(UroToday.com) In a podium presentation in the Prostate cancer IV - Advanced disease session at the 19th Meeting of the EAU Section of Oncological Urology, Dr. Cookson presented on the changing face of prostate cancer, with important implications for our practice of evidence-based medicine.
Based on his experience as co-chair of the AUA guidelines in advanced prostate cancer, Dr. Cookson highlighted both relevant guideline recommendations and the underlying data. He first began with a discussion of care for patients with metastatic hormone-sensitive prostate cancer (HSPC). Based on clinical principles, he emphasized that clinicians should assess the presence of symptoms in order to guide discussions of prognosis and further disease management as well obtain both baseline PSA testing and serials PSAs with periodic conventional imaging to longitudinally assess disease progression. Additionally, the extent of disease (including bony, nodal, and visceral metastasis) should be assessed using conventional imaging in patients who are newly diagnosed. Further, this imaging should be used to inform an assessment of the extent of disease (low- versus high-volume) using the CHAARTED criteria.
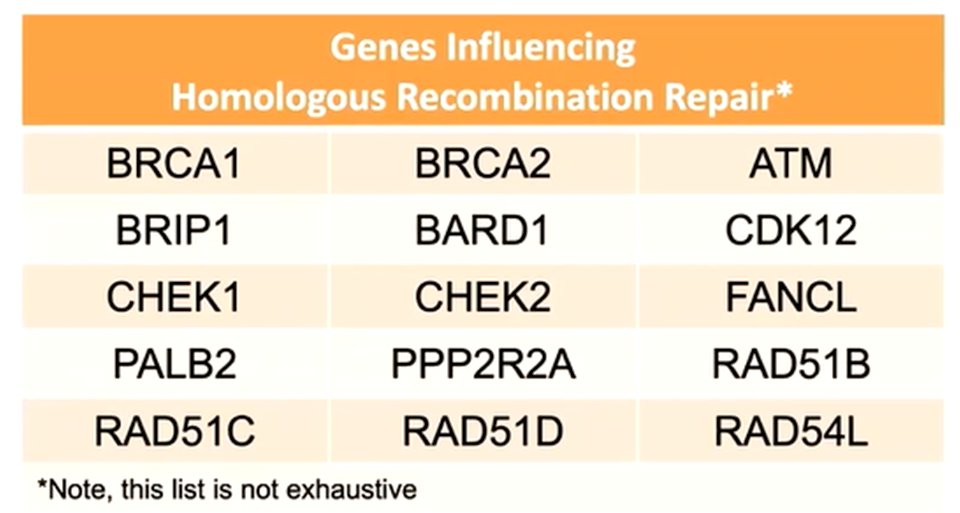
Additionally, in patients with metastatic HSPC, the guidelines recommend genetic counseling and germline testing, independent of age and family history as 10-15% of men with newly diagnosed disease will have homologous recombination repair defects. Identification of these mutations has important implications not just for the proband patient’s treatment but also for cascade testing of family members.
Transitioning from evaluation to treatment, Dr. Cookson emphasized that androgen deprivation therapy with LHRH agonists or antagonists, or surgical castration forms the backbone of therapy. However, based on data which has emerged over the past 5+ years, patients should additionally be offered treatment intensification with abiraterone + prednisone, apalutamide, enzalutamide, or docetaxel.
Dr. Cookson first discussed the role of docetaxel in this disease space, highlighting data from the CHAARTED trial. In this randomized comparison of ADT alone and ADT plus docetaxel in patients with mHSPC, the use of docetaxel was associated with a 10 month improvement in overall survival and a nearly 30% decrease in the relative risk of death. However, importantly, the authors of this trial stratified the study population according to disease extent: high volume disease was defined according to the presence of visceral metastasis or 4 or more bony lesions with at least one beyond the pelvis and vertebral column while low volume disease was the remainder. The benefit of docetaxel was restricted to patients with high volume disease (where the improvement in overall survival was 17 months). Subsequently, the results of a comparison of ADT alone and ADT plus docetaxel from the STAMPEDE trial platform were published confirming the survival benefit of this approach.
In addition to docetaxel, the addition of androgen targeting agents have proven survival benefits in this disease space. Two trials (LATITUDE and STAMPEDE) assessed the role of abiraterone and prednisone in this disease space. Each of these demonstrated significant improvements in overall and radiographic progression-free survival among patients treated with the intensified treatment regime. In the STAMPEDE study, overall survival at 3 years was increased from 76% to 83%. Additionally, the TITAN trial assessed the role of apalutamide in this disease space, similarly finding an overall survival benefit. While ARCHES also assessed the role of enzalutamide in this disease space, Dr. Cookson focused on data from the ENZAMET trial which, like the trials of other agents, demonstrated an overall survival benefit. Notably, there was no difference in outcomes demonstrated according to the volume of disease.
Dr. Cookson then moved from metastatic HSPC to a discussion of treatment options in non-metastatic castration-resistant prostate cancer (nmCRPC). This disease space has seen rapid change over the past few years, with the approval of three new agents on the basis of a newly accepted treatment endpoint (metastasis-free survival). Three studies (SPARTAN, ARMASIS, and PROSPER) have demonstrated the benefit of apalutamide, darolutamide, and enzalutamide, respectively. While these studies first demonstrated benefits in metastasis-free survival (ranging from 22 to 24 months in absolute benefit), follow-up analyses demonstrated improvements in overall survival (ranging from 11 to 14 months in absolute benefit).
Thus, the AUA guidelines on advanced prostate cancer now recommend that clinicians should offer to apalutamide, darolutamide, or enzalutamide in addition to ongoing ADT for patients with high-risk nmCRPC, defined based on a PDA doubling time of 10 months or shorter. Notably, the FDA label is not restrictive on the basis of doubling time but the guideline authors feel that observation may be more appropriate to those with longer doubling times who are at lower risk of developing metastasis. Further, the guideline is clear that systemic chemotherapy or immunotherapy should not be offered to patients with nmCRPC outside the context of a clinical trial.
Dr. Cookson then moved to discuss the mCRPC disease space. In this context, patients should receive conventional imaging at least annually to assess the extent of disease. Further, patients should undergo germline and somatic tumor testing to identify the presence of DNA repair deficiency mutations and microsatellite instability. As discussed in the context of initial diagnosis of mHSPC, identification of these alterations may have important implications for treatment options as well as counseling of family risk and cascade testing.
In mCRPC, Dr. Cookson emphasized the large “menu” of treatment options. Many of these treatment options have subsequently been assessed in other disease spaces and thus previously discussed in mHSPC and nmCRPC.
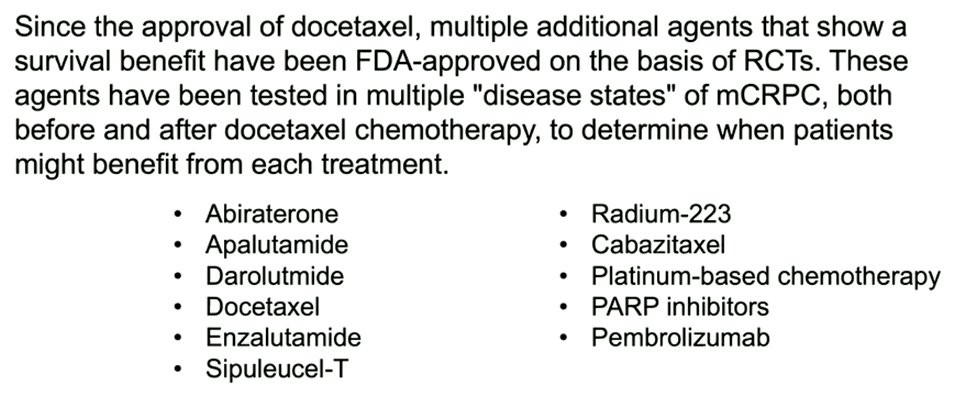
First, in patients with newly diagnosed mCRPC, he emphasized the recommendation for ADT intensification with abiraterone acetate and prednisone, docetaxel, or enzalutamide. He cited data from the COU-AA-302 and COU-AA-301 trials supporting the role of abiraterone acetate in patients pre- and post-chemotherapy, respectively. Similarly, the PREVAIL and AFFIRM trials demonstrated a survival benefit to the use of enzalutamide in patients pre- and post-chemotherapy, respectively. The first agent to show a survival benefit in this disease space was docetaxel, on the basis of data from the TAX-327 trial which demonstrated an overall survival benefit for the use of docetaxel every three weeks.
An alternative strategy for patients with asymptomatic or minimally symptomatic disease is the use of first-line immunotherapy with sipuleucel-T, the first such approach approved for patients with prostate cancer. The IMPACT trial demonstrated a 4-month improvement in overall survival with this approach. Radium-223, an alpha emitter, is recommended for patients with symptomatic disease from bony metastatic disease without known visceral disease based on the results of the ALSYMPCA trial which showed a 30% reduction in the risk of death. Notably, this effect was observed whether patients had previously received docetaxel or not.
In patients who have previously received docetaxel with or without prior androgen axis targeting agents (such as abiraterone or enzalutamide), the guideline panel recommends offering cabazitaxel. Dr. Cookson cited data from the TROPIC trial which demonstrated improved outcomes for patients treated with second-line cabazitaxel. Among patients who have previously received docetaxel and a prior androgen axis targeting agent (such as abiraterone or enzalutamide), the panel recommends cabazitaxel rather than a switch in androgen axis targeting agent, based on data from the CARD trial.
One of the key questions regards treatment sequencing. In general, Dr. Cookson recommended considering previous treatments received when deciding on treatment choice, with a recommendation to use alternative mechanisms of action. Docetaxel, in particular, should be recommended in men with mCRPC who have visceral disease (especially liver metastases), rapidly progressive disease, and those who have previously received androgen axis targeting agents. Notably, the PLATO trial demonstrated that abiraterone does not work well after enzalutamide. Further, the combination of the two agents is no more efficacious but is more toxic than enzalutamide monotherapy.
Dr. Cookson then again emphasized the importance of the identification of DNA repair alterations. In patients for whom these are identified, treatment with a PARP inhibitor is recommended by the guideline panel following prior treatment with an androgen axis targeting agent and/or a taxane based chemotherapy. Two agents, olaparib and rucaparib, have been approved by the FDA for patients with HRR-gene mutated and BRCA1/2-mutated mCRPC, respectively.
Further, in patients with evidence of mismatch repair deficiency or microsatellite instability, patients may be offered pembrolizumab.
Finally, Dr. Cookson highlighted recently published data in 2021 from the VISION trial demonstrating both an overall survival and imaging-based progression-free survival benefit to the use of 177Lu-PSMA-617 in addition to standard of care for patients who were extensively pre-treated with androgen axis targeting agents and taxane-based chemotherapy. Notably, while there was a higher rate of grade 3 or greater adverse events in patients receiving 177Lu-PSMA-617, health-related quality of life was not affected.
In closing, Dr. Cookson emphasized that the role of “precision based therapy” is beginning to emerge for patients with advanced prostate cancer. There are currently a wealth of treatment options and more rationale treatment selection approaches are required moving forward.

Written by: Christopher J.D. Wallis, University of Toronto Twitter: @WallisCJD during the 2022 EAU Section of Oncological Urology (ESOU) Hybrid Annual Meeting, Madrid, Spain, Fri, Jan 21 – Sun, Jan 23, 2022.