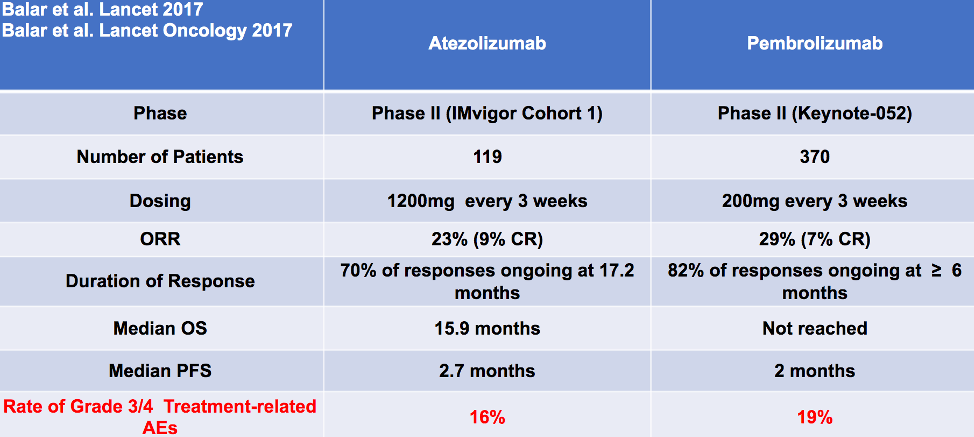
Both atezolizumab and pembrolizumab have been approved as immune checkpoint inhibitors in the first-line, cisplatin-ineligible setting, as summarized in the following table from Dr. Grivas:
In addition to the aforementioned Phase II data, there is now a plethora of immunotherapy doublet versus chemotherapy data as first-line treatment for patients with advanced urothelial carcinoma. This includes the DANUBE trial that was recently presented at the ESMO 2020 meeting testing durvalumab versus durvalumab plus tremelimumab versus chemotherapy, with primary endpoints of progression-free survival (PFS) and overall survival (OS) for the durvalumab plus tremelimumab combination versus standard of care. Unfortunately, this trial did not meet its primary endpoint.
A second trial, which is ongoing, is the CheckMate 901 trial assessing ipilimumab plus nivolumab versus chemotherapy, with primary endpoints of PFS and OS in cisplatin-ineligible patients. Secondary endpoints include PFS and OS in all patients, as well as EORTC QLC-C30 quality of life data. The following demonstrates both these trial’s design:
Additional trials in this disease space assessing immune checkpoint inhibitors as first-line treatment in advanced urothelial carcinoma including the KEYNOTE-361 trial assessing pembrolizumab versus pembrolizumab plus chemotherapy versus chemotherapy alone. Unfortunately, in preliminary data presented at ESMO 2020, the KEYNOTE-361 trial did not meet its primary endpoint, thus there is no utility to treating patients with pembrolizumab plus chemotherapy in the front-line setting. Another trial in this disease space is the IMvigor-130 trial assessing atezolizumab versus atezolizumab plus chemotherapy versus chemotherapy alone: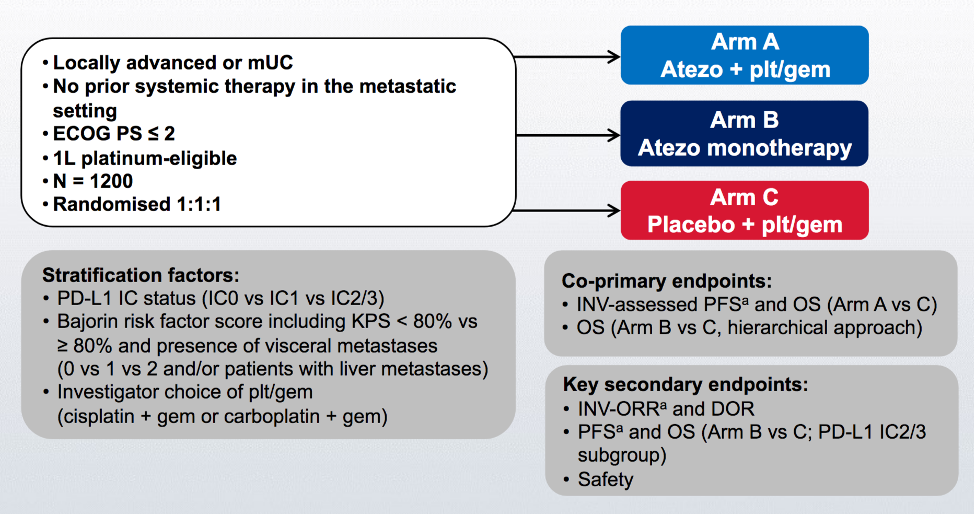
The final PFS in the intention to treat analysis of Arm A vs Arm C showed that atezolizumab plus chemotherapy improved PFS (median 8.2 months, 95% confidence interval [CI] 6.5-8.3) compared to placebo plus chemotherapy (median 6.3 months, 95% CI 6.2-7.0; hazard ratio [HR] 0.82, 95% CI 0.70-0.96):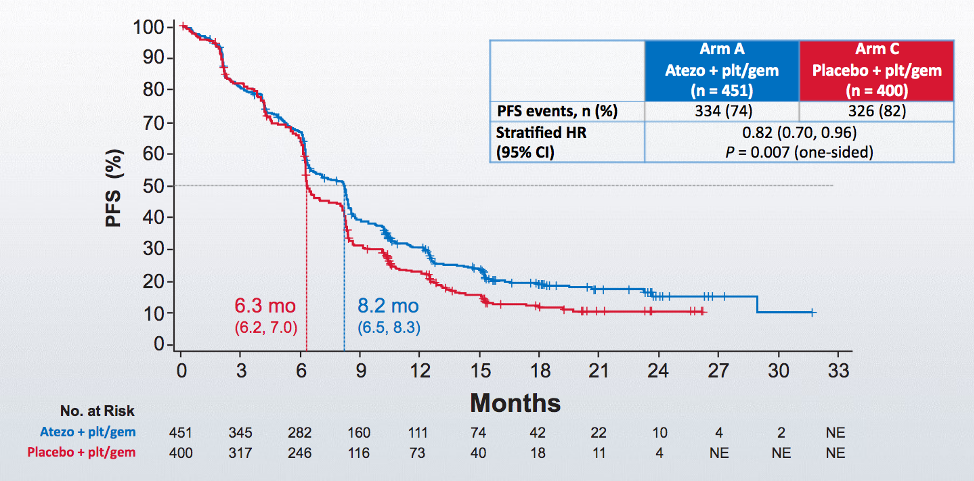
Unfortunately, there was no OS benefit in the combination of atezolizumab plus chemotherapy versus placebo versus chemotherapy group at the time of the intention to treat analysis (HR 0.83, 95% CI 0.69-1.00).
Dr. Grivas then presented data from the JAVELIN Bladder 100, which was previously presented by Dr. Powles at the ESMO 2020 annual meeting: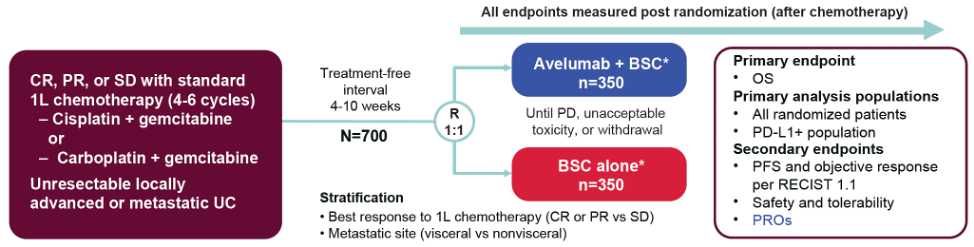
The Phase III JAVELIN Bladder 100 trial tested avelumab (anti–PD-L1) first-line maintenance plus best supportive care versus best supportive care alone.1 The study met its primary endpoint of overall survival benefit with avelumab maintenance therapy, with a median overall survival of 21.4 months versus 14.3 months in the supportive care arm, with a hazard ratio for death with avelumab of 0.69 (95% CI 0.56-0.86). At 12-months, 71% of patients in the avelumab maintenance arm were alive relative to 58% of patients in the supportive care arm. A similar result was observed for survival in the PD-L1+ population (HR 0.56, 95% CI 0.40-0.79). Furthermore, using subgroup analysis, the benefit was consistent across the subgroups. Treatment-emergent adverse events that led to discontinuation of avelumab was 11.9%, whereas death attributed by the investigator to study treatment toxicity was present in 0.6% of patients in the avelumab plus best standard of care arm, including one patient due to sepsis in cycle 10 and one patient with ischemic stroke 100 days after a single dose of avelumab. Importantly, the FDA nearly immediately granted approval for patients to receive avelumab as maintenance therapy after the publication of the manuscript.
For patients that progressed on first-line platinum chemotherapy, there are now five approved agents in the second-line setting, including atezolizumab, nivolumab, pembrolizumab, avelumab, and durvalumab:
Looking at these trials in more detail, Dr. Grivas notes that it is important to consider the grade 3/4 treatment-related adverse event profile, which varies from 8-20%, with the highest adverse events seen in the atezolizumab trial.
However, according to Dr. Grivas, there remains an unmet need:
- There are a lot of complex decisions that need to be made
- It is important to review the findings of these patients (ie. imaging, pathology, cystoscopy, clinical factors, labs, etc)
- Clinicians must decide on surgery, radiation, systemic therapy, and the optimal sequence of therapy
- Many patients already have complex underlying medical problems besides their cancer
- There are often many providers involved in the care of just one patient
- It remains to be answered how we align the care team to provide the best treatment for a given patient
- It is important to recognize early and manage appropriately immune-related adverse events via a team approach
Dr. Grivas then discussed immune-mediated toxicities among these many available agents. With regards to ipilimumab, 60% have immune-related adverse events, including 20-30% with severe immune-related adverse events. These adverse events include rash, pruritus, diarrhea, colitis, hepatitis, hypophysitis, and thyroid abnormalities. These adverse events are typically dose-related and cumulative, with a possible incidence and severity with response. According to Dr. Grivas, skin rash is often seen in the first couple of weeks of treatment, whereas other immune-related adverse events (ie. colitis) are seen later in the treatment course.
Dr. Grivas also provided the following general observations:
- Anti-PD1/PDL1 treatment is better tolerated than anti-CTLA4 agents
- Combination therapy increases the frequency of immune-related adverse events
- The onset of immune-related adverse events is typically within 1 week to >1 year after starting immune checkpoint inhibitors
- Rarely, immune-related adverse events may occur after discontinuation of immune checkpoint inhibitor therapy
- It is common for patients to under-report their symptoms, so education is paramount
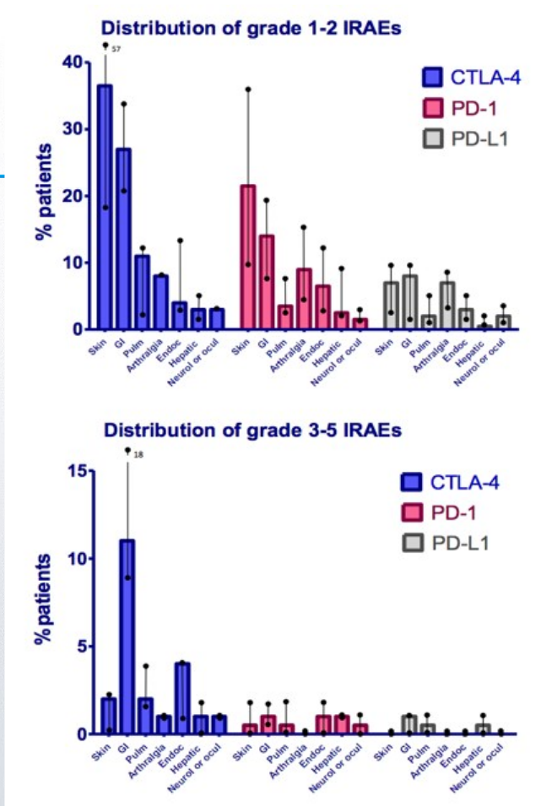
Generally, CTLA-4 inhibitors are more often associated with colitis (odds ratio [OR] 8.7, 95% CI 5.8-12.9), hypophysitis (OR 6.5, 95% CI 3.0-14.3), and rash (OR 2.0, 95% CI 1.8-2.3), whereas PD-1 therapies are more often associated with pneumonitis (OR 6.4, 95% CI 3.2-12.7), hypothyroidism (OR 4.3, 95% CI 2.9-6.3), and arthritis (OR 3.5, 95% CI 2.6-4.8). However, Dr. Grivas cautions that any agent can cause any adverse event. Importantly, there are guidelines from several governing bodies available to manage immune-related adverse events, including from ESMO, SITC, and ASCO.
Dr. Grivas notes that it is important to manage immune-related adverse events with a multidisciplinary team.2 A study from Naidoo et al. aimed to determine whether a virtual multidisciplinary immune-related toxicity team of oncology and medicine subspecialists would be feasible to implement, be used by oncology providers, and identify patients for whom multidisciplinary input is sought. In this study, 117 referrals from 102 patients were received in 8 months, all providers received recommendations within 24 hours, 100% of surveyed providers used the recommendations, and 74% changed patient management based on immune-related toxicity team recommendations. The most commonly referred toxicities were pneumonitis (23%), arthritis (16%), and dermatitis (15%); 15% of patients had multisystem toxicities. Multiple referrals were more common in those treated with combination immune checkpoint inhibitors (OR 6.0, p=0.035) or with multisystem toxicities (OR 8.1, p=0.005). The immune-related toxicity team provided a new multidisciplinary forum to assist providers in diagnosing and managing complex immune-related adverse events. Dr. Grivas wonders if this model can work across institutions with different systems and other logistical situations. Furthermore, whether this model can be “scale-able”, what may be additionally needed, and what the outcomes and patient satisfaction data reveal remains to be determined. At the University of Washington, Dr. Grivas notes the following workflow for their multidisciplinary bladder cancer clinic:
Dr. Grivas provided the following take-home messages for this high-level talk on immunotherapy in advanced bladder cancer and the management of immune-related adverse events:
- Pembrolizumab is FDA approved for Bacillus Calmette-Guérin (BCG)-unresponsive carcinoma in situ (CIS) (with or without papillary tumors) in patients who refuse or cannot get radical cystectomy, which is standard of care in this setting based on the KEYNOTE-057 trial
- Clinical trials or cisplatin-based chemotherapy for cisplatin-eligible patients is important
- Adjuvant atezolizumab did not prolong disease-free survival (DFS) versus observation
- The JAVELIN Bladder 100 trial met the primary endpoint of OS with switch maintenance avelumab plus best standard of care versus best standard of care and is anticipated to change practice after a completed response/partial response/stable disease after first-line platinum-based chemotherapy
- Atezolizumab and pembrolizumab have a similar level of evidence in first-line cisplatin-ineligible patients for PD-L1 positive or platinum-unfit patients (in the US only)
- There is level 1 evidence for pembrolizumab in the platinum-refractory setting based on the KEYNOTE-045 trial
- Immune-related adverse events can be common and cause significant morbidity and there is a need for awareness
- Data is emerging about baseline autoimmune conditions, re-challenging with immunotherapy agents after immune-related adverse events, etc.
- Remaining questions include the optimal duration of treatment, and re-challenging after complete response to progressive disease
- There is currently a great opportunity for registries, biorepositories, databases, and clinical trials
Presented by: Petros Grivas, MD, PhD, Physician, Seattle Cancer Care Alliance, Associate Professor, Division of Medical Oncology, University of Washington School of Medicine, Clinical Director, Genitourinary Cancers Program, UW Medicine, Associate Professor, Clinical Research Division, Fred Hutchinson Cancer Research Center, Seattle, Washington
Written by: Zachary Klaassen, MD, MSc, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, Augusta, Georgia, Twitter: @zklaassen_md at the 2020 Société Internationale d'Urologie Virtual Congress (#SIU2020), October 10th - October 11th, 2020
References:
1. Powles, Thomas, Se Hoon Park, Eric Voog, Claudia Caserta, Begoña P. Valderrama, Howard Gurney, Haralabos Kalofonos et al. "Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma." New England Journal of Medicine (2020).
2. Naidoo, Jarushka, Jiajia Zhang, Evan J. Lipson, Patrick M. Forde, Karthik Suresh, Kendall F. Moseley, Seema Mehta et al. "A multidisciplinary toxicity team for cancer immunotherapy–related adverse events." Journal of the National Comprehensive Cancer Network 17, no. 6 (2019): 712-720.
Related Content:
SIU Virtual Congress 2020: Background on Bladder Cancer and Introduction to Anti-PD1 Agents