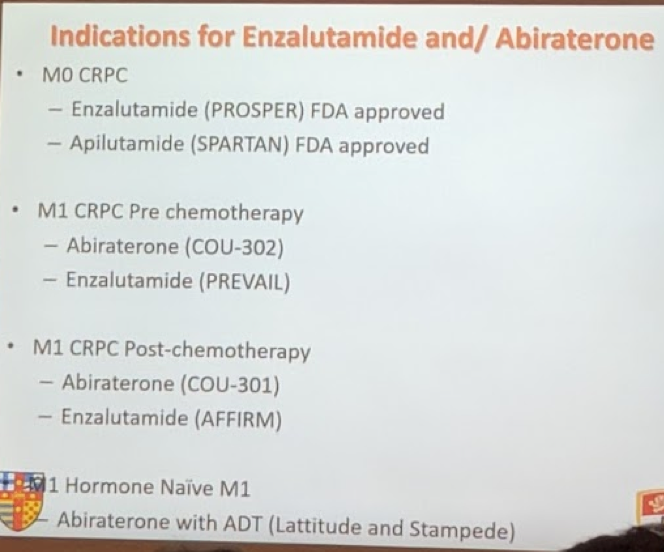
He first reviewed the two main agents in this area: enzalutamide and abiraterone. He reviewed their mechanism of action and its implication on their adverse event profile.
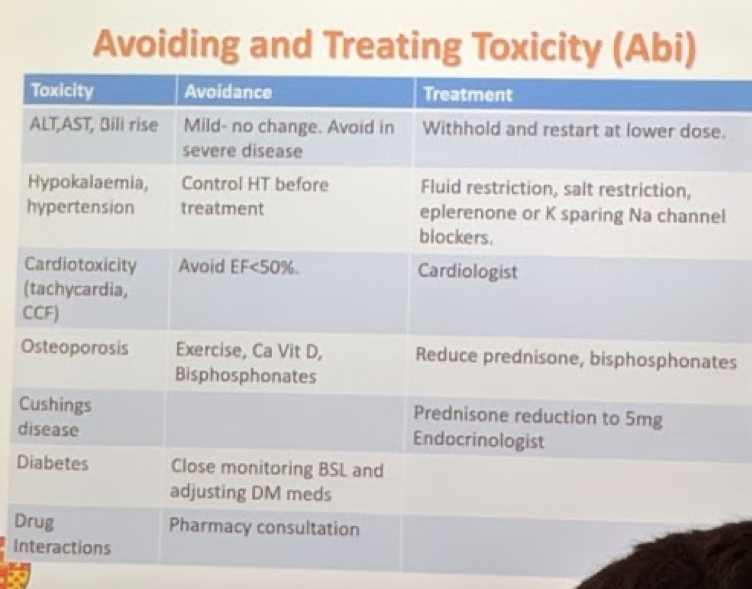
- Specifically for abiraterone, as it is an inhibitor of cyp17, it results in decreased androgen production – but also decreased cortisol production. As such, all steroid production is pushed towards the aldosterone pathway. Importantly, the loss of cortisol results in increased ACTH production – and more aldosterone production. This explains the side effects of hypokalemia, hypertension, fluid retention and renin suppression associated with abiraterone use. The co-administration of prednisone helps suppress ACTH production and replaces cortisol production.
- Enza is an advanced antiandrogen
The more important part of his talk is the practical aspect – the use of these medications in a clinical setting, what common adverse events are, how to monitor patients after starting them on these medications and how to manage adverse events.
First, we discussed abiraterone. Some practical pointers:
- Should be taken 1 hour before or 2 hours after food intake
- Give with prednisone 10 mg daily or 5 mg bid
- It is an inducer of cyp1A2 and cyp2D6, metabolized by cyp3A4 – so consult with pharmacist regarding patient’s other medications that may need dose adjustment
As for monitoring toxicity, he sees them every 2 weeks for the first 3 months, then once a month. During the visits, you need to check LFTs, BMP (and potassium specifically), evaluate for fluid retention and blood pressure.
When it comes to avoiding AE’s and responding to AE’s, here are his guidelines for abi:
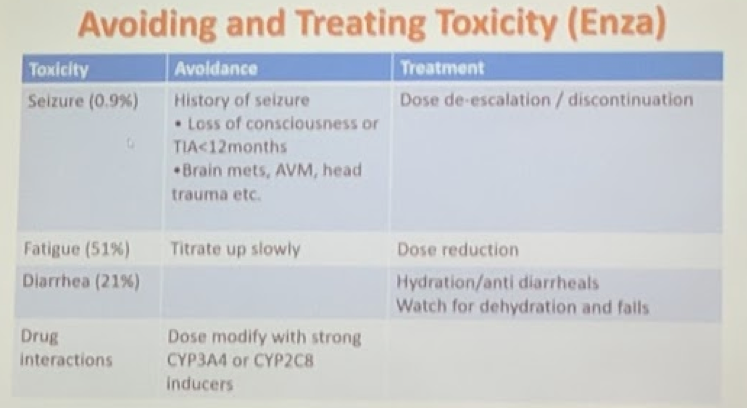
Next, he discussed enzalutamide. Enzalutamide is 4 tablets daily; no steroid co-administration required. No effect of mild/moderate renal or hepatic failure. Adverse events with enzalutamide are also very low. Fatigue is usually the most common (2-6%).
As far as monitoring goes for enza, it is a little less rigorous than abi – he sees them at 2 weeks, and then resumes regular monitoring at 3 months, 6 months, etc. The main thing to monitor is blood pressure – labwork is not required as in abiraterone management.
- However, many other practitioners will see once a month.
This was excellent practical guidance to the use of these oral agents in a urologist practice. Considering the audience was so large for an instructional course, there is clearly interest in reclaiming the management of advanced prostate cancer back to urology. However, it is important to understand how these medications work and what adverse events to monitor for!
Presented by: Manish Patel, Australia
Reference: Fizazi et al. EU 2016
Written By: Thenappan Chandrasekar, MD, Clinical Instructor, Thomas Jefferson University Twitter: @tchandra_uromd, @TjuUrology at the 38th Congress of the Society of International Urology - October 4- 7, 2018 - Seoul, South Korea