Patients with high-grade BCG-unresponsive NMIBC can experience high rates of disease progression and subsequent mortality (1). Those who refuse radical cystectomy in this setting have limited effective bladder sparing options (2). In fact, Valrubicin, is the only FDA-approved agent for patients with BCG unresponsive NMIBC. It demonstrates an 18% complete response rate at 6 months, which decreases to 10% complete response at 12 months (3).
CG0070 is an oncolytic adenovirus (4). It selectively replicates in retinoblastoma pathway defective bladder tumor cells. Adenovirus causes transgene expression of GM-CSF, which causes direct tumor lysis, immune mediated killing from GM-CSF. The current existing data demonstrate that in 2012 a phase 1 trial (4) took place, with 35 patients, showing tolerable confirmation of mechanism of action. A phase 2 study took place in 2017 and the interim analysis demonstrate a 44% complete response rate at 6 months (5), and 30% complete response rate at 12 months (6).
The aim of the discussed poster is to assess the safety and efficacy of CG0070 in patients with high risk BCG-unresponsive NMIBC who refused cystectomy. The results presented in this presentation are the final 18-months results from this phase 2 study. For the purpose of this study, high-grade NMIBC patients (Ta, T1, carcinoma in situ [CIS]) were included. All patients received induction BCG (at least 5/6 courses) and 1 maintenance (2 of 3 courses). All patients were also defined as BCG-unresponsive, which meant either BCG-refractory: failure to be disease free 6 months after BCG therapy, or BCG-relapsing: recurrence after disease free status within 24 months. Patients with over 50% of variant histology were excluded from the study.
In this trial, patients received 6-weekly instillations with induction, and 6,12, and 18 months maintenance treatments. The primary endpoints were complete response, stable disease, progressive disease, and adverse effects. The secondary endpoints included cystectomy pathology, biomarker expression (pRb, ppRB, CD8+ infiltration).
A total of 67 patients were accrued so far with 56 patients having evaluable results at 18 months follow-up. Median age was 72, with males consisting of 81% of the patients. A total of 92% of the patients completed maintenance. The overall complete response rate was 21%. Figure 1 demonstrates the rate of complete response stratified according to pathologic features. 32% of the patients had refractory disease, and 17% had relapsing disease.
Figure 1: Complete response rate stratified according to pathologic features:
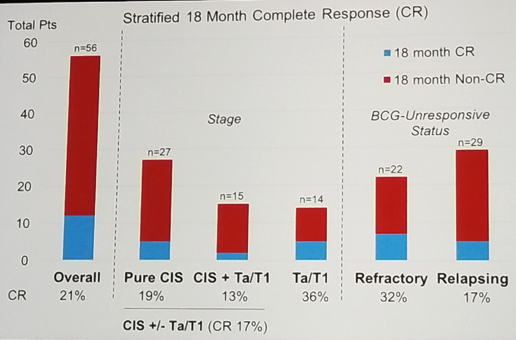
Overall, 92% of the patients reported at least one adverse event during the study. A total of 59 grade 1, 25 grade 2, and 3 grade 3 adverse events were reported. The most common adverse events were genitourinary with bladder spasms, hematuria, and dysuria being most prevalent. Additionally, Influenza-type illness was common (7%), fatigue (4%), and chills (1%).
A total of 10 patients underwent radical cystectomy due to stable/progressive disease, and 6 patients had muscle invasive disease. Six patients had non-treatment related deaths.
The limitations of the study include a heterogenous population with no control arm. The biomarker data with correlation to the clinical response is still pending.
In conclusion, CG0070 adenovirus demonstrates a 21% complete response rate in a NMIBC BCG-unresponsive population after 18 months. 17% and 32% complete response rate was shown in CIS tumors, and BCG-refractory tumors, respectively. The drug related adverse events demonstrate a Clavien grade 3 complication rate of 4.5%. This novel treatment for the NMIBC BCG-unresponsive patients shows considerable promise.
Presented By: Vignesh T. Packiam, Mayo Clinic, Rochester, MN
References:
Hall et al. J Urol 2007
Witjies et al. Eur Urol 2006
Steinberg et al J Urol 2000
Burke et al. J Urol 2012
Packiam et al. Urol Onc 2017
Abstract AUA 2018
Written by: Hanan Goldberg, MD, Urologic Oncology Fellow, SUO, University of Toronto, Princess Margaret Cancer Centre, @GoldbergHanan, at the 19th Annual Meeting of the Society of Urologic Oncology (SUO), November 28-30, 2018 – Phoenix, Arizona