The enhanced recovery after surgery (ERAS) is an evidence-based multimodal approach focused on peri-operative period. It was first introduced in 1990, and championed by colorectal surgeons, the objectives of ERAS are: Improve physiologic and psychological response, enable discharge home earlier, enhance safety and well-being. Several meta-analyses have shown accelerated recovery and decreased hospital stay with ERAS in colorectal surgery.
As preparation for surgery, Dr. Kamat emphasized a preoperative enhanced recovery framework: Optimization of medical co-morbidities, smoking cessation, nutrition assessment (even short-term dietary modification and decrease alcohol intake) and prehabilitation (Physical conditioning). Assuring the mentioned framework is done, it´s helpful to give the patient a written leaflet describing what will happen during surgery, what they should expect and their role in the preparation and in the recovery process.
About the intra-operative enhanced recovery framework, we must pay special attention in making the surgery efficient and expeditious (less than 4 and 5 hours in open surgery and robotic surgery respectively is recommended), making smaller incisions, diminishing bowel manipulation, minimizing blood loss and transfusion, the use of non-narcotic analgesia during surgery and local instillation of local anesthetic at incision sites.
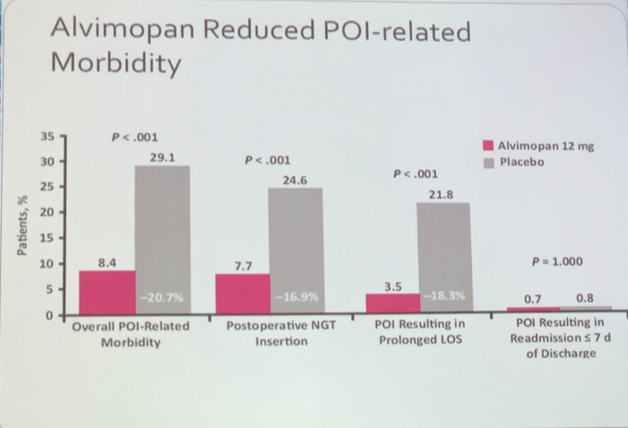
The gastrointestinal (GI) recovery is an important factor for length of stay and readmission since delayed GI recovery (ileus) is the most common cause for a prolonged hospital stay. Post-operative ileus (POI) is related to increased risk of secondary clinical consequences (Nosocomial infections and readmissions). Having said this, we should avoid intense bowel preparation, avoid nasogastric tubes (NGT), give pharmacological prophylaxis for postoperative nausea or vomiting, enforce early enteral feeding diet on the first postoperative day, the liberal usage of laxatives and Alvimopan. The Alvimopan has shown efficacy in phase 4 randomized, double bind, placebo-controlled study, reducing POI from rates of 29% to 8.4%, post-operative NGT insertion from 24.4% to 7.7% and POI resulting in long inpatient stay from 21.8% to 3.5%, this without change in readmission rates (Fig 1).
The ERAS protocol has reduced the intrahospital stay after laparoscopic or robotic Cystectomy with a median of 4 days in contrast to 10 days with traditional care (Fig 2). The quality of life also improves, with better wound cicatrization, fewer analgesics demand and the time spent at intermediate care unit is significantly shorter, and all of this comes with saving up to $10,000 dls per patient.

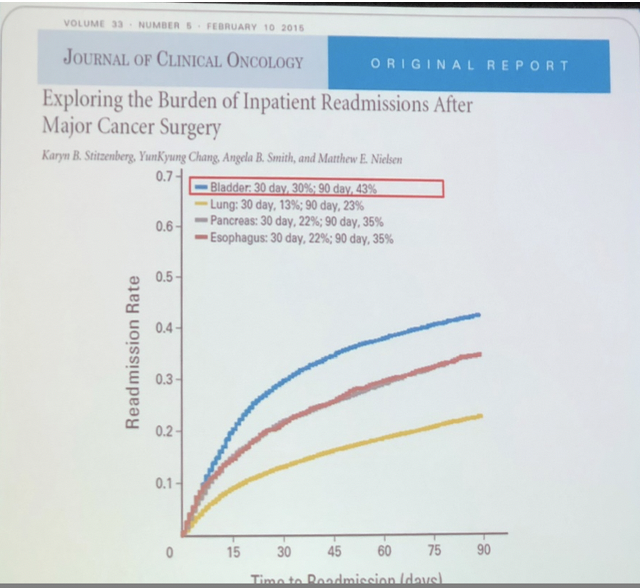
The readmission rate after radical cystectomy continues to be one of the highest readmission rates of any surgery, with up to 25%. It is higher than pancreatic or thoracic surgery (Fig 3). The most important causes of readmission are infections, failure to thrive, urinary complications, GI complications, hematologic and metabolic complications. In order to prevent readmission, we need to focus on the first few weeks after discharge, it´s well known that early follow-up may reduce readmission in a rate of 20%, and it´s important to improve the communication with our patients (early and frequent phone calls, telemedicine, mobile Apps, etc.)
Kamat concluded his talk with some take-home messages:
-The ERAS framework begins prior to the actual admission.
-Identify and treat comorbidities.
-Improve physical conditioning and carbohydrate loading.
-GI optimization avoiding bowel preparation, minimize handling intra-operative, and no NGT
-Reduce the effects of opioids with Alvimopan prior surgery, non-narcotic therapy intra-operative and usage of long-acting local anesthetic
-There are some surgeons facts: Expeditious surgery and minimize blood loss
-Early mobilization
-Don´t tempt readmission fate
-Early detection, screening, and prevention. Regarding the two first weeks after discharge are critical
Presented by: Ashish M. Kamat, MD, Professor of Urologic Oncology, MD Anderson Cancer Center, Houston, TX
Written by: Ashmar Gómez Conzatti, MD, Urology Resident, Instituto Nacional de Ciencias Médicas y Nutrición “Salvador Zubirán”, Mexico City and Ashish M. Kamat, MD, Professor of Urologic Oncology, MD Anderson Cancer Center, Houston, TX at the 2018 Congreso de la Asociación Mexicana de Urología Oncológica – July 25-28, 2018, Acapulco, GRO México