- Most are high-grade and high-stage
- High recurrence in the ipsilateral kidney and ureter
- Often multifocal disease
- Low incidence of contralateral tumors
- Reduces the frequency and cost of follow-up
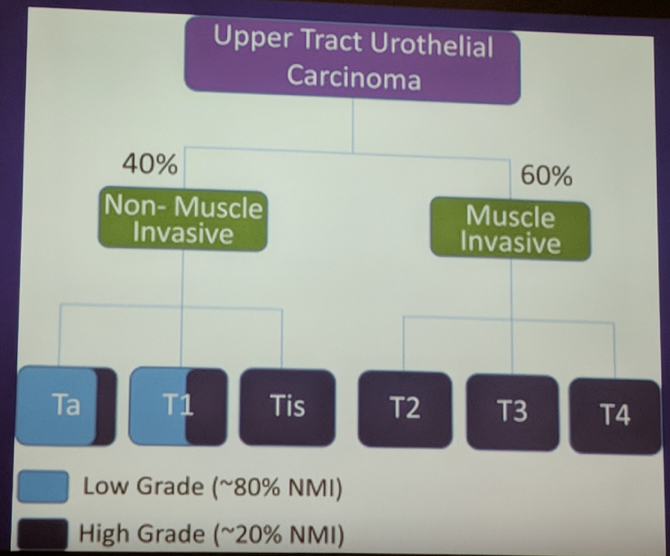
- UTUC, as mentioned in prior studies, is often an aggressive disease
However, in this very nice slide below, he highlights there is a subset of patients, particularly low-grade disease, for whom more conservative management may be appropriate:
Absolute indications for conservative management:
- Unifocal tumor
- Tumor < 1 cm
- Low-grade tumor on biopsy and cytology
- No evidence of infiltration of staging imaging
- Understands the need for close short-term and long-term follow-up and imaging
Relative indications for conservative management:
- Solitary kidney
- Bilateral synchronous tumors
- Impaired renal function
- The necessity of platinum-based chemotherapy in the future (and therefore need to preserve renal function)
Selection of the patient is the key to success! It is important to put together all the information from cytology, cystoscopy/endoscopy, biopsy and imaging to ensure you are choosing a low-risk patient. If something doesn’t quite fit with the picture, question the appropriateness of conservative management!
What are the conservative options available?
- Endoscopic – resection, fulguration
- Open/MIS
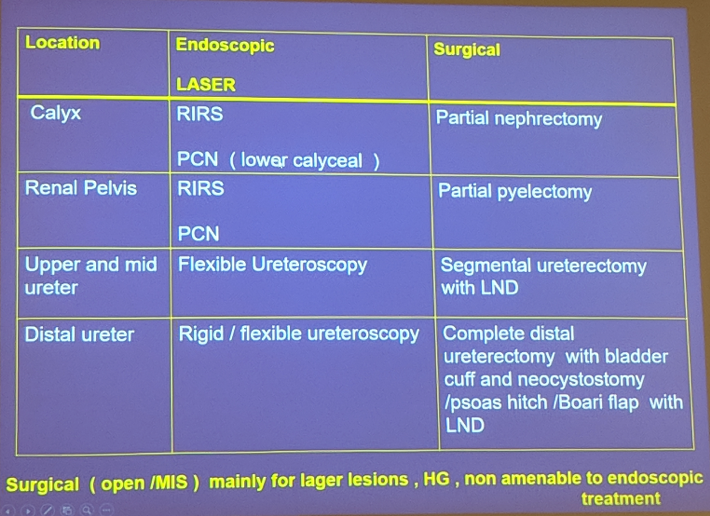
One key point he noted is that lymphadenectomy (LND) should be done if an open/MIS operation is completed.
- Provides exact staging and prognosis
- Helps direct need for adjuvant treatment
- The extent of node dissection is determined by standard templates, derived from RCC and testis literature
- The nodal tissue follows the location of the tumor
- As the tumor is further down the upper tract, the nodal packets are further down towards the pelvis
What is the role of post-operative instillation therapy?
- Different agents have been utilized: BCG, MMC, Pirarubicin
- Efficacy is mixed, but the best technique is uncertain – there is no proven benefit however
- Options include:
- Insert of a PCN and antegrade instillation (Level of evidence 3)
- Retrograde catheter instillation (better success – but the risk of retrograde pyelovenous reflux is high)
- Insertion of a double-J stent and instillation in the bladder – ineffective as the reflux rate is quite low
What is the follow-up after conservative management?
- Imaging every 3 months
- Ureteroscopy or upper tract surveillance every 3 months
- The guidelines recommend: urinary cytology and CTU at 3 and 6 months, then yearly; cysto/urs/cytology at 3 and 6 months, then every 6 months until 2 years, then annually
It is important to remember that 20% may need nephroureterectomy eventually.
He spent a little bit of time on a rare complication of UTUC conservative endoscopic management – seeding of the PCN tract. It is rare, but he brought up the concept of excising the PCN tract at the time of nephroureterectomy.
In terms of the evidence supporting conservative management, it should be noted that there are NO randomized trials in support of conservative management. However, there have been multiple systematic reviews identifying the nephron-sparing benefit and equivalent oncologic outcomes with conservative therapy.
Presented by: Makarand Khochikar, MS, DNB, Urology, FRCS, Urology Chief Uro-Oncologist at Siddhi Vinayak Ganpati Cancer Hospital, Miraj
Written By: Thenappan Chandrasekar, MD, Clinical Instructor, Thomas Jefferson University Twitter: @tchandra_uromd, @TjuUrology at the 38th Congress of the Society of International Urology - October 4- 7, 2018 - Seoul, South Korea
Further Related Content:
Is it an Aggressive Disease? - Upper Urinary Tract Transitional Cell Carcinoma
Diagnosis and Staging: The Pitfalls and the Challenges of Upper Urinary Tract Transitional Cell Carcinoma