(UroToday.com) In one of the first sessions of the 2021 International Kidney Cancer Symposium (IKCS): North America meeting focusing on multimodality perspectives on clinical trials, Dr. Biren Sariaya presented on how we may enhance patient centered care.
He first began by defining patient-centered care, quoting Francis Peabody who said, “the secret of the care of the patient is caring for the patient”. Based on the 2001 Crossing the Quality Chasm report from the Institute of Medicine, patient centered cancer care is “respectful of and responsive to individual patient preferences, needs, and values and ensuring that patient values guide all clinical decisions”. Addressing the latter part of this, he suggested that shared decision making is the key to ensuring that patient values guide all clinical decisions. Shared decision making is premised on the collaboration between patients and their clinicians to reach an agreement about a health decision, where there are multiple medically appropriate treatment options.
He then highlighted work from Dr. Kane emphasizing that, at an interpersonal level, both physician and patient characteristics, knowledge, attitudes, skills, and emotions contribute to the communication climate and quality of communication which are key for shared decision making. Taken together, the physician and patient worldviews must come together to allow for a process that accurately affects the patient’s priorities.
This process of shared decision making can help patients evaluate options in the context of what is important to them, rather than in an agnostic climate. However, he suggested that this process starts much earlier, before the final treatment decision. He highlighted two models for communication, the ASK-TELL-ASK framework and the SPIKES framework, which emphasize the importance of understanding the patient’s story, their priorities and perspectives, and the language they use. This allows us to understand patient values and preferences. After this, we can provide medical information regarding the disease and treatment considerations before ensuring that patients have understood the information provided.

At this point, the clinician can assist the patient in evaluating treatment options based on patient goals and concerns and facilitating shared decision making implementation. In the context of oncologic communication, he emphasized the importance of informing patients about what the cancer is (the diagnosis), where the cancer is (the stage), what this means for the patient (the prognosis and treatment goals), and what we may do about it (treatment options).
Of these, he emphasized the importance of the third (prognosis) as prognostic understanding is key for patients making better decisions. A randomized intervention of early integration of palliative care with standard of care for patients with advanced lung cancer demonstrated improved overall survival in spite of less chemotherapy administered in patients who received early integration of palliative care. This, he suggested, is driven by different treatment decisions as a result of their improved understanding of the disease and its prognosis. He further emphasized that there may be a need for multi-disciplinary involvement to allow for patients to gain a better prognostic understanding.
He discussed work from the 1980s in which oncologists were typically over-optimistic about patient prognosis, both compared to the patient and other physician expectations and to lived experience. He suggested that this is likely due to the human desire for our patients to do well. Further, the introduction of immunotherapy to the treatment landscape has introduced further challenges: recent work has shown that patients with genitourinary cancers on immunotherapy often have an inaccurate prognostic understanding of their disease. As treatment options have evolved, particularly in advanced and metastatic kidney cancer, there has been increased uncertainty. Communicating this to patients is key to ensuring shared decision making.
Where there is a challenge, there is opportunity. In this context, the opportunity is for the integration of palliative care. He emphasized that palliative care is specialized medical care for people living with a serious illness. The goal here is the relief of suffering, as delivered by a multidisciplinary team. Palliative care may be delivered by the primary team (oncologists, cardiologists, etc) or by specialized professionals specifically trained in palliative care.
Given the broad potential for suffering, this addresses multiple domains of care. This may manifest with physical aspects of care (pain, nausea, vomiting), psychological aspects (anxiety and depression), social aspects (patient and family support), spiritual, religious, and existential aspects of care, cultural aspects of care, and ethical and legal aspects of care.
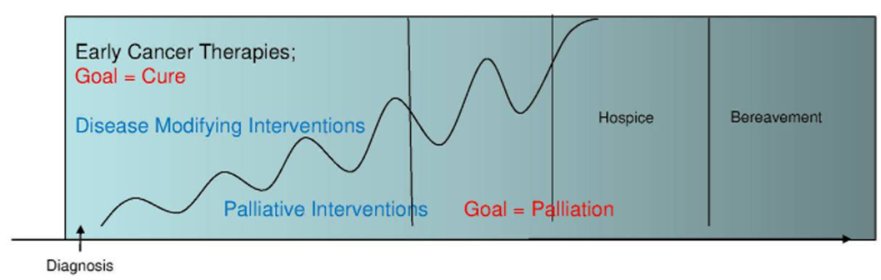
Given these varying domains, he emphasized the important role of palliative interventions across the trajectory of the disease, with differing goals and priorities based on the disease burden.
Many guidelines have advocated for the integration of palliative care in the care of patients with cancer, including in ASCO guidelines dating back as far as 2012. This is based on evidence that early integration of palliative care in routine oncologic care improves quality of life and mood, decreases the use of chemotherapy in the last month when patients accurately understood prognosis and may improve survival (based on data from patients with lung cancer). Phase III data support the role of palliative care in patients with lung cancer, gastrointestinal cancers, and others. However, there is relatively sparse data in genitourinary cancers. In mRCC, there are no published data. However, a recent analysis of NCDB suggested about 20% of patients with mRCC receive palliative care, without an increase over time.
In terms of opportunities in kidney cancer, he emphasized the importance of including patients where treatment goals are not clear. We further need work to better understand who to communicate uncertainty and better ways to offer goal directed therapies. As a pilot, he suggested a study of early integration of palliative care with the aim of assessing patient participation, quality of life, and symptoms. In an exploratory fashion, the goal of understanding the mechanism of action of palliative care is possible, examining coping mechanisms, prognostic understanding, and patient and physician emotions.
Taking the example of advanced bladder cancer with treatment options of radical cystectomy or chemoradiation, he emphasized the value of highlighting an explanation of the best-case scenario, expected outcomes, and the worst-case scenario.