Several studies have shown that AS is a safe approach. Based on the DISSRM registry, 5-year cancer-specific survival was similar between patients electing AS or intervention (99-100%). In another large series of patients on AS, 5-year cancer-specific mortality was 1.2%. The majority of small renal tumors are indolent (Figure 1) and over 75% of tumors grow at a rate of less than 5 mm per year. When a tumor is closely monitored and grows at a rate higher than expected for a benign lesion, delayed intervention is recommended.

Figure 1. correlation between tumor size and aggressive histology
In general, renal mass biopsy prior to initiating AS is recommended only if it would change management. Indolent malignant tumors such as low grade clear cell RCC, chromophobe, or papillary type I have low malignant potential and are therefore suitable for AS (Figure 2). Recommended imaging interval is 3-6 months initially. When the tumor is stable in size and there are more competing risks for death, intervals can be extended.
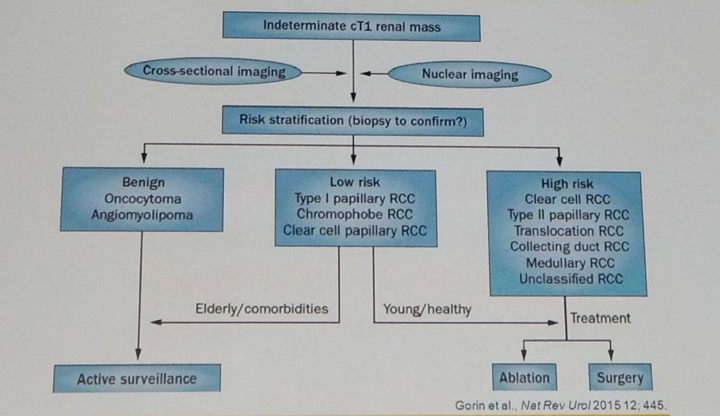
Figure 2. Proposed algorithm for active surveillance.
Presented by: David Duchene, MD, Professor, Department of Urology, University of Kansas Medical Center, USA
Written by: Shlomi Tapiero, MD, Department of Urology, University of California-Irvine, medical writer for UroToday.com at the 36th World Congress of Endourology (WCE) and SWL - September 20-23, 2018 Paris, France
Read: State of the Art: Small Renal Masses, the Moderated Session by Jaime Landman, MD
Read: State of the Art: Small Renal Masses - Imaging by Francesco Porpiglia, MD
Read: State of the Art: Small Renal Masses – Latest in Partial Nephrectomy, Duke Herrell, MD
Read: State of the Art: Small Renal Masses - Office Biopsies, Can Obek, MD