She began by highlighting factors that we may consider to support early cystectomy for patients with high-risk non-muscle invasive bladder cancer. First among these, she emphasized that a significant proportion of patients with high-risk non-muscle invasive bladder cancer have muscle invasive or node positive disease. Second, patients with progressive high-risk non-muscle invasive bladder cancer have worse prognosis than patients with primary high-risk non-muscle invasive bladder cancer and primary muscle invasive disease. Third, she suggested that patients with high-risk non-muscle invasive bladder cancer may have poor quality of life. Finally, she emphasized that survival after immediate radical cystectomy is excellent.
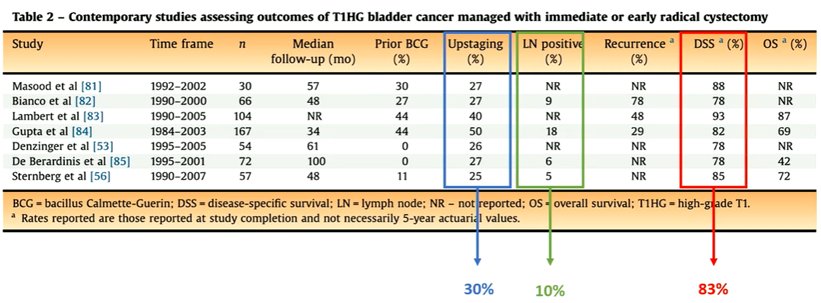
Discussing the first of these points in greater detail, she emphasized that a recent review of series of radical cystectomy in high-risk non-muscle invasive bladder cancer demonstrated an upstaging rate of approximately 30%, a node positive rate of approximately 10%, and a disease specific survival of approximately 83%. Thus, many of these patients with high-risk non-muscle invasive bladder cancer truly have either muscle invasive disease, nodal disease, or both even when managed with immediate or early radical cystectomy.
Addressing the second point and citing two of many studies on the subject, Dr. Masson-Lecomte highlighted that patients who had progression to muscle invasive disease had worse bladder cancer survival than those who initially presented with primary muscle invasive disease (37% vs 67% cancer specific survival at 3-years). Further, the number of transurethral resections prior to radical cystectomy was associated with the likelihood of lymph node metastasis at the time of radical cystectomy: in particularly, lymph node metastasis was found in 8% of patients who underwent a single TURBT prior to cystectomy and 24% in those who underwent 2-4 TURBTs prior to cystectomy.
Highlighting work from Dr. Hautmann, she highlighted that, among patients with T1HG disease, those who underwent early radical cystectomy had lower rates of muscle invasive disease (20% vs 43%) and node positive disease (9% vs 20%) than those who underwent deferred radical cystectomy. Delayed radical cystectomy was reported to be associated with a 15% decrease in survival. However, it bears noting that this study was limited to those patients who eventually underwent radical cystectomy and excludes those patients who had a good response to conservative therapy with BCG.
Summarizing the retrospective literature, Dr. Masson-Lecomte highlighted that approximately 20-30% of patients with high-risk non-muscle invasive bladder cancer have muscle invasive disease at diagnosis and approximately 10% have node positive disease. However, as highlighted above, he emphasized the importance of selection bias in this literature. In particular, she noted that patients with high-risk non-muscle invasive bladder cancer who had good responses to BCG were not included and thus we may be differentially selecting out a particularly high risk subset.
In this context, she highlighted the importance of the BRAVO randomized trial. This study is a randomized feasibility study of radical cystectomy and BCG in patients with high-risk high-grade NMIBC. She noted that this study included all patients with high-grade disease with other high-risk features including CIS, LVI, residual disease on re-resection, pT1 stage, and others. However she emphasized that this cohort is not enriched for very high-risk characteristics as a majority of patients had pTa disease while the remainder had either carcinoma in situ (CIS) or pT1 disease.
Considering outcomes, 23 of 25 patients randomized to BCG received inducaiton and 33% had full maintenance. Four of these patients underwent eventual radical cystectomy with two progressing to distant metastasis. Notably, while adverse events were relatively common in this group (65%), these were mostly grade 1 and 2 events. In the radical cystectomy arm, five patients opted for BCG. Muscle invasive disease was found in 2 patients (10% with pT2) and no patients had nodal disease, rates that are lower than the retrospective literature highlighted above. As of follow-up, all patients were free of disease. A higher proportion of grade 3 and 4 adverse events were seen in this arm, as may be expected following radical cystectomy, though absolute numbers were comparable (65%).
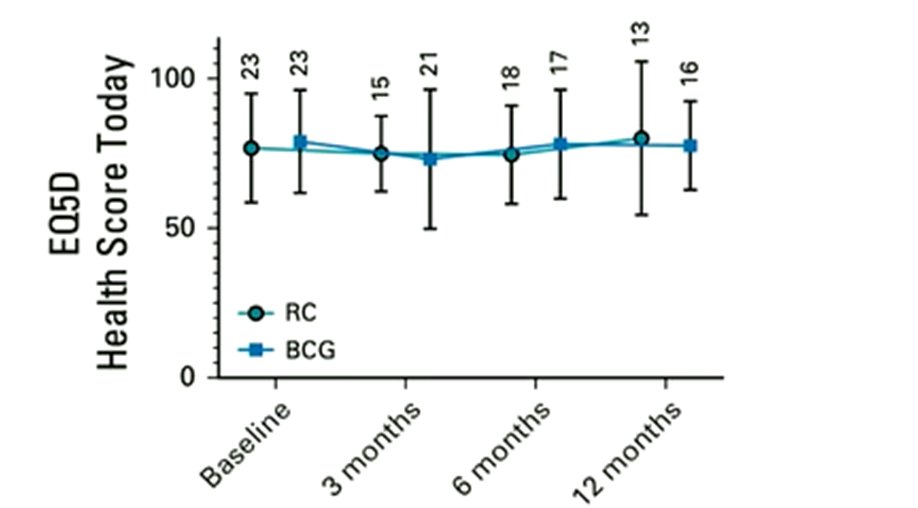
Considering patient reported quality of life, the authors found no differences between the two arms, though the number of patients contributing to this analysis was small.
Comparing these results to the aforementioned retrospective literature, Dr. Masson-Lecomte emphasized that a lower proportion of patients had muscle invasive disease or nodal disease. Further, pT0 rates were relatively high in the radical cystectomy group (25%). Thus, in this cohort, he emphasized that there is a higher risk of overtreatment than undertreatment. As a result, distinguishing between patients with high-risk and very-high-risk disease at diagnosis is critical.
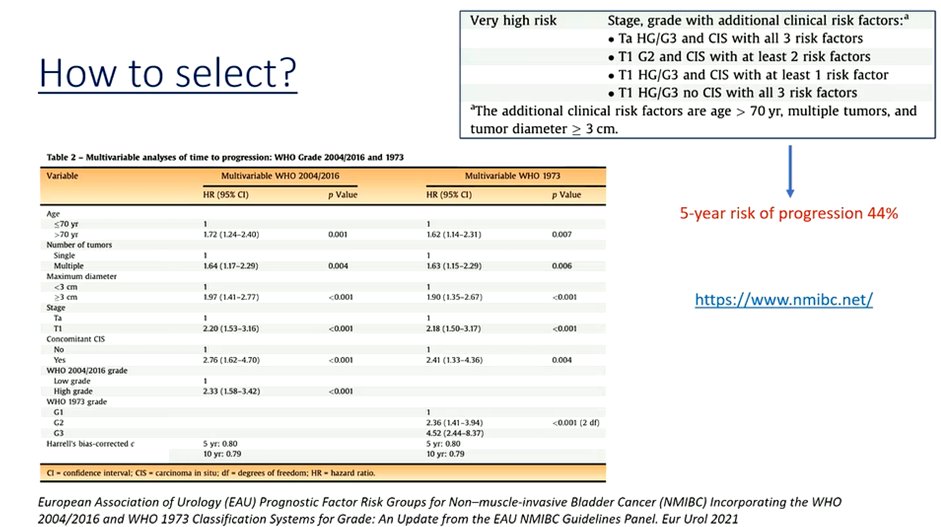
To this end, she highlighted the EAU guidelines and classification of non-muscle invasive bladder cancer as well as the risk prognostic tool (www.nmibc.net). This tool allows identification of the five-year risk of progression. She emphasized that while patients with high-risk disease (such as would represent most of the BRAVO cohort) have a 5-year risk of progression of 11%, this rises to 44% among those with very-high-risk disease.
As a result, she emphasized the importance of accurate risk stratification. She highlighted that not all patients with high-risk non-muscle invasive bladder cancer should be considered for early cystectomy as most patients with be effectively treated by TURBT and maintenance BCG. However, a subset of patients will have potentially lethal disease at diagnosis and omitting early radical cystectomy in these patients will lead to significant survival loss.
Presented by: Alexandra Masson-Lecomte, Hôpital Saint Louis, Paris