(UroToday.com) The 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023 was host to a non-prostate, genitourinary tumors mini oral session. Dr. Constance Thibault presented the results of NEMIO, a randomized phase I-II trial evaluating the combination of durvalumab +/- tremelimumab in combination with dose-dense methotrexate, vinblastine, doxorubicin (Adriamycin), and cisplatin (ddMVAC) for patients with muscle-invasive bladder cancer (MIBC).
Neoadjuvant cisplatin-based chemotherapy followed by radical cystectomy is the current guideline-recommended standard of care for the treatment of muscle invasive bladder cancer; however, 35-50% of patients still have residual muscle invasive disease (i.e., ≥ypT2 or N+).1 Pre-clinical studies suggest that ddMVAC may increase the efficacy of anti-PD(L)-1 therapy, via the following two mechanisms:
- Low-dose methotrexate enhances the maturation of dendritic cells leading to increased T-cells proliferation
- Anthracycline can induce immunogenic cell death, leading to increased PD-L1 and IFN- γ expression, decreased immunosuppressive and myeloid-derived suppressor cell activity, and thus decreased regulatory T-cell function.
As such, combining chemotherapy with anti-PD(L)-1 agents may enhance the anti-tumor activity of both treatments. The objective of the NEMIO study was to evaluate the efficacy and safety of neoadjuvant ddMVAC + durvalumab +/- tremelimumab for MIBC patients treated with radical cystectomy.
NEMIO is a phase 1/2, non-comparative, open-label, multicenter randomized trial of patients with T2-4N0-1M0 MIBC with predominant urothelial component, who were both cisplatin and radical cystectomy eligible. 121 patients were randomized in a 1:1 fashion to either:
- ddMVAC (4 cycles) + durvalumab 1,500 mg every 4 weeks for 2 cycles
- ddMVAC (4 cycles) + durvalumab (2 cycles) + tremelimumab 75 mg every 4 weeks for 2 cycles
All patients were planned for radical cystectomy following systemic, neoadjuvant therapy. The co-primary endpoints were pathologic complete response (pCR; ypT0N0) and safety outcomes. The secondary endpoints were:
- Pathologic downstaging (≤ypT1N0)
- Disease-free survival
- Overall survival
Following safety assessment in a phase I cohort of 12 patients, the study was planned for the phase II efficacy cohort of 109 patients.
The safety population included 119 patients, with the efficacy cohort including 113 patients (6 did not undergo cystectomy: 4 refused cystectomy and 2 had progressive disease).
The baseline patient characteristics are summarized below. The median patient age was 64. Pure urothelial histology was present in 84%, with the remaining having mixed urothelial-variant histology. 9% had cT3-4 and 4% had known cN1 disease. Macroscopic residual tumor following TURBT was present in 32% of patients (41% additional with no available data).
In the ddMVAC + durvalumab arm, 88% of patients completed all 4 cycles of ddMVAC and 97% completed the 2 cycles of durvalumab (all drugs completion: 88%). Conversely in the ddMVAC + durvalumab + tremelimumab arm, 76% completed all 4 cycles of ddMVAC, and 90% completed durvalumab + tremelimumab (all drugs completion: 90%). The median time from randomization to surgery was 12.4 weeks, and the median time to surgery from last injection was 6 weeks.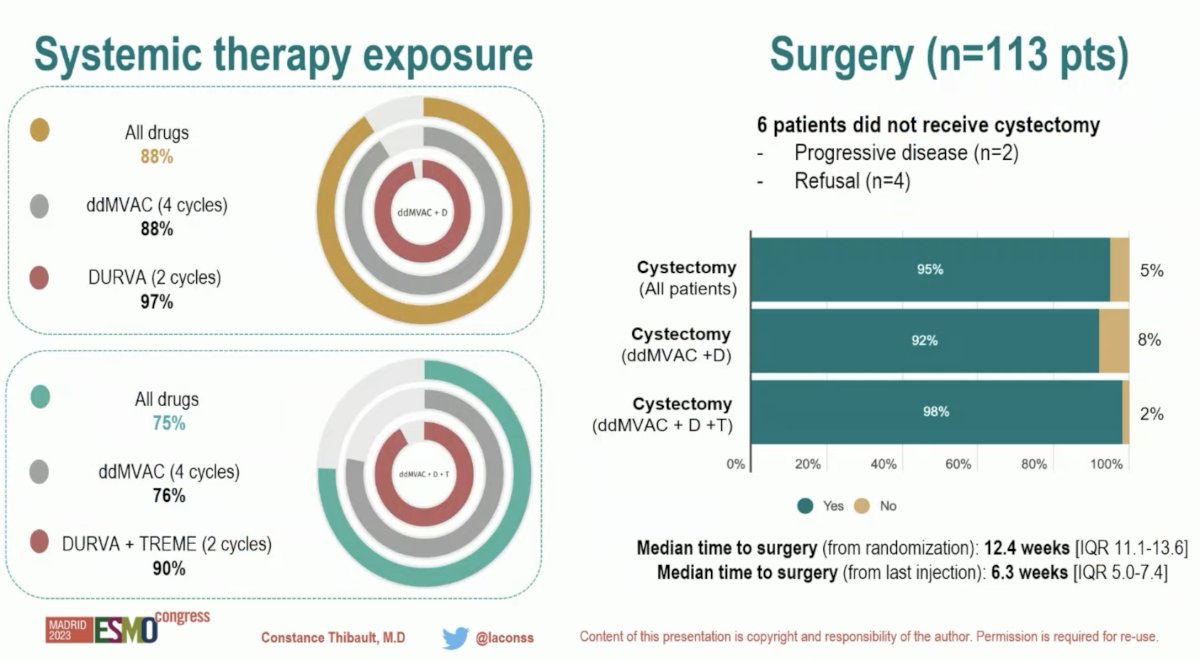
From a safety standpoint, the most common all grade treatment-related adverse events were fatigue (71 – 85%), nausea (68 – 85%), and anemia (57 – 63%) in both arms.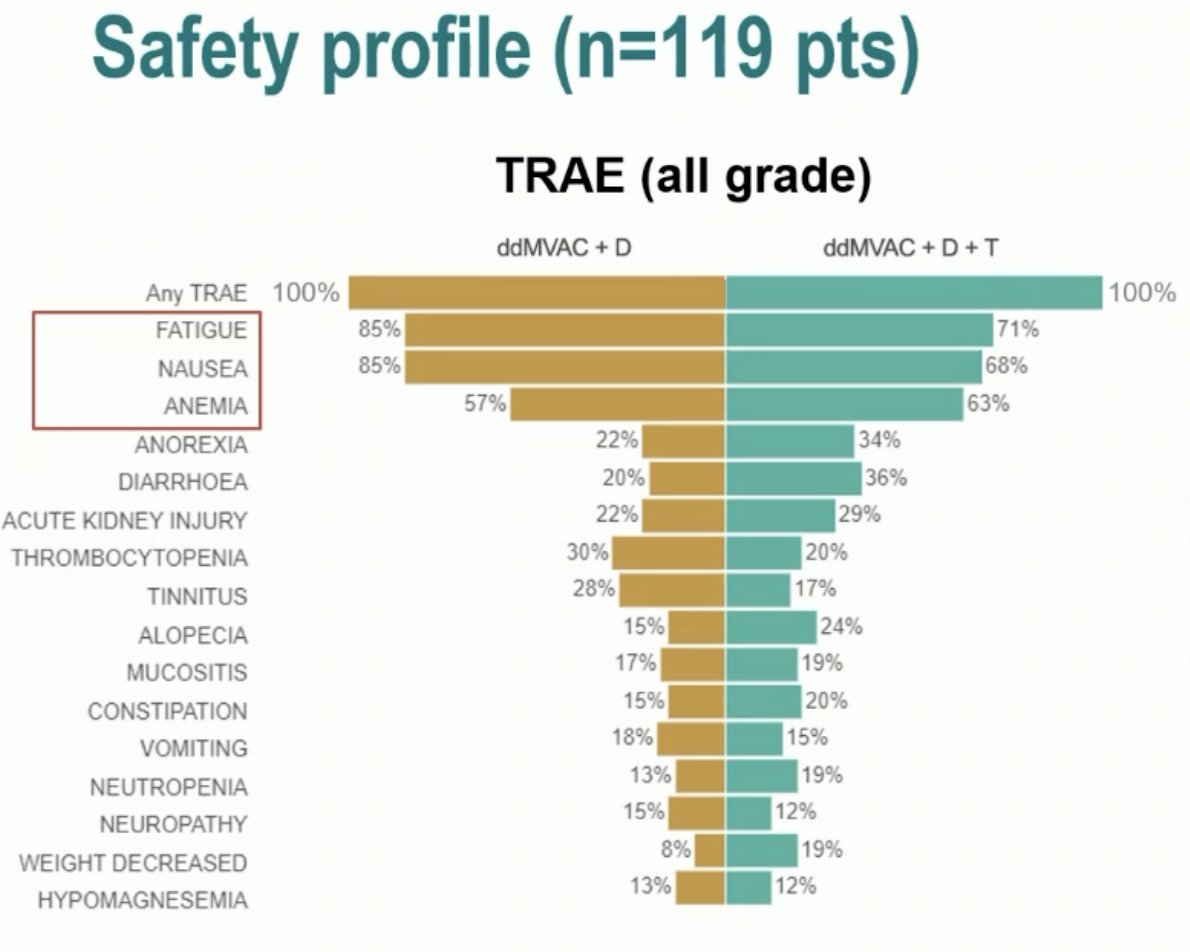
The most common grade 3-4 TRAEs were neutropenia (8 – 17%), anemia (8 – 12%), and acute kidney injury (5 – 10%).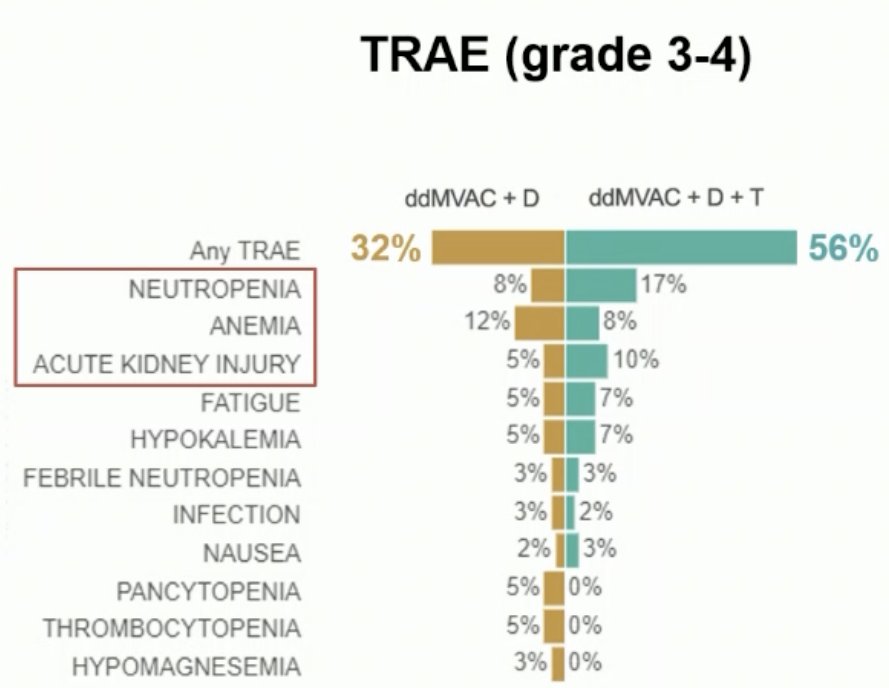
The immune-related adverse events are summarized below: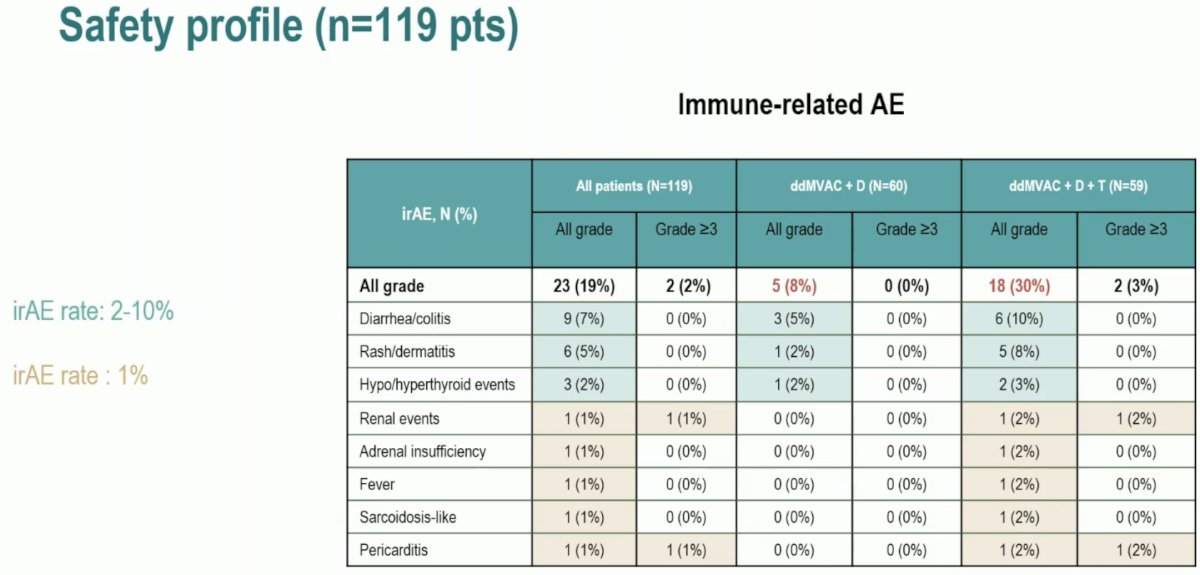
From an efficacy standpoint, the pCR was similar in both arms at 49% with ddMVAC + durvalumab and 47% with ddMVAC + durvalumab + tremelimumab. Pathologic downstaging to ≤ypT1N0 occurred in 66% of patients overall (71% in dual therapy arm; 61% in triplet therapy arm). 34% of patients had residual muscle-invasive disease.
At a median follow-up of 15 months, the 1-year disease-free rate was 80% with doublet therapy and 90% with the triplet therapy regimen.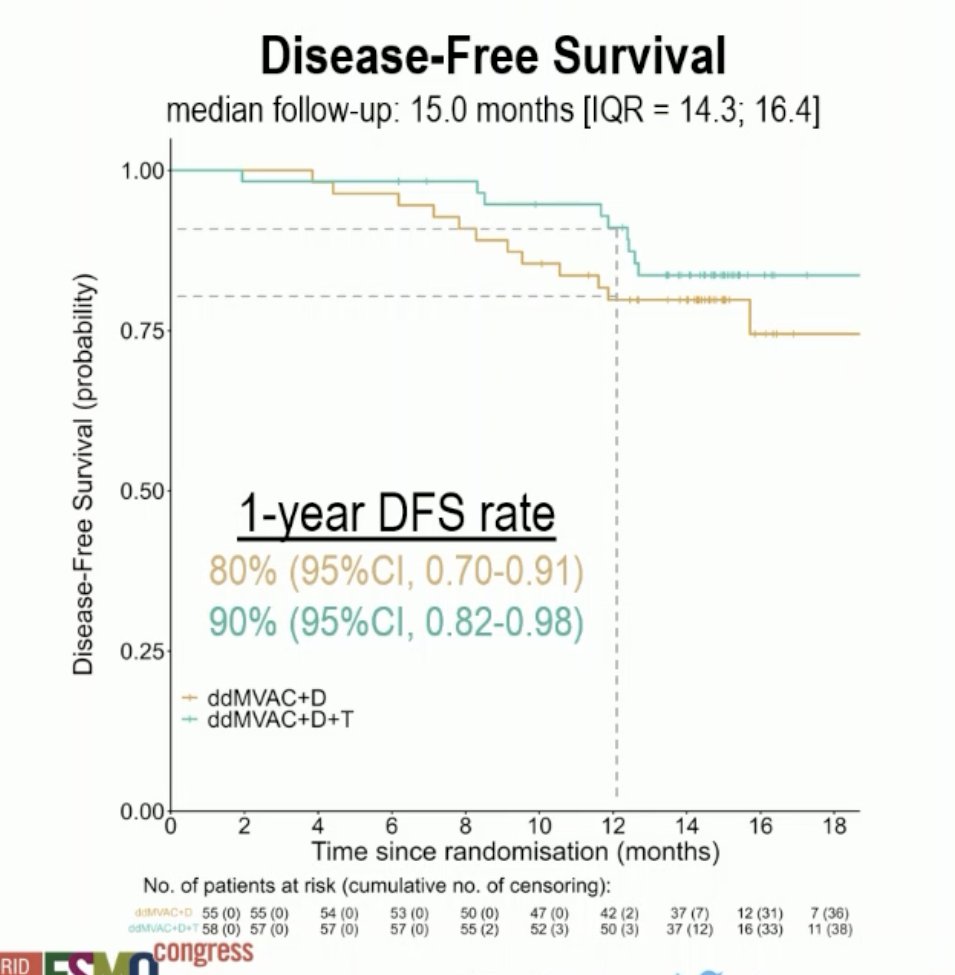
At a median follow-up of 16 months, the 1-year overall survival rates were 89% and 97%, respectively.
Dr. Thibault concluded that:
- The combination of neoadjuvant ddMVAC + durvalumab +/- tremelimumab was safe and the full treatment course has been delivered in the vast majority of MIBC patients (≥75%)
- No delay in cystectomy
- No unexpected toxicity, no treatment related death
- Pathological complete response rate was 48% and only 34% had residual muscle-invasive disease after ddMVAC (4 cycles) + durvalumab +/- tremelimumab (2 cycles).
- Longer term follow-up data are pending with 2-year disease-free and overall survival rates expected for Q2 2024.
- Molecular and immunological translational research projects are ongoing
- molecular subtypes, TMB, cDNA,
- TLS, tumor immune microenvironment, immunological signature, metabolomic profile
Presented by: Constance Thibault, MD, Medical Oncology, Hôpital Européen Georges-Pompidou (Hôpitaux Universitaires Paris-Ouest), Paris, France
Written by: Rashid K. Sayyid, MD, MSc – Society of Urologic Oncology (SUO) Clinical Fellow at The University of Toronto, @rksayyid on Twitter during the 2023 European Society of Medical Oncology (ESMO) Annual Congress held in Madrid, Spain between October 20th and 24th, 2023
Reference: