) and Medicare data, GnRH agonists were associated with a significantly higher risk of coronary artery disease, acute myocardial infarction, and sudden cardiac death compared with orchiectomy.12 In another recent meta-analysis, GnRH agonists were associated with a greater risk of incident cardiovascular disease compared with orchiectomy or antiandrogen monotherapy.13 Not all data point the same way, however. In a large observational study in Sweden, men with prostate cancer who received a GnRH agonist had a statistically similar risk of incident cardiovascular events and mortality as men who underwent orchiectomy.14
For patients with a history of cardiovascular disease, we have limited evidence that degarelix is cardiovascularly safer than GnRH agonist therapy. Most data comparing GnRH agonists and antagonists are retrospective and observational,15 but recently, a randomized, two-center, open-label trial assessed the cardiovascular safety of degarelix and GnRH agonists in 80 men with prostate cancer and pre-existing cardiovascular disease.16 After a median follow-up time of 10 months, rates of incident cardiovascular events were 7% for degarelix versus 28% for GnRH agonists (P = .008).16 Additionally, patients whose FSH level had dropped by less than 60% during the first 3 months of treatment were at significantly increased risk of cardiovascular events.16
Other studies generally confirm these findings. In a pooled analysis of data from clinical trial participants with prostate cancer and pre-existing cardiovascular disease, degarelix was associated with an approximately 50% lower rate of incident cardiac events at 1 year compared with GnRH agonists (FIGURE 1), even after controlling for confounding factors.17 In another recent analysis of hospital discharge data and insurance claims, GnRH antagonist therapy was associated with a significantly lower risk of myocardial infarction or ischemic stroke compared with GnRH agonist therapy.18
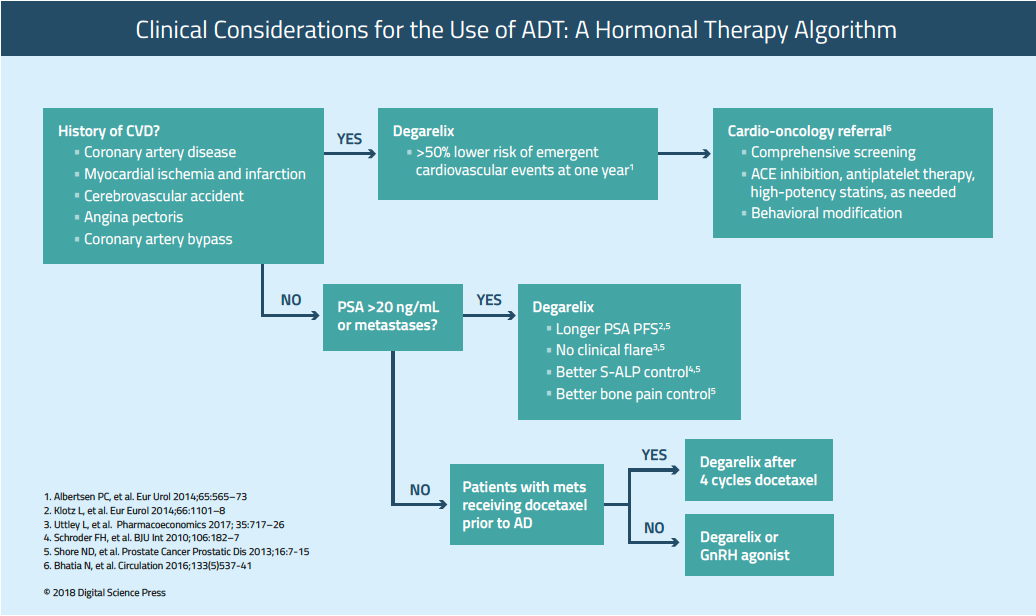
Based on these data, I am more likely to consider degarelix than GnRH agonist therapy for men with cardiovascular disease or established risk factors. In addition to its (likely) reduced cardiovascular toxicity, degarelix typically achieves castrate levels of testosterone within 72 hours, leading to faster PSA suppression without testosterone flare or microsurges.19 Additionally, GnRH antagonist therapy has been linked to improved PSA progression-free survival and less joint and musculoskeletal pain than GnRH agonist therapy.6,20,21
Several lines of evidence may help explain why degarelix appears to pose a lower cardiovascular risk than GnRH agonist therapy. First, prolonged use of GnRH agonists adversely affects multiple cardiometabolic risk factors, including glucose tolerance, low-density lipoprotein (LDL) and triglyceride levels, waist circumference, and sarcopenia.5 These changes can indirectly induce atherosclerosis and coronary artery disease. In addition, GnRH agonist therapy has been found to promote plaque rupture and thrombosis by stimulating T cell and macrophage activity.10,22,23 (In contrast, GnRH antagonists do not stimulate T cell activity.)23 Furthermore, GnRH agonists primarily suppress luteinizing hormone, while GnRH antagonists suppress both luteinizing hormone (LH) and follicle-stimulating hormone (FSH).5 Follicle stimulating hormone is highly expressed in prostatic adenocarcinoma and appears to promote both atherosclerotic plaque formation and insulin resistance in men receiving ADT.24 Finally, recent evidence indicates GnRH agonists can cause QTc interval prolongation, which might explain sporadic reports of sudden cardiac death in these patients.25
The picture becomes even more nuanced when we consider that the relative risk of various ADTs can vary by race and ethnicity. In a recent study in Taiwan, men with prostate cancer at increased risk for cardiovascular were significantly more likely to experience an ischemic cardiovascular event after orchiectomy compared with GnRH agonist therapy.26 This study was not an anomaly—a study of men with prostate cancer in China reported a similar result.28
Fortunately, a large trial is underway that may help elucidate some of these distinctions. The single-blind PRONOUNCE study (NCT02663908) is enrolling up to 900 patients with prostate cancer and established cardiovascular risk factors who are being assigned on a one-to-one basis to receive either degarelix or leuprolide for up to one year.28 The composite primary endpoint is major adverse cardiovascular events, while secondary endpoints include time to myocardial infarction, stroke, unstable angina requiring hospitalization, cardiovascular death, and all-cause mortality. Patients with advanced prostate cancer and established cardiovascular disease are potentially eligible to enroll if they have no 30-day history of acute cardiovascular disease and have received no hormonal therapy in the past year. The results of this trial could substantially expand our understanding of the cardiovascular risks of ADT. I encourage participation.
When considering risk, it is also important to note that the metabolic effects of ADT differ somewhat from the “classic” metabolic syndrome.29 For example, ADT is associated with increased adiponectin and normal C-reactive protein levels, while the opposite occurs in the metabolic syndrome.29 Also, unlike metabolic syndrome, prolonged ADT increases both low and high-density lipoprotein (HDL) levels and both subcutaneous and visceral abdominal fat.29,30 In a widely cited prospective observational study, men with prostate cancer who received ADT typically experienced a 22% increase in visceral abdominal fat, a 13% increase in subcutaneous abdominal fat, and a 12% increase in insulin resistance.30 The authors hypothesized that insulin resistance might result from visceral fat accumulation, rather than sex hormone deficiency.30.
As our options for GnRH antagonism expand, we will need to continue to ascertain their relative safety. For example, the phase 3 HERO study (NCT03085095) is comparing the investigational oral GnRH antagonist relugolix with leuprolide in men with advanced prostate cancer. Topline results are expected in 2019 and I particularly await the safety results of this trial.
Screening and the ABDCEs of risk management
Based on these data, it is clear that risk management is of primary importance when administering ADT. We need robust, multifaceted strategies to address the diverse cardiovascular and closely linked metabolic risks of these treatments.
The American Heart Association, the American Cancer Society, the American Urological Association, and the American Society for Radiation Oncology have published detailed recommendations on assessing and managing cardiovascular risks in men being considered for ADT.31 Before starting ADT, patients should be evaluated for pre-existing cardiovascular disease and for untreated or undertreated metabolic risk factors.5,31A complete history and physical exam should evaluate patients for current or historical angina, congestive heart failure, valvular disease, arrhythmias, and hypertension.5 Patients with established or suspected cardiovascular disease should be referred to a cardio-oncologist or cardiologist.
All patients should have a baseline blood pressure, lipid and metabolic panel, HbA1c, and electrocardiogram. 5,31 Patients with signs of congestive heart failure or structural heart disease should have a follow-up echocardiogram.5 I recommend follow-up screening every 3 months, which should include, at a minimum, a metabolic profile, lipid panel, and blood pressure.31 Regular follow-up monitoring is especially important because patients with pre-existing cardiovascular disease are at greatest risk of cardiovascular events during the first 6 months of ADT.32
In addition to publishing the AHA/ACS/AUA guidelines, experts have tailored the ABCDE paradigm to specifically address ADT.5 Initially developed for survivors of breast cancer, the ABCDE acronym stands for awareness and aspirin, blood pressure, cholesterol, and cigarettes, diabetes, diet, and exercise.5,33
In terms of awareness, patients should be educated to watch for chest pain or discomfort, shortness of breath on exertion, fatigue, nausea, sweating, light-headedness, headache, and sudden onset of chest discomfort or pain that may radiate to the neck and jaw. Limited data indicate that daily aspirin may decrease prostate cancer-specific mortality.5
For managing blood pressure, angiotensin converting enzyme inhibitors may be particularly helpful. I recommend a cardio-oncology consult for patients with pre-existing hypertension, especially if it is not well controlled (a common treatment goal is less than 140/90 mm Hg). For cholesterol, consider cardiology consult for high-intensity statin therapy, especially if patients with hyperlipidemia also have established cardiovascular disease or diabetes.5 In terms of cigarettes, smoking independently increases the risk of death in patients with prostate cancer, and they should be counseled to completely avoid tobacco products and referred for smoking cessation treatment whenever possible.5
In terms of diabetes and diet, ADT can worsen glycemic control, making it important to monitor blood glucose regularly and adjust diabetes therapies as needed. I counsel patients that ADT often leads to weight gain and that their diet should emphasize vegetables, fruits, lean protein, and whole grains. Evidence supports this approach: In a small, single-blind, randomized controlled pilot trial of men receiving ADT for prostate cancer, a 12-week intervention consisting of improved diet and group-based cognitive behavioral therapy led to significant improvements in muscle strength, body composition, and mobility.34
Exercise is one of the most important ways to mitigate the cardiovascular and metabolic risks of ADT. For example, resistance exercise can prevent and even reverse adiposity in these patients. In a year-long multicenter analysis of men starting ADT in the RADAR trial (NCT00193856), early initiation of exercise helped preserve body mass index, lean body mass, bone mineral density, fat mass, and cholesterol.35 In contrast, the control group showed increased adiposity, sarcopenia, dyslipidemia, and bone loss.35 In a single-center study, men receiving ADT who exercised 3 times. weekly for 12 weeks lost an average of 2 cm in waist circumference, while non-exercising controls gained an average of 0.7 cm.36 Notably, none of the exercises developed metabolic syndrome, compared with 8% of controls.36 In a third study of men receiving ADT, 12 weeks of resistance training improved lean muscle mass, body fat percentage, and prostate cancer-specific quality of life but did not significantly reduce the risk of metabolic syndrome over this short time period.37 Data from other controlled studies indicate that resistance exercise improves quality of life and reduces cancer-related fatigue in advanced prostate cancer.38
We can expect more robust data on how to mitigate the cardiovascular risks of ADT from the RADICAL-PC trial (Role of Androgen Deprivation Therapy in Cardiovascular Disease – A Longitudinal Prostate Cancer Study). This study seeks to ascertain risk factors for ADT-emergent cardiovascular disease by following men with newly diagnosed prostate cancer or who are being prescribed ADT for the first time.39 Embedded within this study is RADICAL PC2 (NCT03127631), a randomized, controlled trial that is comparing usual care with an intervention consisting of behavioral modifications (nutritional advice, exercise, and smoking cessation), as-needed antiplatelet therapy, statin therapy, and ACE inhibitor therapy.39 RADICAL PC2 continues to recruit patients, and primary results are expected in 2020. If the RADICAL PC2 intervention is found to negate the cardiovascular risks of GnRH agonist therapy, that would potentially give our patients with prostate cancer and cardiovascular risk factors more options for ADT.
Behavioral and pharmacologic risk management is doubly important because the second-line ADT agents abiraterone acetate and enzalutamide both show cardiovascular safety signals.40 Abiraterone can cause mineralocorticoid excess, which in turn can induce or exacerbate hypertension, hypokalemia, and fluid retention. In a prospective study of patients with metastatic, castration-resistant prostate cancer who also had risk factors for coronary artery disease, 6% of patients developed hypertension after starting on abiraterone, and 30% of patients experienced worsening of pre-existing hypertension.41 Enzalutamide also has been associated with hypertension, and a meta-analysis of more than 8,000 men receiving either abiraterone or enzalutamide reported an 84% increase in the risk of high-grade cardiac toxicity and a more than two-fold increase in the risk of high-grade hypertension. 42 We need more data on the cardiovascular safety of these therapies, but for now, we should assume that they pose a cardiovascular risk and pursue baseline and follow-up monitoring, cardio-oncology referrals, and behavioral risk modifications.
Sequencing
Just three years ago, ADT alone – whether with a GnRH agonist, a GnRH antagonist, or both – was the standard of care for metastatic hormone-sensitive prostate cancer, with docetaxel added after disease became castration-resistant. That changed in 2015, when upfront docetaxel plus ADT was found to significantly extend overall survival by a median of 13.6 months in the CHAARTED trial (NCT00309985) and by a median of 15 months in the STAMPEDE trial (NCT00268476).43,44 In 2017, additional results from the STAMPEDE study and results from the LATITUDE trial (NCT01715285) showed that upfront combination therapy with ADT and abiraterone (plus prednisone) also significantly improved overall survival and radiographic progression-free survival compared with ADT alone in men with hormone-sensitive. metastatic prostate cancer.45,46 Enzalutamide is also under priority FDA review for approval in combination with ADT for men with M0 castration-resistant disease and rapidly rising PSA levels. In the pivotal phase 3 PROSPER trial, these patients had a median metastasis-free survival of 36.6 months with enzalutamide plus ADT, versus 14.7 months with ADT plus placebo.47
The results of these studies are practice-changing,48 but questions remain about sequencing. Most of our patients with advanced prostate cancer will eventually receive both docetaxel and a second-line ADT agent during their disease course. In the STAMPEDE trial, after a median follow-up time of 4 years, abiraterone-ADT versus docetaxel-ADT showed no significant differences in median overall survival, metastasis-free survival, prostate-cancer-specific survival, or rates of symptomatic skeletal events.49 Therefore, the question is not so much which treatment to use, but which to use first.
Unfortunately, STAMPEDE and LATITUDE did not compare different sequences of docetaxel and abiraterone. Physicians might be tempted to use abiraterone first to spare patients the toxicities of chemotherapy. However, this is not necessarily the best choice. Patients who are relatively strong, with good performance status , may better be able to tolerate docetaxel upfront, and data suggest that this sequence can help maximize docetaxel’s benefits. Because of differences in hepatic uptake, castrated men with prostate cancer have been shown to clear docetaxel about twice as rapidly as uncastrated patients.50 Thus, by delaying docetaxel until patients become castration-resistant, we can inadvertently weaken treatment response. As long as docetaxel is part of our prostate cancer armamentarium, we need to consider when to use it relative to ADT.
Fortunately, an ongoing phase 2 study (NCT03069937) should help inform this issue. In this trial, men with metastatic, hormone-sensitive prostate cancer are receiving four cycles of docetaxel, followed by two cycles of docetaxel plus degarelix, followed by five additional doses of degarelix (once every 28 days). If readouts are positive, we can expect a large phase 3 follow-up study. Another question is when and whether to consider upfront triple-combination therapy with ADT, abiraterone, docetaxel. The ongoing phase 3 PEACE1 trial (NCT01957436) is evaluating this regimen in men with metastatic hormone-sensitive prostate. cancer. Primary results are expected in 2019. Other trials, such as ARCHES (NCT02677896), ENZAMET (NCT02446405), and STAMPEDE arm J, also are comparing the efficacy of ADT, docetaxel, and one or more second-line ADT agents with either ADT plus docetaxel or second-line ADT monotherapy. The results of these studies should help us determine the best treatment sequences for our patients with advanced prostate cancer.
In the near future, genomic profiling will probably help us better individual patient treatment selections. Demographics are also an important consideration. At ASCO 2018, an analysis of the Abi Race trial (NCT01940276) showed that abiraterone induced deeper PSA responses in black men compared with white men.51 Median time to PSA progression was 16.6 months versus 11.5 months, respectively.51 Adverse events, including hypertension, were mostly comparable between groups, but white men had a higher rate of fatigue (40% versus 26% for black men) and black men had a higher rate of hypokalemia (36% versus 18% for white men).51
Such findings underscore the need for diversity when enrolling patients in clinical trials, particularly because we now have powerful tools to assess the genetics of risk at a granular level. For now, I recommend carefully considering each patient’s fitness, comorbidities, tumor characteristics, and expected disease trajectory.
SUMMARY
Androgen deprivation therapy remains foundational in the treatment of advanced prostate cancer. Hormone suppression is associated with a variety of important adverse effects, of which cardiovascular and metabolic complications especially overlap. Multiple studies indicate that GnRH agonists may increase the risk of cardiovascular disease and major adverse cardiovascular events more than GnRH antagonists. In addition, degarelix is associated with faster testosterone suppression without flare and longer PSA-free survival. Pending the results of the PRONOUNCE study, I consider degarelix instead of GnRH agonist therapy for men with a history of cardiovascular disease or a PSA level exceeding 20 ng/mL or metastases. Baseline and regular follow- up monitoring should ascertain cardiovascular and metabolic risk factors and changes. Emerging data indicate that multifaceted behavioral interventions can help positively modify cardiovascular and metabolic risk, although we await results from the RADICALPC2 trial to help quantify their impact. As new therapies for advanced prostate cancer shift toward earlier-stage treatment, we must carefully consider how best to sequence and combine ADT, second-line and next-generation ADT, docetaxel, and other therapies. A tailored, individualized approach should account for patients’ fitness, disease characteristics, and comorbidities. Genomic tools may soon help us personalize treatment and sequencing to optimize both efficacy and safety.
References
1. Global Burden of Disease Cancer Collaboration, Fitzmaurice C, Akinyemiju TF, et al. Global regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: a systematic analysis for the Global Burden of Disease Study. JAMA Oncol. 2018 Jun 2. doi: 10.1001/jamaoncol.2018.2706. [Epub ahead of print]
2. Centers for Disease Control and Prevention. United States cancer statistics: data visualizations; prostate cancer. Available at: https://gis.cdc.gov/Cancer/USCS/DataViz.html Accessed June 28, 2018.
3. Zajdlewicz L, Hyde MK, Lepore SJ, et al. Health-related quality of life after the diagnosis of locally advanced or advanced prostate cancer: a longitudinal study. Cancer Nurs 2017 Sep/ Oct;40(5):412-419.
4. Huggins C, Hodges CV. Studies on prostatic cancer I. The effect of castration, estrogen, and of androgen injection on serum phosphatases in metastatic carcinoma of the prostate. Cancer Res 1941;1:293-297.
5. Bhatia N, Santos M, Jones LW, et al. Cardiovascular effects of androgen deprivation therapy for the treatment of prostate cancer: ABCDE steps to reduce cardiovascular disease in patients with prostate cancer. Circulation 2016 Feb; 133(5): 537-541.
6. Shore ND, Abrahamsson PA, Anderson J, et al. New considerations for ADT in advanced prostate cancer and the emerging role of GnRH antagonists. Prostate Cancer Prostatic Dis 2013 Mar;16(1):7-15.
7. Choi S, Lee AK. Efficacy and safety of gonadotropin-releasing hormone agonists used in the treatment of prostate cancer. Drug Healthc Patient Saf 2011; 3:107-119.
8. Chowdhury S, Robinson D, Cahill D, et al. Causes of death in men with prostate cancer: an analysis of 50,000 men from the Thames Cancer Registry. BJU Int 2013 Jul;112(2):182-189.
9. Byar DP, Corle DK. Hormone therapy for prostate cancer: results of the Veterans Administration Cooperative Urological Research Group studies. NCI Monogr 1988;(7):165-170.
10. Zareba P, Duivenvoorden W, Leong DP, et al. Androgen deprivation therapy and cardiovascular disease: what is the linking mechanism? Ther Adv Urol 2016 Apr;8(2):118-129.
11. Greiman AK, Keane TE. Approach to androgen deprivation in the prostate cancer patient with pre-existing cardiovascular disease. Curr Urol Rep 2017 Jun;18(6):41.
12. Gandaglia G, Sun M, Popa I, et al. The impact of androgen-deprivation therapy (ADT) on the risk of cardiovascular (CV) events in patients with non-metastatic prostate cancer: a population-based study. BJU Int 2014 Dec;114(6b):E82-E89.
13. Zhao J, Zhu S, Sun L, et al. Androgen deprivation therapy for prostate cancer is associated with cardiovascular morbidity and mortality: a meta-analysis of population-based observational studies. PLoS One 2014 Sep 29;9(9):e107516.
14. Thomsen FB, Sandin F, Garmo H, et al. Gonadotropin-releasing hormone agonists, orchiectomy, and risk of cardiovascular disease: semi-ecologic, nationwide, population-based study. Eur Urol 2017 Dec;72(6):920-928.
15. Clinton TN, Woldu SL, Raj GV. Degarelix versus luteinizing hormone-releasing hormone agonists for the treatment of prostate cancer. Expert Opin Pharmacother 2017 Jun;18(8):825-832.
16. Margel D, Pe’er A, Ber Y, et al. MP52-17 cardiovascular events and biomarkers in a randomized trial comparing lhrh agonist and antagonist among patients with advanced prostate cancer. J Urol 2018 Apr;199(4):suppl p. e702.
17. Albertsen PC, Klotz L, Tombal B, et al. Cardiovascular morbidity associated with gonadotropin releasing hormone agonists and an antagonist. Eur Urol 2014 Mar;65(3):565-573.
18. Scailteux LM, Vincendeau S, Balusson F, et al. Androgen deprivation therapy and cardiovascular risk: no meaningful difference between GnRH antagonist and agonists-a nationwide population- based cohort study based on 2010-2013 French Health Insurance data. Eur J Cancer 2017 May;77:99-108.
19. Rick FG, Block NL , Schally AV. An update on the use of degarelix in the treatment of advanced hormone-dependent prostate cancer. Onco Targets Ther 2013; 6: 391-402.NL ,Rick FG, Block NL , Schally AV. An update on the use of degarelix in the treatment of advanced hormone-dependent prostate cancer. Onco Targets Ther 2013; 6: 391-402.
20. Uttley L, Whyte S, Gomersall T, et al. Degarelix for treating advanced hormone-dependent prostate cancer: an evidence review group perspective of a NICE single technology appraisal. Pharmacoeconomics. 2017 Jul;35(7):717-726.
21. Klotz L, Miller K, Crawford ED, et al. Disease control outcomes from analysis of pooled individual patient data from five comparative randomised clinical trials of degarelix versus luteinising hormone-releasing hormone agonists. Eur Urol 2014 Dec;66(6):1101-1108.
22. Libby P. Molecular and cellular mechanisms of the thrombotic complications of atherosclerosis. J Lipid Res 2009 Apr;50 Suppl:S352-S357.
23. Rosario DJ, Davey P, Green J, et al. The role of gonadotrophin-releasing hormone antagonists in the treatment of patients with advanced hormone-dependent prostate cancer in the UK. World J Urol 2016 Dec;34(12):1601-1609.
24. Crawford ED, Schally AV, Pinthus JH, et al. The potential role of follicle-stimulating hormone in the cardiovascular, metabolic, skeletal, and cognitive effects associated with androgen deprivation therapy. Urol Oncol 2017 May;35(5):183-191.
25. Gagliano-Jucá T, Travison TG, Kantoff PW, et al. Androgen deprivation therapy is associated with prolongation of QTc interval in men with prostate cancer. J Endocr Soc 2018 Apr 20;2(5):485-496.
26. Chen DY, See LC, Liu JR, et al. Risk of cardiovascular ischemic events after surgical castration and gonadotropin-releasing hormone agonist therapy for prostate cancer: a nationwide cohort study. J Clin Oncol 2017 Nov;35(32):3697-3705
27. Teoh JY, Chan SY, Chiu PK, et al. Risk of cardiovascular thrombotic events after surgical castration versus gonadotropin-releasing hormone agonists in Chinese men
28. Slovin SF, Melloni C, Mansor-Lefebvre S, et al. A multicenter, randomized, controlled trial comparing the occurrence of major adverse cardiovascular events (MACEs) in patients (pts) with prostate cancer (pc) and cardiovascular disease (CARDIOVASCULAR DISEASE) receiving degarelix (GnRH receptor antagonist) or leuprolide (GnRH receptor agonist). J Clin Oncol 2018;36(suppl 6):abstr TPS395.
29. Saylor PJ, Smith MR. Metabolic complications of androgen deprivation therapy for prostate cancer. J Urol 2009 May;181(5):1998-2006.
30. Hamilton EJ, Gianatti E, Strauss BJ, et al. Increase in visceral and subcutaneous abdominal fat in men with prostate cancer treated with androgen deprivation therapy. Clin Endocrinol (Oxf). 2011 Mar;74(3):377-383.
31. Levine GN, D’Amico AV, Berger P, et al. Androgen-deprivation therapy in prostate cancer and cardiovascular risk: a science advisory from the American Heart Association, American Cancer Society, and American Urological Association: endorsed by the American Society for Radiation Oncology. Circulation 2010 Feb 16;121(6):833-840.
32. O’Farrell S, Garmo H, Holmberg L, et al. Risk and timing of cardiovascular disease after androgen- deprivation therapy in men with prostate cancer. J Clin Oncol 2015 Apr;33(11):1243-1251.
33. Montazeri K, Unitt C, Foody JM, et al. ABCDE steps to prevent heart disease in breast cancer survivors. Circulation 2014 Oct;130(18):e157-e159.
34. Focht BC, Lucas AR, Grainger E, et al. Effects of a group-mediated exercise and dietary intervention in the treatment of prostate cancer patients undergoing androgen deprivation therapy: results from the IDEA-P trial. Ann Behav Med 2018 Apr 19;52(5):412-428.
35. Galvão DA, Spry N, Denham J, et al. A multicentre year-long randomised controlled trial of exercise training targeting physical functioning in men with prostate cancer previously treated with androgen suppression and radiation from TROG 03.04 RADAR. Eur Urol 2014 May;65(5):856-864.
36. Dorff TB, Gross ME, Quinn DI, et al. Impact of resistance exercise on metabolic syndrome (MetS) parameters in men receiving androgen deprivation therapy (ADT) for prostate cancer. J Clin Oncol. 2017;35(suppl 6):abstr 223.
37. Dawson JK, Dorff TB, Todd Schroeder E, et al. Impact of resistance training on body composition and metabolic syndrome variables during androgen deprivation therapy for prostate cancer: a pilot randomized controlled trial. BMC Cancer 2018 Apr 3;18(1):368.
38. Neefjes ECW, van den Hurk RM. Muscle mass as a target to reduce fatigue in patients with advanced cancer. J Cachexia Sarcopenia Muscle 2017 Aug;8(4):623-629.
39. Pinthus JH, Klotz L, Lukka H, et al. The RADICAL-PC trial. J Clin Oncol. 2016;34(suppl 2):abstr 178.
40. Veccia A, Maines F, Kinspergher S, et al. Cardiovascular toxicities of systemic treatments of prostate cancer. Nat Rev Urol. 2017 Jan 24;14(4):230-243.
41. Prati V, Ruatta F, Aversa C, et al. Cardiovascular safety of abiraterone acetate in metastatic castration-resistant prostate cancer patients: a prospective evaluation. Future Oncol 2018 Feb;14(5):443-448.
42. Iacovelli R, Ciccarese C, Bria E, et al. The cardiovascular toxicity of abiraterone and enzalutamide in prostate cancer. Clin Genitourin Cancer 2018 Jun;16(3):e645-e653.
43. Sweeney CJ, Chen Y-H, Carducci M, et al. Chemohormonal therapy in metastatic hormone-sensitive prostate cancer. N Engl J Med. 2015 Aug 20; 373(8):737-746.
44. James ND, Sydes MR, Clarke NW, et al. Addition of docetaxel, zoledronic acid, or both to first-line long-term hormone therapy in prostate cancer (STAMPEDE): survival results from an adaptive, multiarm, multistage, platform randomised controlled trial. Lancet 2016 Mar 19;387(10024):1163-1177.
45. James ND, de Bono JS, Spears MR, et al. Abiraterone for prostate cancer not previously treated with hormone therapy. N Engl J Med 2017 Jul 27;377(4):338-351.
46. Fizazi K, Tran N, Fein L, et al. Abiraterone plus prednisone in metastatic, castration-sensitive prostate cancer. N Engl J Med. 2017 Jul 27;377(4):352-360.
47. Hussain M, Fizazi K, Saad F, et al. Enzalutamide in men with nonmetastatic, castration-resistant prostate cancer. N Engl J Med. 2018 Jun 28;378(26):2465-2474.
48. NCCN.org. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines Ò ): Prostate Cancer. Version 3.2018- June 21, 2018. https://www.nccn.org/professionals/physician_gls/pdf/prostate. pdf Accessed June 27, 2018.
49. Sydes MR, Spears MR, Mason MD, et al. Adding abiraterone or docetaxel to long-term hormone therapy for prostate cancer: directly randomised data from the STAMPEDE multi-arm, multi-stage platform protocol. Ann Oncol. 2018 May 1;29(5):1235-1248.
50. Franke RM, Carducci MA, Rudek MA, et al. Castration-dependent pharmacokinetics of docetaxel in patients with prostate cancer. J Clin Oncol 2010 Oct;28(30):4562-4567.
51. George DJ, Heath EI, Sartor AO, et al. Abi Race: A prospective, multicenter study of black (B) and white (W) patients (pts) with metastatic castrate resistant prostate cancer (mCRPC) treated with abiraterone acetate and prednisone (AAP). Presented at: American Society of Clinical Oncology; June 1-5, 2018; Chicago, IL, USA. Abstract LBA5009.
Written by: Thomas E. Keane, MBBCh, FRCSI, FACS, is professor and chairman of the Department of Urology at the Medical University of South Carolina in Charleston. Dr. Keane specializes in managing prostate, bladder, and renal cancers. An avid researcher, Dr. Keane has served as principal investigator or co-investigator on more than 20 major clinical and preclinical studies, funded by grants from the National Institutes of Health as well as industry-funded. Much of his work focuses on innovative concepts in translational research, including utilizing human tumor xenografts to investigate the efficacy of new therapies as they relate to GU malignancies with particular reference to cytotoxic agents, sphingolipids, and boron-containing compounds. He holds a U.S. patent for sphingolipid derivatives and their use.