(UroToday.com) The 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023 was host to a non-prostate, genitourinary tumors mini oral session. Dr. Ursula Vogl delivered the discussant for the preceding three oral abstract presentations:
- A phase II study investigating the safety and efficacy of neoadjuvant atezolizumab in non-urothelial, muscle invasive bladder cancer (ABACUS-2)
- Durvalumab +/- tremelimumab in combination with dose-dense MVAC (ddMVAC) as neoadjuvant treatment in patients with muscle-invasive bladder carcinoma: results of NEMIO, a randomized phase I-II trial
- Study EV-103 Cohort L: Perioperative treatment w/ enfortumab vedotin (EV) monotherapy in cisplatin (cis)-ineligible patients (pts) w/ muscle invasive bladder cancer (MIBC)

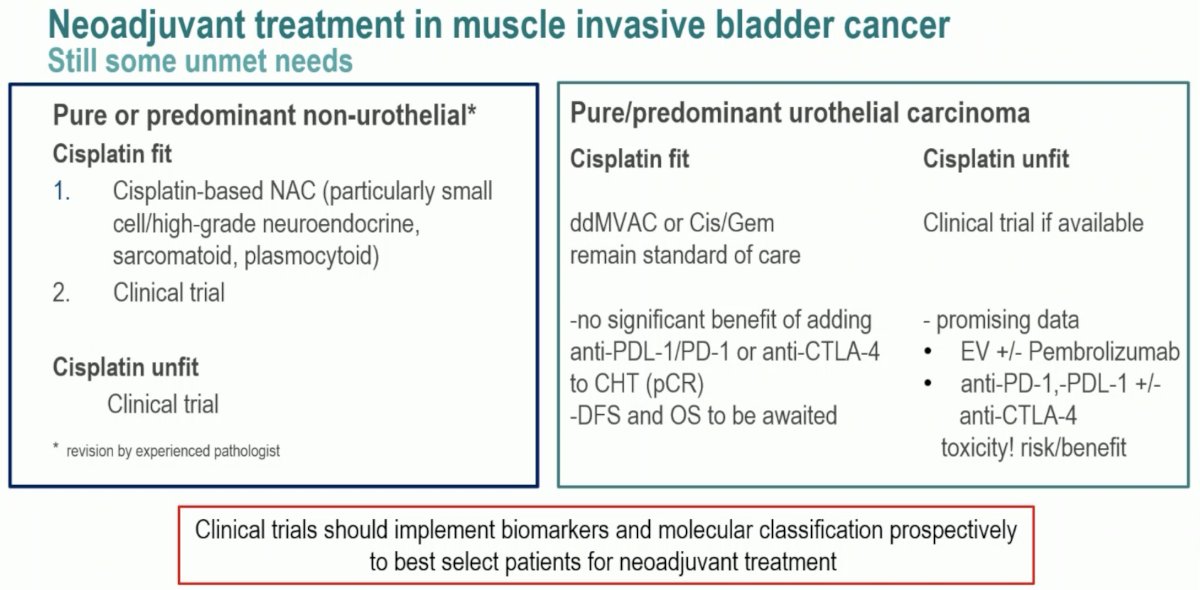
Dr. Vogl noted that the question posed by the ABACUS-2 study is whether or not to perform neoadjuvant treatment in patients with mixed or pure non-urothelial (i.e., variant) histologies. Currently, the data for neoadjuvant therapy in this patient cohort remains limited to evidence from retrospective databases or small clinical trials. For small cell or high-grade neuroendocrine variants, neoadjuvant chemotherapy should be offered.
What about the role of immunotherapy in these patients? The phase II neoadjuvant PURE-01 trial of 3 cycles of pembrolizumab showed a pathologic complete response (pCR) rate of 42% if variant histology represented >50% of the tumor (squamous differentiation or lymphoepithelioma-like variant).1,2 Atezolizumab in locally advanced/metastatic urothelial carcinoma showed an objective response rate of 9% in 47 platinum pre-treated patients in the SAUL phase 3B trial in non-urothelial carcinoma.3
ABACUS-2 included patients with cT1-4aN0-1M0 mixed or pure non-conventional urothelial carcinoma subtype with residual disease following TURBT who were fit and planned for radical cystectomy. Patients must have been assessed as cisplatin-ineligible or not appropriate. Patients were planned for 2 cycles of neoadjuvant atezolizumab (1,200 mg IV every 3 weeks) followed by radical cystectomy and then standard of care follow-up for 2 years. The primary endpoint was pCR.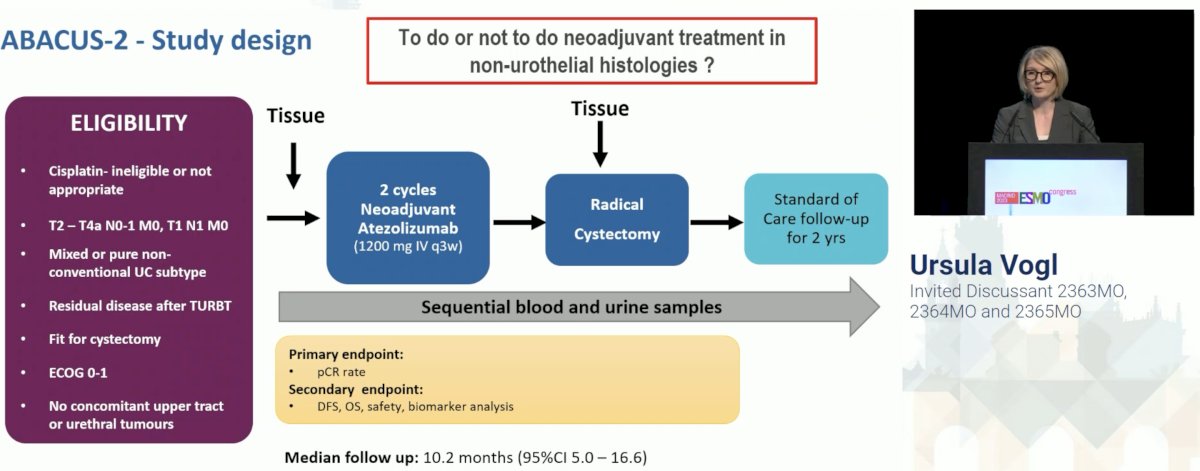
Importantly, patients underwent central pathology review prior to treatment initiation, and as illustrated below, there were significant changes in the assigned variant histologic subtype following the review (45% of cases). Dr. Vogl noted that this emphasizes the need to review the histology in case of non-conventional urothelial carcinoma by an experienced bladder cancer pathologist.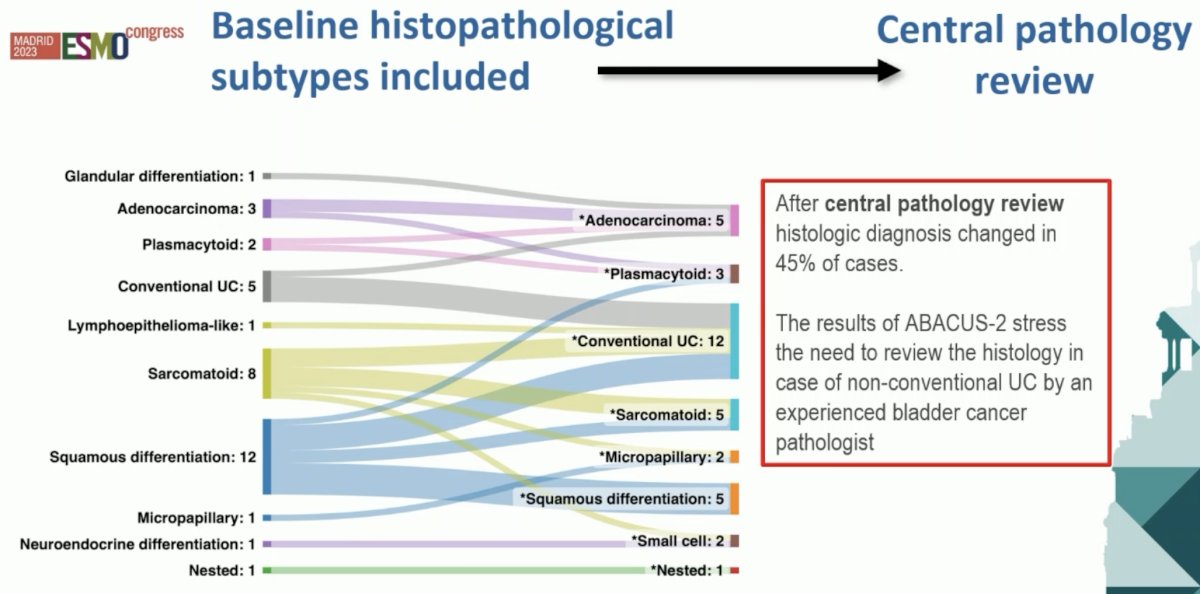
The pCR rate in the 24 patients with evaluable tissue was 38%. The highest pCR rate was observed in those with sarcomatoid variants (62%), although there were only 5 such patients in the cohort.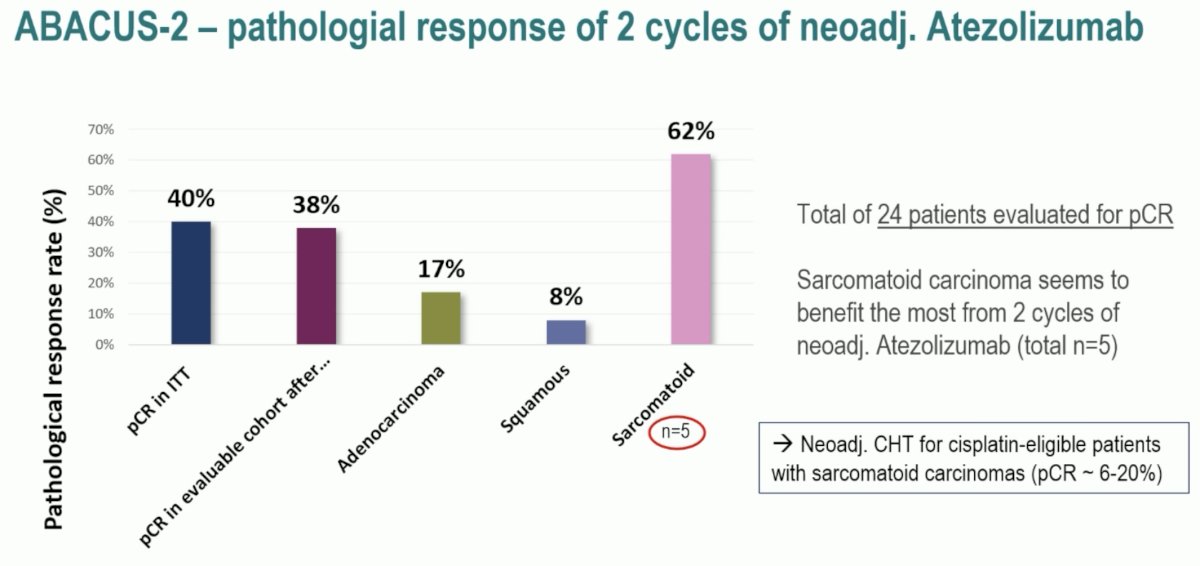
The safety profile of atezolizumab was favorable in this setting. Grade 3-4 treatment-related adverse events occurred in only 1 patient (acute kidney injury), which prevented the patient from receiving the 2nd cycle of atezolizumab. There were no treatment-related deaths. 33/35 patients proceeded to cystectomy.
Dr. Vogl’s take home messages from the ABACUS-2 trial were as follows:
- The efforts to run a trial in rare non-urothelial histologies where evidence for the benefit of neoadjuvant treatment is limited should be applauded
- The high pCR rate of 62% with 2 cycles of atezolizumab in sarcomatoid histology merits further investigation
- The trial has not yet reached its primary endpoint (pCR >30% in 29 patients) since histologies changed significantly (45%) following central pathology review. The trial will thus re-open to conclude enrollment.
- There is a need to review the histology in cases of non-conventional urothelial carcinoma by an experienced bladder cancer pathologist.
Next, Dr. Vogl discussed the NEMIO trial which aimed to evaluate the role of chemotherapy and immunotherapy either in doublet or triplet combinations in patients with predominant urothelial carcinoma, cisplatin eligible MIBC patients. This study is a phase 1/2, non-comparative, open-label, multicenter randomized trial of patients with T2-4N0-1M0 MIBC who were both cisplatin and radical cystectomy eligible. 121 patients were randomized in a 1:1 fashion to either:
- ddMVAC (4 cycles) + durvalumab 1,500 mg every 4 weeks for 2 cycles
- ddMVAC (4 cycles) + durvalumab (2 cycles) + tremelimumab 75 mg every 4 weeks for 2 cycles
All patients were planned for radical cystectomy following systemic, neoadjuvant therapy. The co-primary endpoints were pathologic complete response (pCR; ypT0N0) and safety outcomes.
Importantly, both these combinations were feasible, with 76 - 88% of patients completing all 4 cycles of ddMVAC. In comparison, only 39% of patients in the phase III VESPER trial completed all 6 cycles,4 although we do note the difference in the number of cycles (4 versus 6) between these two trials. From a safety standpoint, the most common all grade treatment-related adverse events (TRAEs) were fatigue (71 – 85%), nausea (68 – 85%), and anemia (57 – 63%) in both arms. The most common grade 3-4 TRAEs were neutropenia (8 – 17%), anemia (8 – 12%), and acute kidney injury (5 – 10%).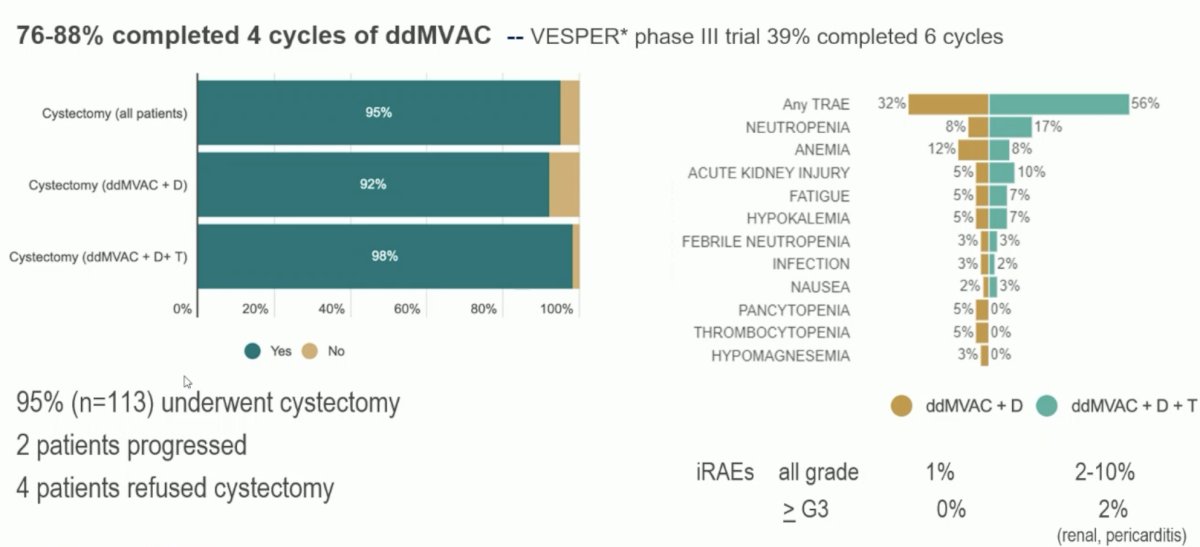
How do the efficacy results from NEMIO compare to other neoadjuvant trials combining chemo-hormonal therapy and anti-PD-(L)1 agents in cisplatin eligible patients? The pCR rate of 47 – 49% is the highest observed to date, although we must highlight the known limitations of cross-trial comparisons.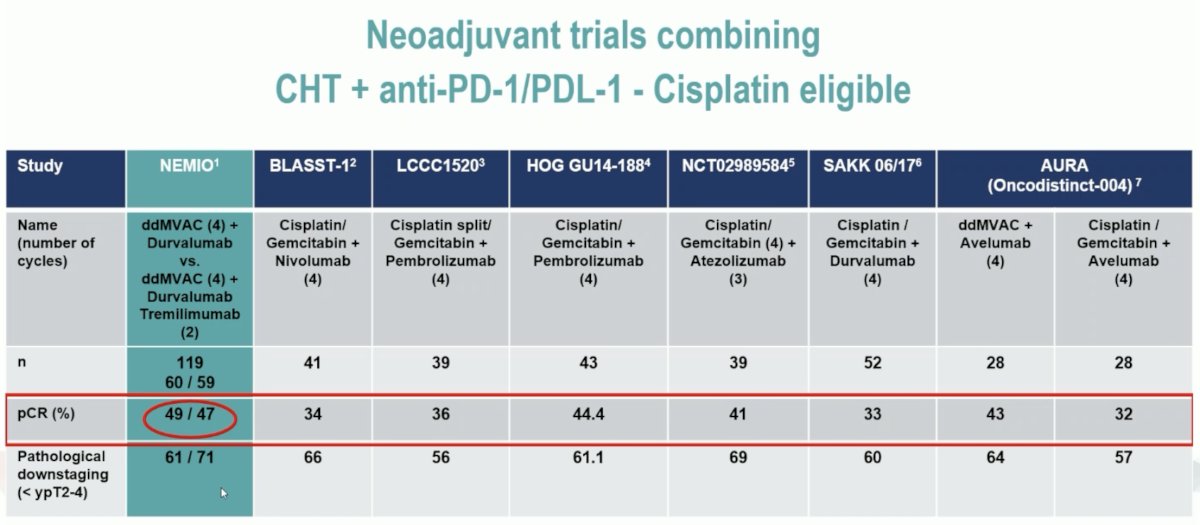
Dr. Vogl’s take home messages from this trial were:
- Adding two cycles of durvalumab +/- tremelimumab to current standard of care (ddMVAC) as neoadjuvant treatment was safe and did not lead to significant treatment discontinuation or cystectomy postponement
- The overall pCR rate of 48% seems comparable to ddMVAC in the VESPER phase III trial (42%) – the 3rd ‘control’ comparator of ddMVAC-only is missing in this trial.
- DFS and OS need further follow-up before any conclusion for further trials can be made
Finally, Dr. Vogl discussed the results from EV-103 Cohort L of perioperative EV in cisplatin-ineligible MIBC. EV-103 Cohort L included patients with cisplatin-ineligible cT2-4aN0M0 or cT1-4aN1M0 urothelial carcinoma patients medically fit for a radical cystectomy + pelvic nodal dissection. Following enrollment, patients were given EV monotherapy (1.25 mg/kg) in 3-week cycles on days 1 and 8 for 3 cycles total. Following surgery, patients received the same regimen for 6 cycles. The primary endpoint was pCR.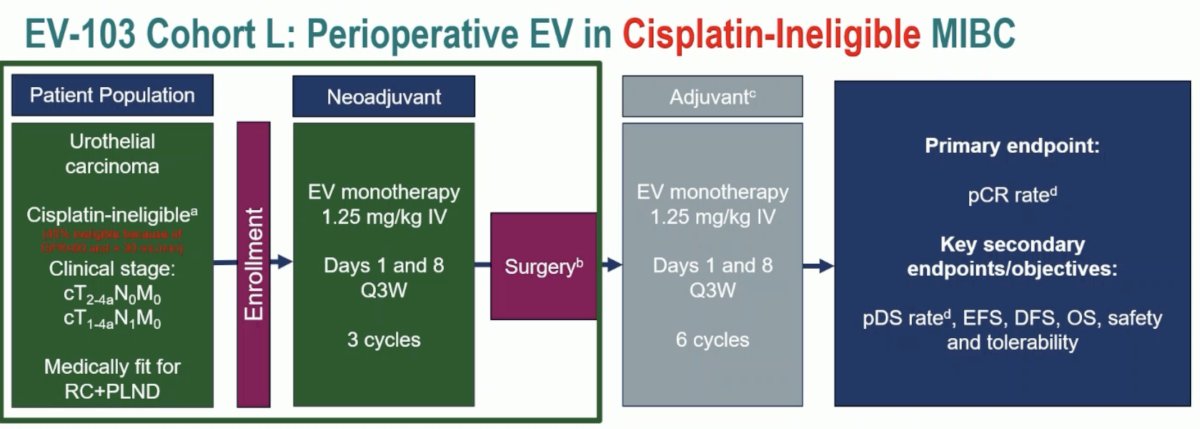
82.4% of patients completed all 3 cycles of neoadjuvant EV, with all these patients completing surgery within a median time of 1.3 months from the last EV dose. 39% of patients experience grade 3+ TEAEs during the neoadjuvant and radical cystectomy period (up to 30 days following last dose of EV and/or surgery). While the results of this report provide us with the important data regarding the safety of 3 neoadjuvant cycles, we await the results of the adjuvant EV phase toxicity data that will be of utmost interest.
Contextualizing the results of these trials within the framework of those evaluating neoadjuvant/perioperative therapy in cisplatin ineligible/refusing patient shows that the pCR rate in EV-103 Cohort L is comparable to those observed in the other trials (29 – 46%).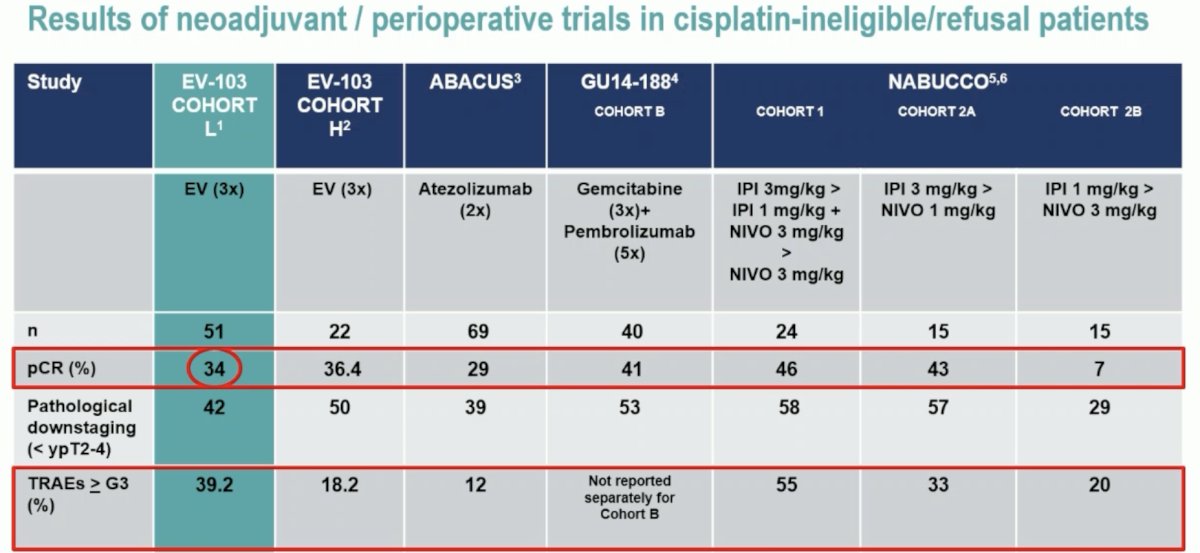
Dr. Vogl’s take home messages from EV-103 Cohort L were as follows:
- The cisplatin-ineligible population has a high unmet need for neoadjuvant treatment. Clinical trials in this population are of great importance.
- The majority of patients completed all 3 neoadjuvant cycles of EV and underwent cystectomy
- Pathologic downstaging and pCR rates are not higher than reported in trials with immune checkpoint inhibitor treatment
- Higher (39.2%) and clinically significant (G3+) adverse event rate reported so far. Reversibility and occurrence in the adjuvant phase will be of utmost interest in a cisplatin-unfit (frail) patient population
Presented by: Ursula Vogl, MD, MBA, Senior Physician Oncologist at Istituto Oncologico della Svizzera Italiana, Clinical Head of the Prostate Cancer Center of Southern Switzerland (CPSI), Bellinzona, Switzerland
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023
References:- Necchi A, Anichini A, Raggi D, et al. Pembrolizumab as Neoadjuvant Therapy Before Radical Cystectomy in Patients with Muscle-Invasive Urothelial Bladder Carcinoma (PURE-01): An Open-Label, Single-Arm, Phase II Study. J Clin Oncol 2018 Dec 1;36(34):3353-3360.
- Necchi A, Raggi D, Gallina A, et al. Updated Results of PURE-01 with Preliminary Activity of Neoadjuvant Pembrolizumab in Patients with Muscle-invasive Bladder Carcinoma with Variant Histologies. Eur Urol 2020 Apr;77(4):439-446.
- Sternberg CN, Loriot Y, James N, et al. Primary results from SAUL, a multinational single-arm safety study of atezolizumab therapy for locally advanced or metastatic urothelial or nonurothelial carcinoma of the urinary tract. Eur Urol 2019 Jul;76(1):73-81.
- Pfister C, Gravis G, Flechon A, et al. Dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin or gemcitabine and cisplatin as perioperative chemotherapy for patients with nonmetastatic muscle-invasive bladder cancer: Results of the GETUG-AFU V05 VESPER trial. J Clin Oncol. 2022;40(18):2013-2022.
ESMO 2023: ABACUS-2, A Phase II Study Investigating the Safety and Efficacy of Neoadjuvant Atezolizumab in Non-Urothelial Muscle Invasive Bladder Cancer
ESMO 2023: NEMIO, a Randomized Phase I-II Trial: Durvalumab +/- Tremelimumab in Combination with Dose-Dense MVAC as Neoadjuvant Treatment in Patients with Muscle-Invasive Bladder Carcinoma
ESMO 2023: EV-103 Cohort L: Perioperative Treatment with Enfortumab Vedotin Monotherapy in Cisplatin-Ineligible Patients with Muscle Invasive Bladder Cancer