Focal therapy is defined as a treatment of a specific focus (targeted ablation) or limited defined region (quadrant ablation or hemi-ablation). In doing so, it spares at least one of two neurovascular bundles and the urethra.
Until now, there was a dichotomy in treatment options for low volume localized prostate cancer – active surveillance (good QOL, no intervention) vs. radical therapy (radical intervention, impacted QOL). Focal therapy aims to fill the void. It is ultimately based on the concept of an index lesion – if you don’t believe in that, focal therapy is not ideal treatment.
Index lesion defined as:
1) Largest volume or most aggressive tumor in the prostate
2) Defines tumor volume, p-stage and Gleason score
3) 80% of tumor volume
4) Drives cancer progression
mpMRI significantly increases the identification of significant prostate cancer. NPV is high, at least in referral centers – though this was disputed in prior presentations by members in the audience. However, the mpMRI may underestimate the true size of the lesion!
Goal of FT:
1) Optimize risk stratification at diagnosis
2) Eradicate targeted abnormalities for effective cancer control
3) Spare non-cancerous portions of the organ
4) Minimal risk to quality of life
5) Re-treat with FT if necessary
6) Salvage with radical therapy
He then reviewed the literature of focal therapy. FT was initiated with cryotherapy. However, now, we are at 7 different energy modalities. Using IDEAL stage 2b as a criteria for quality, 4 of those energy modalities have been studied adequately with 2800 patients reported in the literature.
Pretreatment considerations:
1) Age – not a barrier
2) Patient factors = very important
-LUTS – baseline symptoms
- Sexual preservation is the most important goal – baseline IIEF5
- Prostate volume – preferably <50 g
3) Disease factor
- D’Amico risk classification – typically with low and intermediate risk
- Gleason 3+4 is the sweet spot
- Cancer foci volume and %
Controversies within focal therapy
1) Predicting and localizing a unifocal lesion in a multifocal disease process
- Unifocal cancer, unilateral cancer
- Clinically significant index lesion with insignificant multifocal prostate cancer
2) Definition of effective and standard postoperative control – has not been well established yet.
3) Clinical limitations of the different modalities
4) Current evidence of efficacy
He presented a nice slide of 5 modalities, how they were tested and what their limitations were. See below.
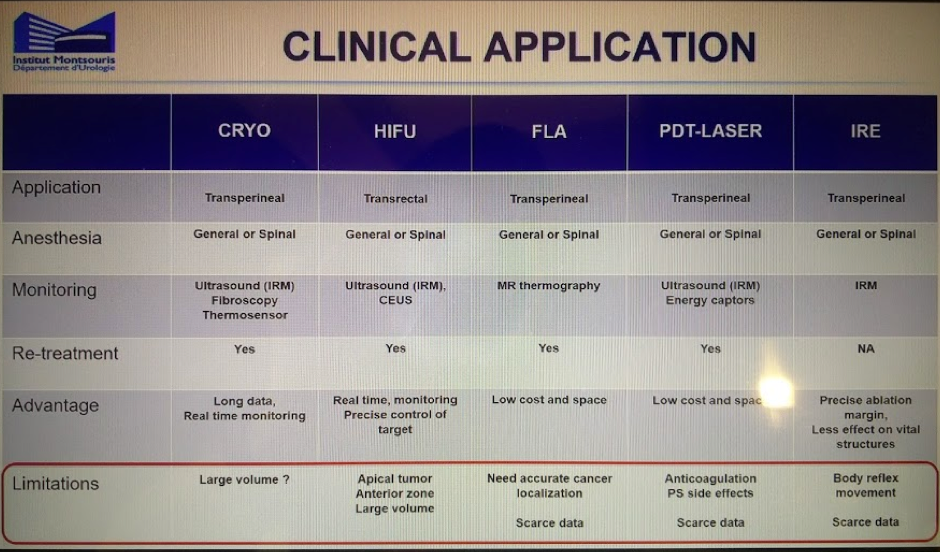
HIFU, cryotherapy, laser ablation and brachytherapy have been the most utilized energy therapies. Choosing the right energy for the right lesion is also important – each has their own limitations (including anatomic limitations).
Objectives Outcomes: All of these should be done in the early stages of this treatment
1) Post-operative imaging and biopsy is critical at this early stage
2) Imaging
- Contrast enhanced ultrasound
- MR Prostate (with DCE phase)
3) PSA kinetics
4) Control biopsy post ablation to ensure no residual disease or recurrent disease
5) Validated questionnaires for continence and sexual function
Overall, QOL impact is minimal from focal therapy. They do take an insult within the first 1-3 months, but by 3-6 months they are back to baseline.
In terms of oncologic outcomes, all studies have had limited follow-up. Oncologic success is definite as no residual significant PCa or small volumes Gleason 3+3.
- About 20% have positive biopsy within 5 years
- Retreatment is always an option
1) Oncologic
- No difference in OS, CCS (as expected over short time frame)
- No difference in BCR
2) Functional outcomes and complications
- Significantly less in focal therapy
Obviously, there is a lot of promise for focal therapy. However, long-term results need to be awaited. Defining outcomes is also important to standardize.
Presented by: Rafael Sanchez-Salas
Written by: Thenappan Chandrasekar, MD, Clinical Fellow, University of Toronto, Twitter: @tchandra_uromd at the 37th Congress of Société Internationale d’Urologie - October 19-22, 2017- Lisbon, Portugal