(UroToday.com) The 2025 European Society of Medical Oncology (ESMO) Annual Congress, held in Berlin, Germany, between October 17th and 21st was host to the session Radioligand therapeutics. Dr. Louise Emmett discussed Imaging-based theranostics: Is this really happening?
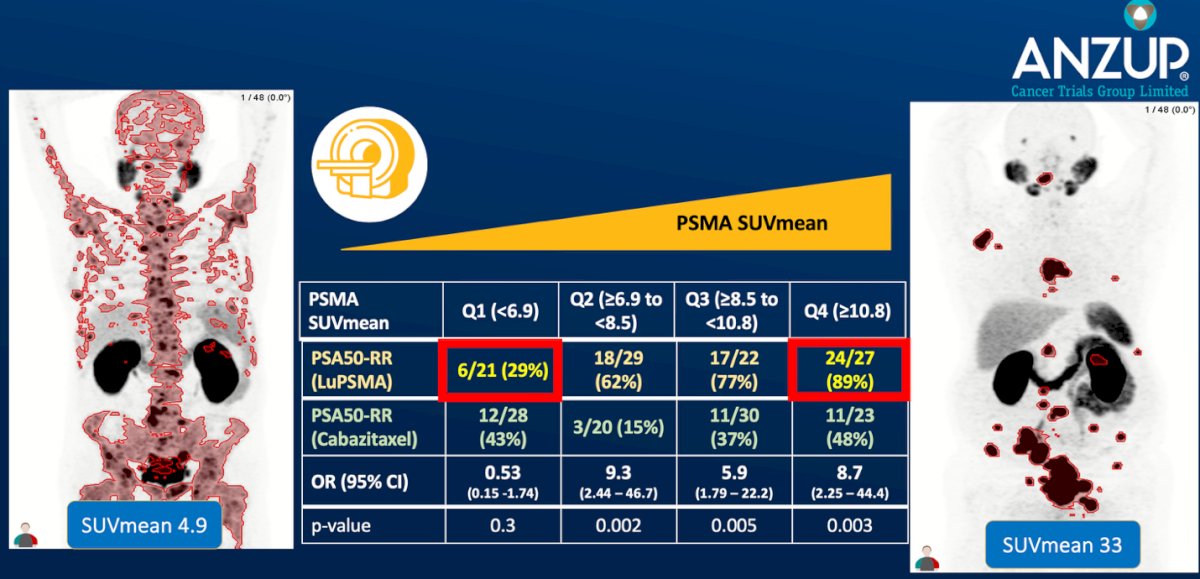
Dr. Emmett began by emphasizing the predictive and prognostic value of PSMA and FDG PET imaging in patients treated with [¹⁷⁷Lu]Lu-PSMA-617 versus cabazitaxel in the TheraP phase II trial. She highlighted that higher PSMA SUVmean strongly correlated with improved PSA50 response rates to Lu-PSMA-617, increasing from 29% in the lowest quartile (SUVmean <6.9) to 89% in the highest (SUVmean ≥10.8). Moreover, survival analysis demonstrated that patients with higher baseline PSMA SUVmean values experienced significantly prolonged overall survival (median 21.4 months for SUVmean ≥9.9 versus 12.6–14.6 months for lower quartiles). These findings support the role of PSMA PET not only as a biomarker for patient selection but also as a quantitative predictor of therapeutic benefit from PSMA-targeted radioligand therapy.1
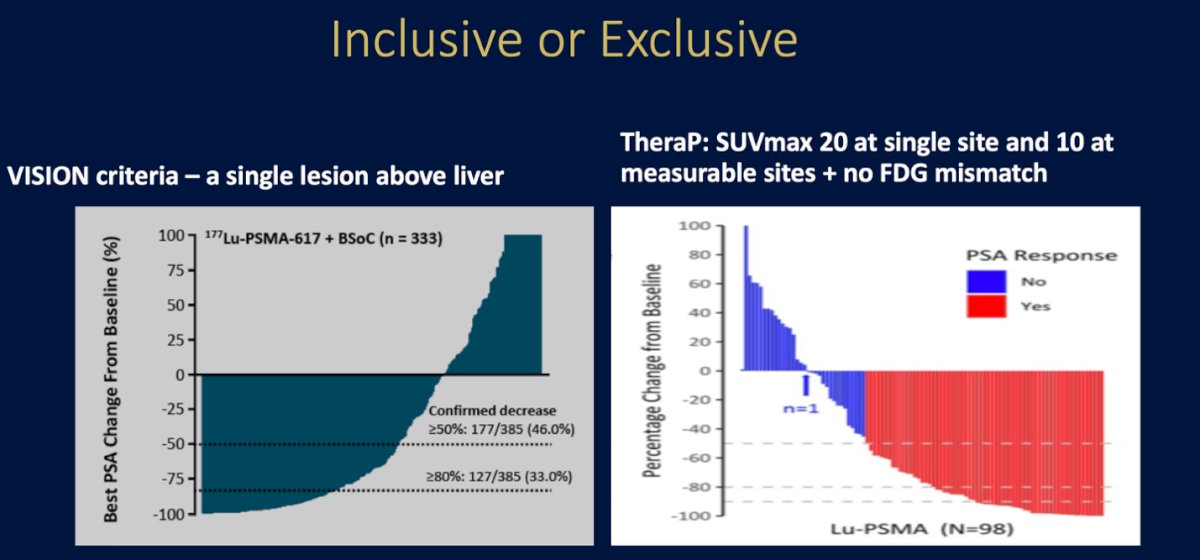
Dr. Emmett then discussed the contrasting inclusion criteria between the VISION and TheraP trials, which significantly influence patient selection for PSMA-targeted radioligand therapy.1,2 The VISION trial adopted a more inclusive approach, allowing enrollment if at least one lesion demonstrated PSMA uptake greater than liver background. In contrast, TheraP used a stricter selection, requiring a PSMA SUVmax ≥20 in at least one site and ≥10 in measurable disease sites, while excluding patients with FDG–PSMA mismatch lesions (FDG-positive but PSMA-negative disease). She pointed out that while more restrictive criteria, such as those in TheraP, enhance the likelihood of response, they may exclude patients who could still derive clinical benefit, representing an opportunity cost, particularly in those with primary resistant disease. Dr. Emmett emphasized the need for a sensible middle ground that balances precision in patient selection with equitable access to therapy, to ensure both efficacy and inclusivity in clinical practice.
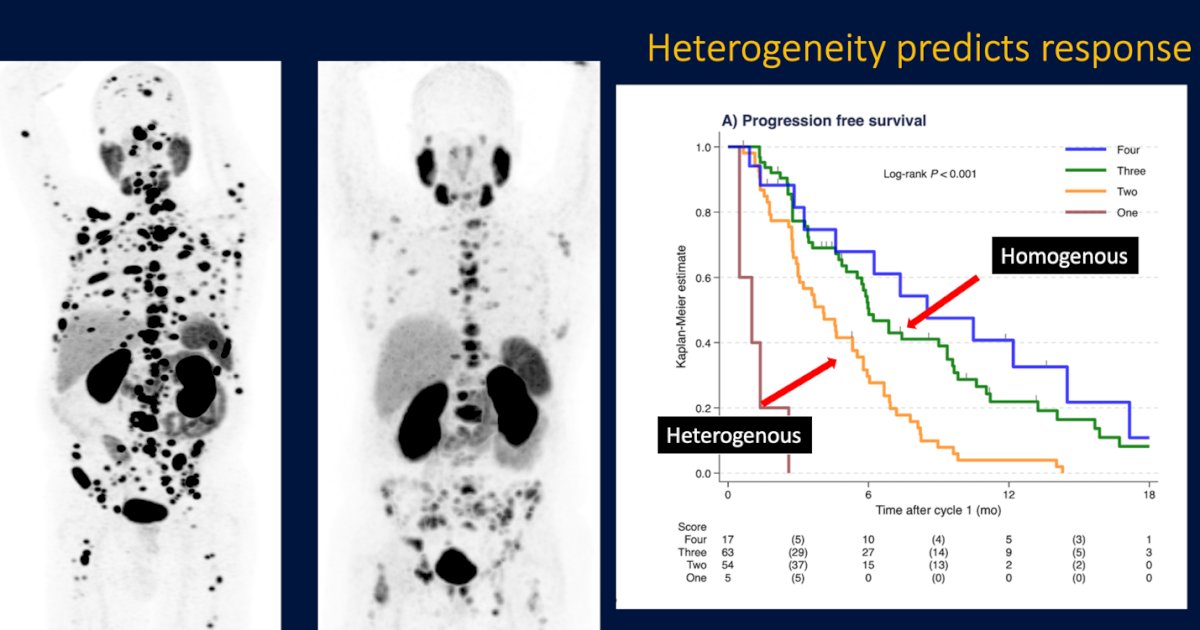
Moreover, Dr. Emmett highlighted that PSMA PET heterogeneity is a strong predictor of treatment response. She referenced data showing that patients with homogeneous and high-intensity PSMA expression experienced significantly better PSA and survival outcomes compared to those with heterogeneous uptake patterns. In the proposed 4-category HIT (heterogeneity and intensity of tumors) scoring system, increasing homogeneity and SUVmax were associated with improved PSA50 response rates, longer PSA-PFS, and overall survival.3
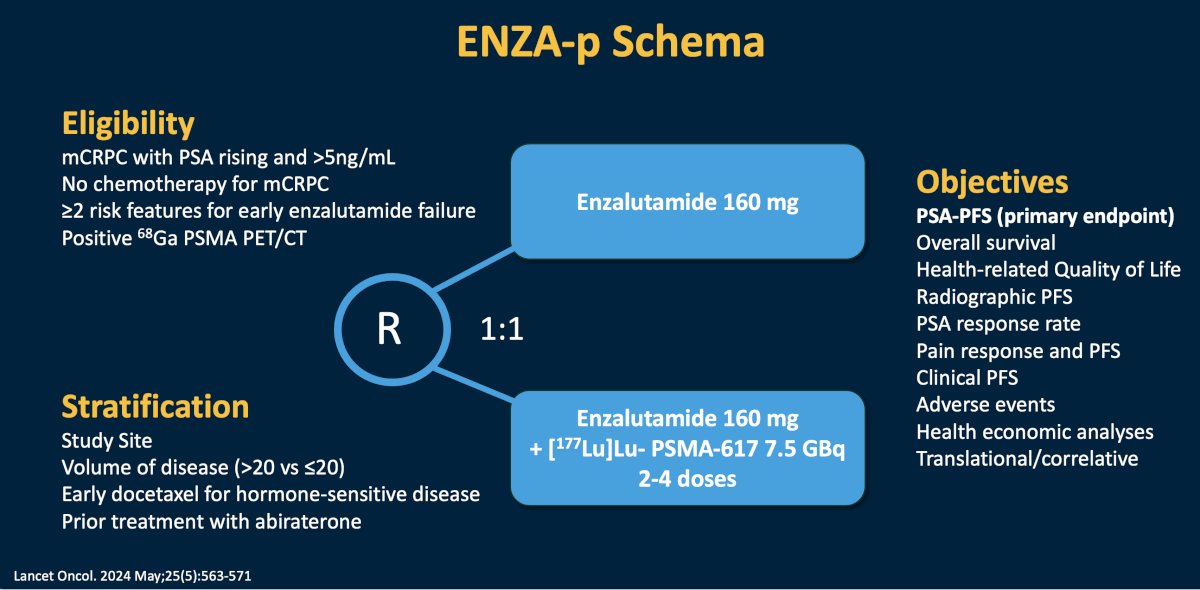
Dr. Emmett then discussed the ENZA-p trial (schema below), which evaluates the addition of 177Lu-PSMA-617 to enzalutamide in patients with mCRPC who have not received prior chemotherapy. She noted that PSMA PET was used as a biomarker for patient selection, with eligibility requiring SUVmax ≥15 in at least one site and ≥10 across all measurable lesions. Despite these inclusion thresholds, the imaging screen failure rate was 18%, underscoring that a subset of patients with insufficient PSMA expression may not benefit from PSMA-targeted RLT. The trial’s design aims to assess whether combining RLT with AR-targeted therapy can improve PSA-PFS, overall survival, and quality of life compared to enzalutamide alone.
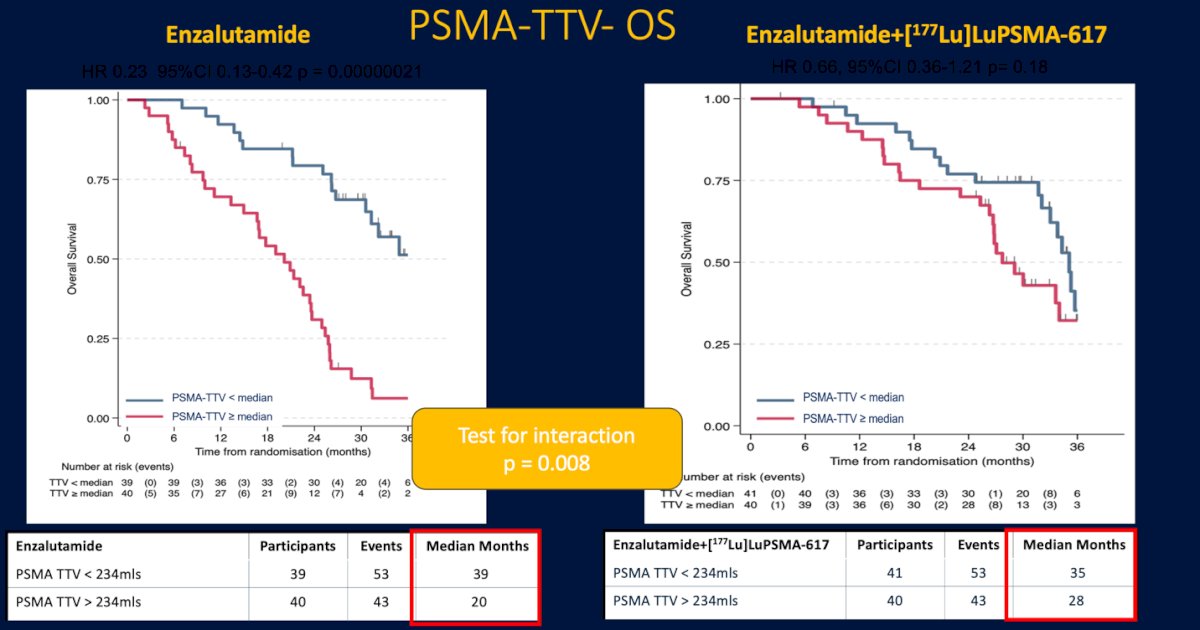
An exploratory analysis from the ENZA-p trial evaluating total tumor volume (PSMA-TTV) as a prognostic biomarker for overall survival. Among patients treated with enzalutamide alone, those with a PSMA-TTV below the median had significantly improved survival compared to those with higher tumor volumes (median OS 39 vs 20 months, HR 0.23, p<0.000001). Interestingly, this difference was less pronounced in the combination arm with 177Lu-PSMA-617, where outcomes were more comparable across tumor burden subgroups (median OS 35 vs 28 months, HR 0.66, p=0.18). The significant test for interaction (p=0.008) suggests that the addition of RLT may mitigate the adverse prognostic impact of high PSMA-TTV, highlighting its potential to overcome tumor burden–driven resistance.4
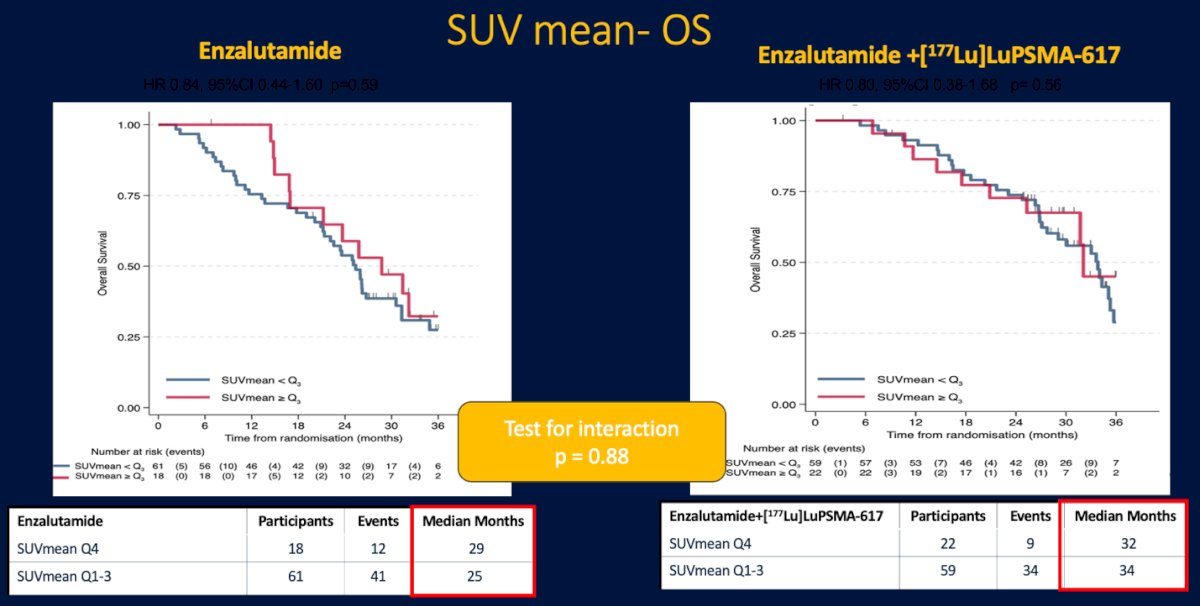
Similarly, when evaluating SUVmean as a predictive biomarker for overall survival, no significant difference was observed between patients with high versus low PSMA uptake. In the enzalutamide-alone arm, median OS was 29 months for those in the highest SUVmean quartile compared to 25 months for the lower quartiles (HR 0.84, p=0.59). In the combination arm with 177Lu-PSMA-617, median OS was 32 and 34 months, respectively (HR 0.80, p=0.56). The test for interaction (p=0.88) showed no differential effect by SUVmean, suggesting that while tumor volume strongly influences outcomes, baseline PSMA uptake intensity alone may not be a reliable predictor of response or survival benefit with radioligand therapy. (4)
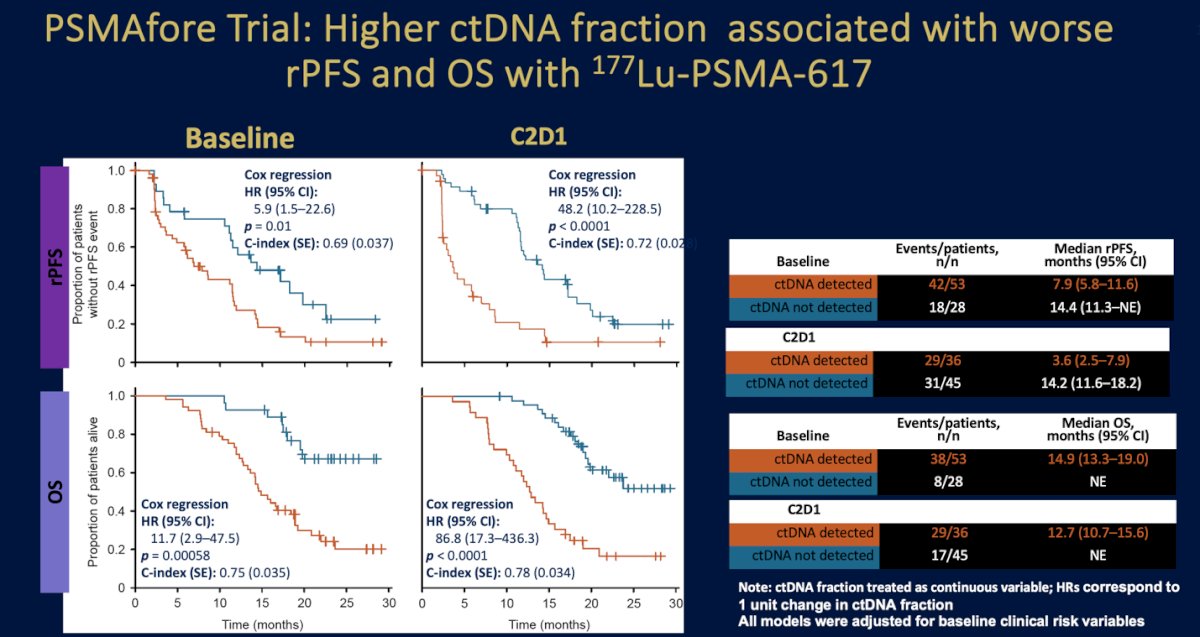
Moreover, Dr. Emmett emphasized that imaging-based screening represents only one component of patient selection for PSMA-targeted therapy. Data from the PSMAfore trial demonstrated that the circulating tumor DNA (ctDNA) fraction also carries strong prognostic significance. Patients with detectable ctDNA at baseline had significantly worse radiographic progression-free survival (median 7.9 vs 14.4 months, HR 5.9, p=0.01) and overall survival (median 14.9 vs not reached, HR 11.7, p=0.00058). This prognostic separation persisted after treatment initiation—by cycle 2 day 1, those with persistent ctDNA positivity continued to fare poorly (median rPFS 3.6 vs 14.2 months; HR 48.2, p<0.0001). These findings underscore that molecular disease burden—captured through ctDNA—may complement PSMA PET in refining prognostication and treatment personalization for patients receiving 177Lu-PSMA-617.5
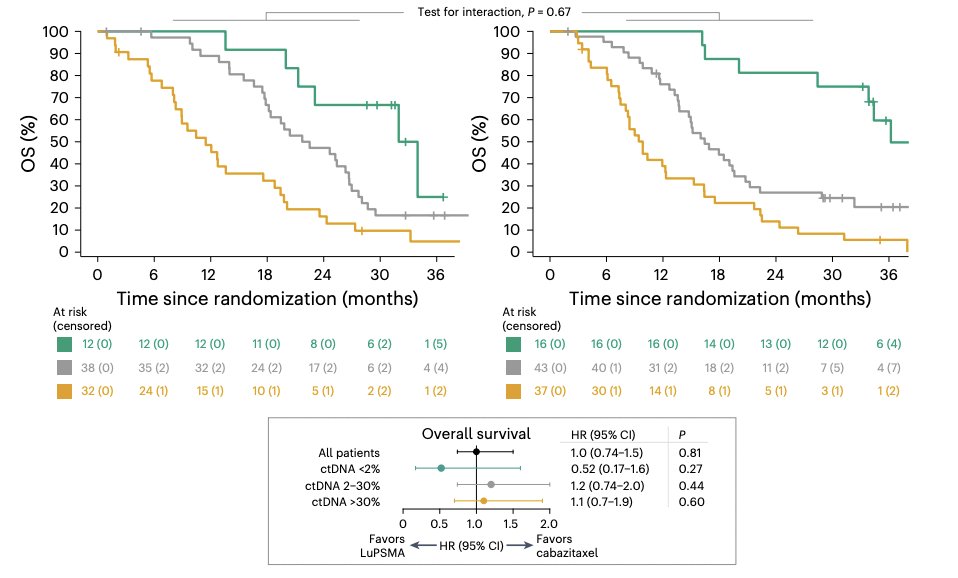
Similarly, in the TheraP ctDNA substudy, patients with undetectable ctDNA experienced superior progression-free survival with 177Lu-PSMA-617 compared to cabazitaxel, while those with higher ctDNA fractions derived less benefit, reinforcing ctDNA as a potential biomarker of treatment sensitivity.6
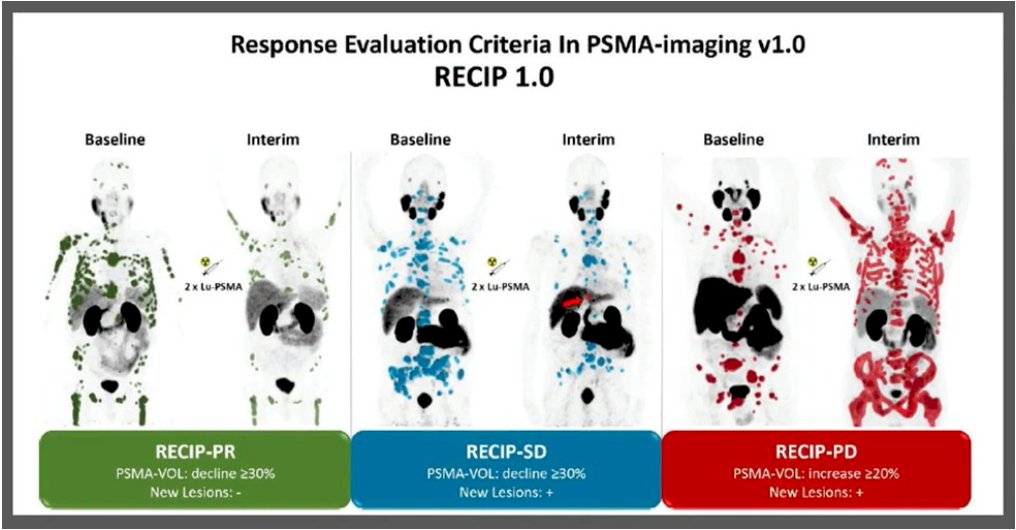
Dr. Emmett emphasized the need for more refined imaging biomarkers to guide treatment response. She highlighted that dynamic biomarkers could enable true personalization of therapy and optimize patient outcomes. Specifically, early response biomarkers are needed to distinguish radiation resistance from sensitivity, while treatment response biomarkers should help identify clinically meaningful progression, ensuring timely adaptation of therapy.
The RECIP (Response Evaluation Criteria in PSMA Imaging) framework is a structured approach for assessing treatment response to 177Lu-PSMA therapy. In a bi-center study of 124 men, baseline and week 12 PSMA PET/CT were analyzed using both quantitative and visual parameters. Median overall survival was 8.3 months for RECIP-PD, 13.0 months for RECIP-SD, and 21.7 months for RECIP-PR (p<0.001). Notably, changes in SUVmax or SUVmean were not prognostic, whereas integrating PSA with RECIP imaging criteria improved identification of responders and progressors compared to PSA alone (p=0.028).7
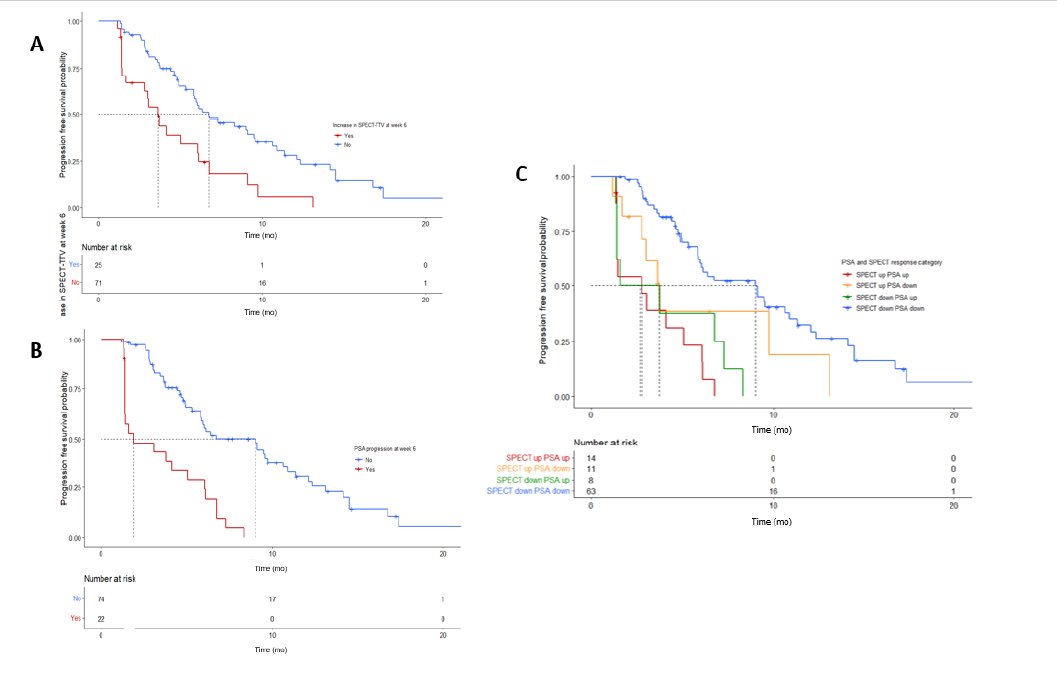
Similarly, findings from the Re-SPECT clinical registry, which included 127 men with mCRPC treated with 177Lu-PSMA (median 3 doses), demonstrated that quantitative 177Lu-PSMA SPECT/CT imaging at week 6 can predict short progression-free survival. Patients with increased SPECT-TTV at week 6 had shorter PSA-PFS (3.7 vs 6.7 months, p<0.0008), and when both PSA and SPECT-TTV progressed, PSA-PFS was significantly reduced (2.8 vs 9.0 months, p<0.0001). Notably, changes in SUVmean or SUVmax were not prognostic.8
Similarly, in a Swiss-wide prospective registry including 73 patients with mCRPC treated with [177Lu]Lu-PSMA (median 6.4 GBq), quantitative SPECT/CT analysis at week 6 showed that early responders by TTV had significantly longer OS (HR 0.28, p<0.01). PSA responders also had improved OS (HR 0.21, p<0.01), and patients who responded by both TTV and PSA achieved the most favorable outcomes (OS HR 0.09, PSA-PFS HR 0.11; both p<0.01). As in prior studies, changes in SUVmax or SUVmean were not predictive of survival or PSA-PFS.9
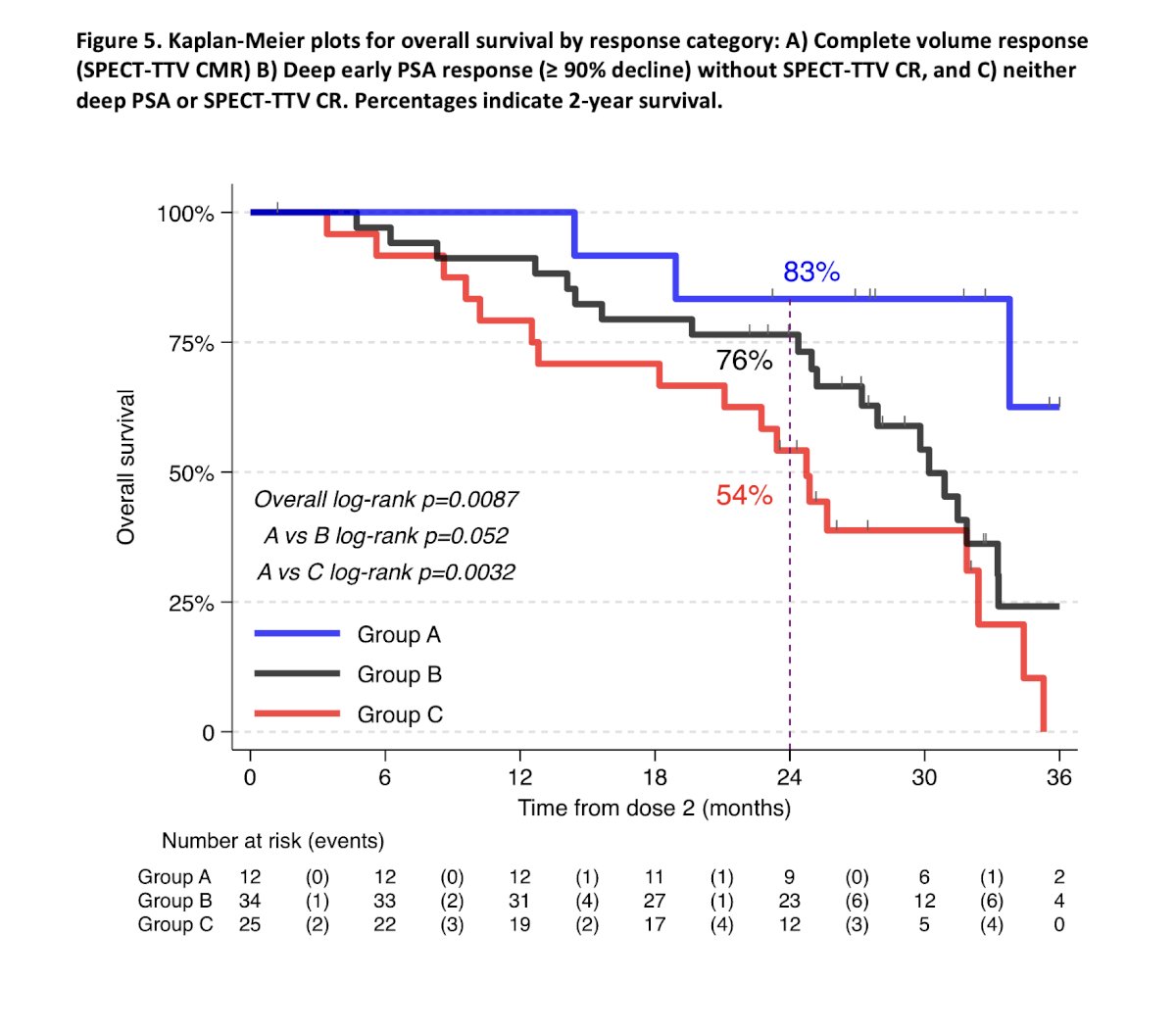
In the ENZA-p trial, which included 81 patients receiving 177Lu-PSMA-617, baseline and week 6 SPECT/CT were analyzed for total tumor volume. Patients achieving a complete response on week 6 PSMA-TTV experienced significantly longer overall survival, with two-year OS rates of 83% for complete responders versus 54% for non-responders (p=0.0087). The combination of PSMA and PSA metrics provided superior predictive value for overall survival compared to either parameter alone.
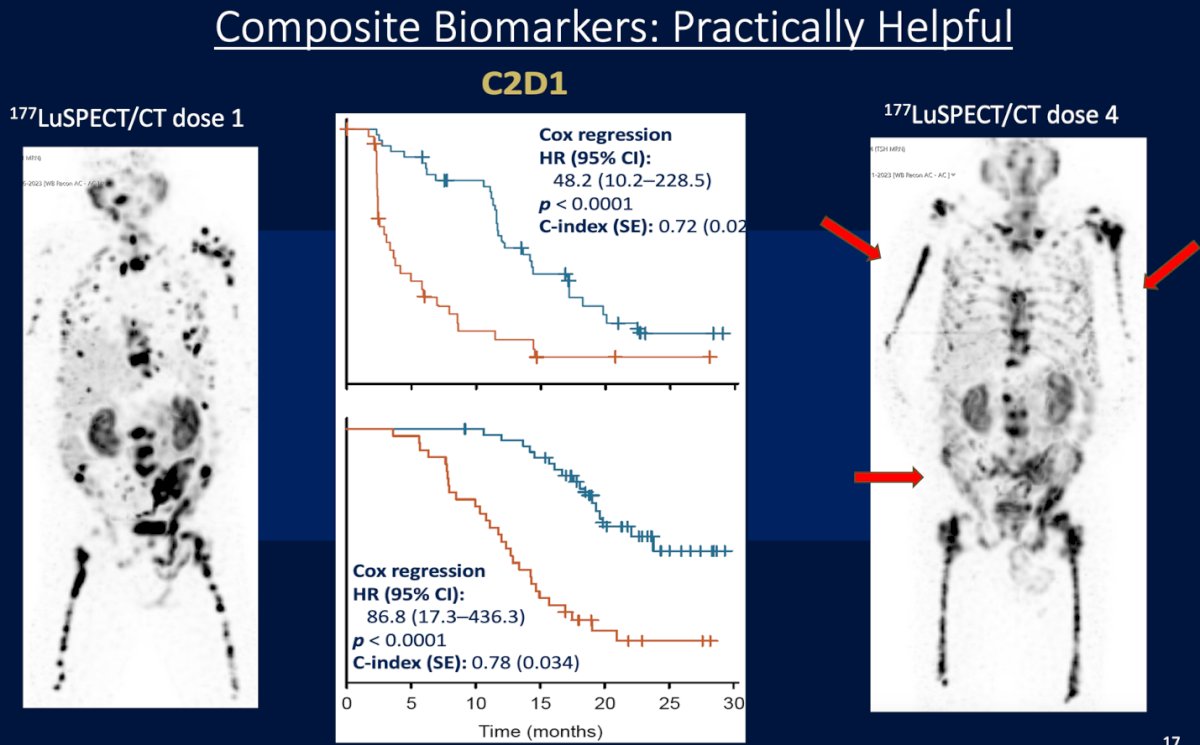
Dr. Emmett highlighted that composite biomarkers integrating both imaging (SPECT/CT) and molecular parameters are practically useful to predict outcomes during 177Lu-PSMA therapy. Early assessments at cycle 2, day 1 (C2D1) already stratify patients by prognosis, with a clear separation in survival curves (HR 48.2 for rPFS and HR 86.8 for OS; both p<0.0001). These composite approaches enable dynamic monitoring and early identification of responders versus non-responders across treatment cycles.
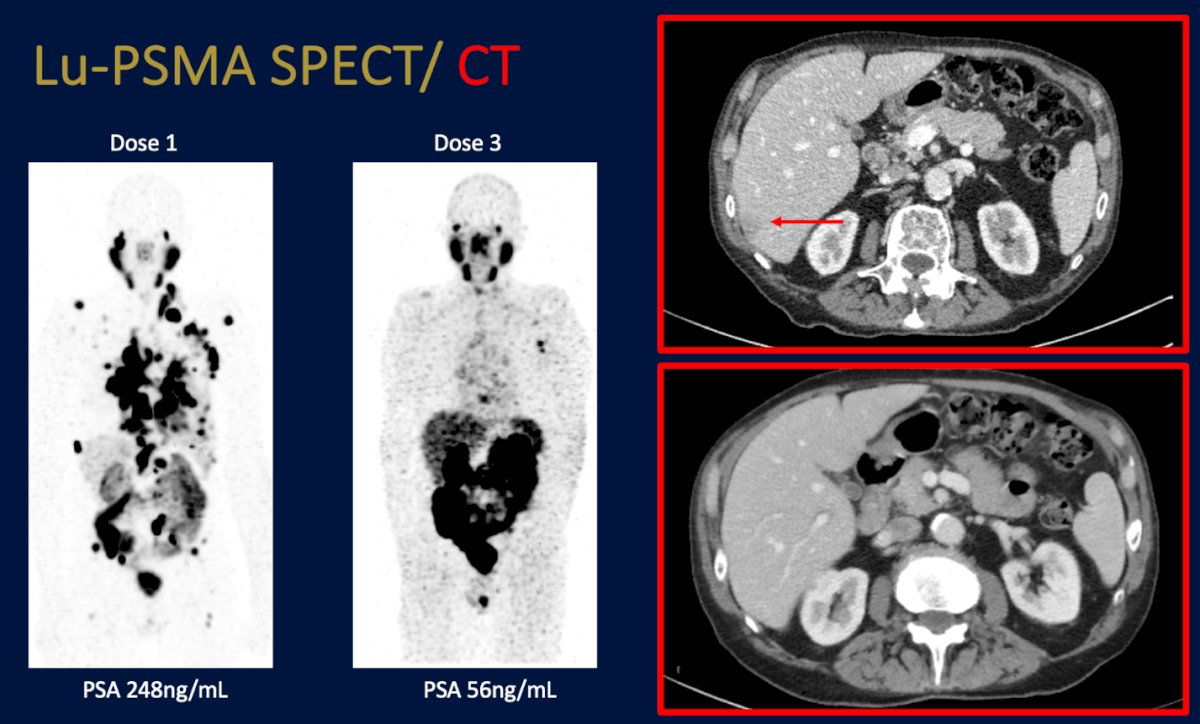
Dr. Emmett emphasized that “everyone deserves at least two doses,” underscoring the importance of reassessing response mid-therapy rather than discontinuing treatment prematurely. Post-treatment Lu-PSMA SPECT/CT allows clinicians to visualize response and tailor therapy accordingly, whether identifying marked responders who may safely stop treatment or detecting progression requiring a change in management. Supporting this, Dr. Thomas Hope shared data showing that nearly half of management changes during RLT were informed by imaging findings, highlighting the critical role of SPECT/CT in real-time decision-making.
Dr. Emmett emphasized the need to develop standardised criteria for treatment response to systemic therapies on PSMA-PET/CT, both for prospective trials and clinical purposes, and concluded by highlighting the SPARC initiative (Standardized PSMA PET Analysis and Reporting Consensus), a multidisciplinary effort to harmonize PSMA-PET/CT reporting in prostate cancer. The Delphi consensus recommended the use of the miTNM framework by PROMISE, incorporation of the PRIMARY score for intra-prostatic staging, and quantitative metrics such as PSMA-VOL, SUVmean, and SUVmax. While SUVmax reporting reached consensus, data remain insufficient to define standardized imaging-based response or progression criteria for PSMA-PET/CT.10
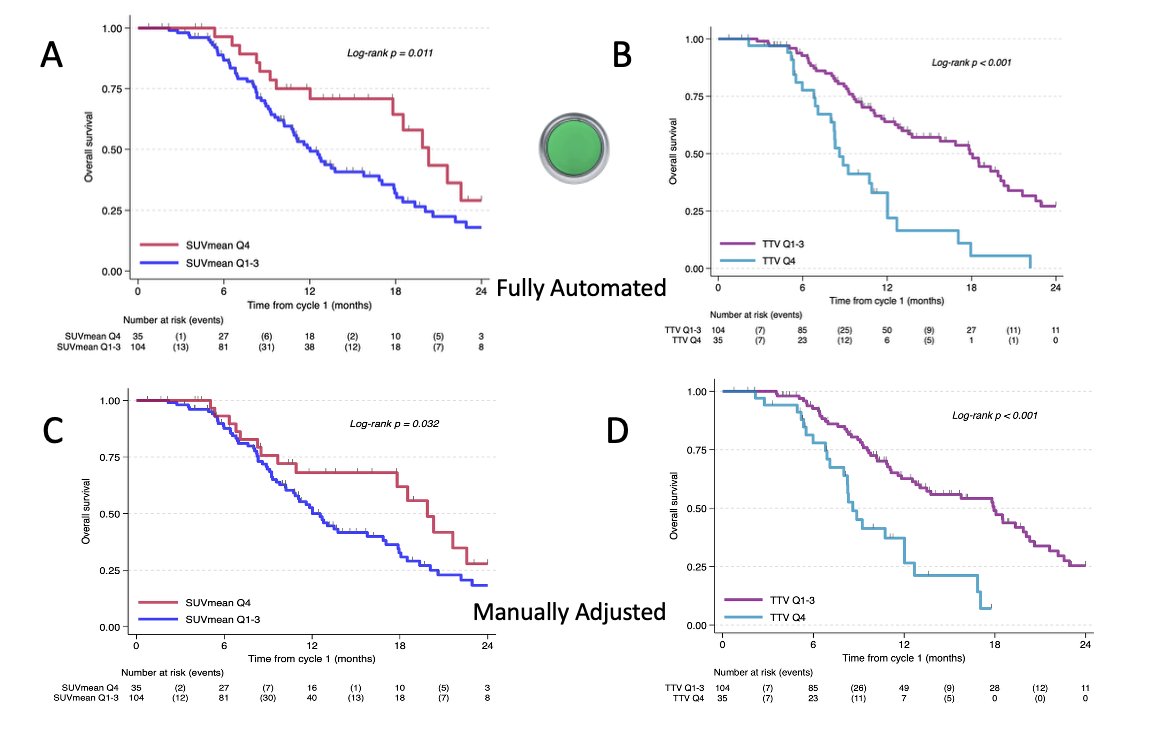
Lastly, data from St Vincent’s Hospital evaluating a fully automated PSMA PET quantification approach in patients treated with 177Lu-PSMA therapy. Among 139 analyzed patients, both automated and manually adjusted methods showed strong prognostic value. Using the automated approach, patients in the highest PSMA-TTV quartile had significantly shorter median OS (8.5 vs 18 months, p<0.001), while those with higher SUVmean also demonstrated inferior survival (12 vs 20 months, p=0.011). These findings suggest that automated PSMA quantification is feasible, reproducible, and closely correlates with progression-free and overall survival.
Dr. Emmett concluded her presentation with the following take-home messages:
- Screening molecular imaging (TTV and SUVmean) is useful in identifying those most likely to respond to 177Lu-PSMA therapy. However, further research is needed to understand how ctDNA and PSMA PET quantitation intersect to best predict RLT response.
- There is potential to expand the use of PSMA PET beyond patient selection for PSMA RLT.
- In ENZA-p, PSMA tumour volume was highly prognostic for overall survival with enzalutamide therapy.
- On-treatment biomarkers are practically useful in guiding therapy response, particularly in patients with heterogeneous disease. This is critical given the absence of current tools to identify radiation-resistant disease at screening.
- Two on-treatment biomarkers may be better than one or perhaps even three.
- Combining PSMA SPECT or PET, PSA, and possibly ctDNA at 12 weeks may better guide treatment response.
Presented by: Louise Emmett, MD, MBChB, FRACP, FAANMS, Professor, Director of Theranostics and Nuclear Medicine, St. Vincent’s Hospital Sydney, University of New South Wales, Sydney, Australia
Written by: Julian Chavarriaga, MD – Urologic Oncologist at Cancer Treatment and Research Center (CTIC) via Society of Urologic Oncology (SUO) Fellow at The University of Toronto. @chavarriagaj on Twitter during the 2025 European Society of Medical Oncology (ESMO) Annual Congress held in Berlin, Germany, between October 17th and 21st.
References:
- Buteau JP, Martin AJ, Emmett L, Iravani A, Sandhu S, Joshua AM, Francis RJ, Zhang AY, Scott AM, Lee ST, Azad AA, McJannett MM, Stockler MR, Williams SG, Davis ID, Hofman MS; TheraP Trial Investigators and the Australian and New Zealand Urogenital and Prostate Cancer Trials Group. PSMA and FDG-PET as predictive and prognostic biomarkers in patients given [177Lu]Lu-PSMA-617 versus cabazitaxel for metastatic castration-resistant prostate cancer (TheraP): a biomarker analysis from a randomised, open-label, phase 2 trial. Lancet Oncol. 2022 Nov;23(11):1389-1397. doi: 10.1016/S1470-2045(22)00605-2. Epub 2022 Oct 16. PMID: 36261050.
- Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, Tagawa ST, Nordquist LT, Vaishampayan N, El-Haddad G, Park CH, Beer TM, Armour A, Pérez-Contreras WJ, DeSilvio M, Kpamegan E, Gericke G, Messmann RA, Morris MJ, Krause BJ; VISION Investigators. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021 Sep 16;385(12):1091-1103. doi: 10.1056/NEJMoa2107322. Epub 2021 Jun 23. PMID: 34161051; PMCID: PMC8446332.
- Swiha M, Papa N, Sabahi Z, Ayati N, John N, Pathmanandavel S, Crumbaker M, Li S, Agrawal S, Ayers M, Hickey A, Sharma S, Nguyen A, Emmett L. Development of a Visually Calculated SUVmean (HIT Score) on Screening PSMA PET/CT to Predict Treatment Response to 177Lu-PSMA Therapy: Comparison with Quantitative SUVmean and Patient Outcomes. J Nucl Med. 2024 Jun 3;65(6):904-908. doi: 10.2967/jnumed.123.267014. PMID: 38637137.
- Emmett L, Subramaniam S, Crumbaker M, Joshua AM, Sandhu S, Nguyen A, Weickhardt A, Lee ST, Ng S, Francis RJ, Goh JC, Pattison DA, Tan TH, Kirkwood ID, Gedye C, Rutherford NK, Kumar ASR, Pook D, Ramdave S, Nadebaum DP, Voskoboynik M, Redfern AD, Macdonald W, Krieger L, Schembri G, Chua W, Lin P, Horvath L, Bastick P, Butler P, Zhang AY, McJannett M, Thomas H, Langford A, Hofman MS, Martin AJ, Davis ID, Stockler MR; ENZA-p Trial Investigators; Australian and New Zealand Urogenital and Prostate Cancer Trials Group. Overall survival and quality of life with [177Lu]Lu-PSMA-617 plus enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer (ENZA-p): secondary outcomes from a multicentre, open-label, randomised, phase 2 trial. Lancet Oncol. 2025 Mar;26(3):291-299. doi: 10.1016/S1470-2045(25)00009-9. Epub 2025 Feb 13. PMID: 39956124.
- Johann S. De Bono et al. Baseline ctDNA analyses and associations with outcomes in taxane-naive patients with mCRPC treated with 177Lu-PSMA-617 versus change of ARPI in PSMAfore.. J Clin Oncol 42, 5008-5008(2024).
- Kwan EM, Ng SWS, Tolmeijer SH, Emmett L, Sandhu S, Buteau JP, Iravani A, Joshua AM, Francis RJ, Subhash V, Lee ST, Scott AM, Martin AJ, Stockler MR, Donnellan G, Annala M, Herberts C, Davis ID, Hofman MS, Azad AA, Wyatt AW; TheraP Investigators and the ANZUP Cancer Trials Group. Lutetium-177-PSMA-617 or cabazitaxel in metastatic prostate cancer: circulating tumor DNA analysis of the randomized phase 2 TheraP trial. Nat Med. 2025 Aug;31(8):2722-2736. doi: 10.1038/s41591-025-03704-9. Epub 2025 May 27. PMID: 40425844.
- Gafita A, Rauscher I, Weber M, Hadaschik B, Wang H, Armstrong WR, Tauber R, Grogan TR, Czernin J, Rettig MB, Herrmann K, Calais J, Weber WA, Benz MR, Fendler WP, Eiber M. Novel Framework for Treatment Response Evaluation Using PSMA PET/CT in Patients with Metastatic Castration-Resistant Prostate Cancer (RECIP 1.0): An International Multicenter Study. J Nucl Med. 2022 Nov;63(11):1651-1658. doi: 10.2967/jnumed.121.263072. Epub 2022 Apr 14. Erratum in: J Nucl Med. 2023 Sep;64(9):1503. PMID: 35422442; PMCID: PMC9635677.
- John N, Pathmanandavel S, Crumbaker M, Counter W, Ho B, Yam AO, Wilson P, Niman R, Ayers M, Poole A, Hickey A, Agrawal S, Perkins G, Kallinen A, Eslick E, Stockler MR, Joshua AM, Nguyen A, Emmett L. 177Lu-PSMA SPECT Quantitation at 6 Weeks (Dose 2) Predicts Short Progression-Free Survival for Patients Undergoing 177Lu-PSMA-I&T Therapy. J Nucl Med. 2023 Mar;64(3):410-415. doi: 10.2967/jnumed.122.264677. Epub 2022 Sep 8. Erratum in: J Nucl Med. 2024 May 1;65(5):809. PMID: 36215568.
- Neubauer MC, Nicolas GP, Bauman A, Fani M, Nitzsche E, Afshar-Oromieh A, Forrer F, Rentsch C, Stenner F, Templeton A, Schäfer N, Wild D, Chirindel A; all investigators on behalf of the SSNM Therapy Working Group. Early response monitoring during [177Lu]Lu-PSMA I&T therapy with quantitated SPECT/CT predicts overall survival of mCRPC patients: subgroup analysis of a Swiss-wide prospective registry study. Eur J Nucl Med Mol Imaging. 2024 Mar;51(4):1185-1193. doi: 10.1007/s00259-023-06536-2. Epub 2023 Dec 1. PMID: 38038755; PMCID: PMC10881597.
- Herrmann K, Walz J, MacLennan S, Briganti A, Cornford P, Czernin J, Eiber M, Fanti S, Fendler WP, Fizazi K, Gafita A, Gillessen S, Goffin K, Hadaschik B, Hofman MS, Hope TA, Maurer T, Morgans AK, Morris MJ, Murphy DG, Oprea-Lager DE, Ost P, ÓSullivan JM, Rouvière O, Sandhu S, Sartor O, Sathekge MM, Tempany C, Witjes W, Emmett L, Bjartell AS. SPARC: The Standardised Prostate-specific Membrane Antigen Positron Emission Tomography/Computed Tomography Analysis and Reporting Consensus: A Delphi Analysis. Eur Urol. 2025 Sep 12:S0302-2838(25)00482-8. doi: 10.1016/j.eururo.2025.08.005. Epub ahead of print. PMID: 40945999.