Magnetic resonance imaging (MRI) is sometimes being utilized in renal tumor imaging, namely when there are contraindications to contrast medium, or when the CT images are inconclusive. T1 weighted images can detect fat and hemosiderin and thus diagnose angiomyolipoma and hemorrhagic cysts, respectively. On the other hand, T2 sequence can better characterize complex cystic tumors and different types of RCC (Figure 1). Despite the high accuracy of both CT and MRI, in 10-20% of cases, the discrimination between benign and malignant renal masses is impossible. In these cases, a biopsy is recommended, if its result may alter the management.
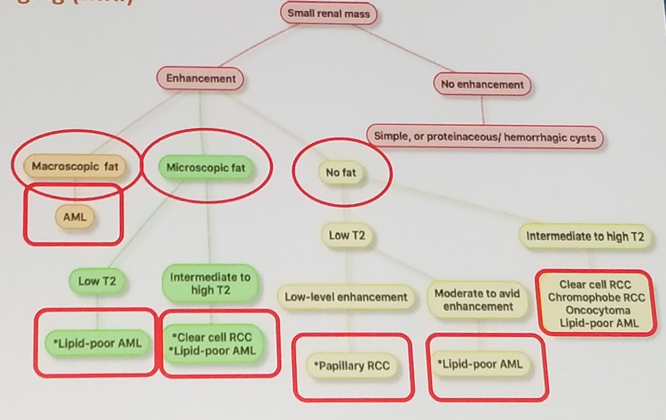
Figure 1. Proposed imaging algorithm of renal mass
Since the introduction of the R.E.N.A.L. Nephrometry Score in 2009, there have been several other scoring systems that asses tumor complexity based on anatomical features (PADUA Score, Centrality Index, Arterial-Based Complexity Score, Diameter-Axial-Polar Score, and Contact Surface Area). In general, these scoring systems have been correlated with operative and ischemia time, blood loss, urine leak, length of stay, and tumor recurrence. Additional scoring systems of non-tumor related anatomy have been studied clinically and include the Mayo Adhesive Probability (MAP) Score and the Renal Pelvis Score. These two are associated with the complexity of the procedure and perioperative outcomes. Other imaging-based adjunct tools for preoperative planning are the 3D reconstruction (from 1 mm CT angiogram slices) and virtual reality of kidney models. Lastly, a 3D model integrated into the robotic console generates a superimposed image of the tumor and blood vessels (augmented reality). In the postoperative settings following partial nephrectomy, contrast-enhanced CT can assess the functional status of the kidney. The percentage of parenchymal volume preserved after tumor resection correlated with the change in eGFR to a greater degree than merely ischemia time.
Presented by: Francesco Porpiglia, MD, Professor, Department of Urology, University of Turin, Italy
Read: State of the Art: Small Renal Masses, the Moderated Session by Jaime Landman, MD
Read: State of the Art: Small Renal Masses – Active Surveillance by David Duchene, MD
Read: State of the Art: Small Renal Masses – Latest in Partial Nephrectomy, Duke Herrell, MD
Read: State of the Art: Small Renal Masses - Office Biopsies, Can Obek, MD