She began by discussing key questions for men with non-metastatic prostate cancer who are receiving radiotherapy:
1 – who should have ADT added to their radiotherapy?
2 – what is the optimal duration of ADT?
This is relevant in three settings where radiotherapy is commonly delivered: as primary treatment men with localized disease, in the adjuvant setting following radical prostatectomy, and in the salvage setting following radical prostatectomy.
In the context of primary treatment of patients with localized, treatment-naïve prostate cancer. There is a clear demonstrated benefit (based on meta-analysis of 12 randomized trials) that the addition of ADT to radiotherapy improves metastasis-free survival for patients with intermediate and high-risk disease. Thus, the ESMO guidelines recommend 4-6 months of therapy for those being treated for intermediate-risk disease and 18-36 months of therapy for those being treated for high-risk disease.
However, the data to inform this question in the post-operative setting is much less clear. There is essentially no strong evidence in the adjuvant setting while there is some data from RTOG 9601, GETUF-AFU-16, and RTOG 0534 regarding the use in the salvage setting for biochemical failure. However, this fails to address the question of duration. Thus, given this evidence void, the most recent version of the ESMO guidelines note that “concomitant ADT with LHRH agonist for 6 months or bicalutamide for 2 years may be offered” to these patients. Dr. Gillessen emphasized the vagueness of these recommendations.
She noted that RADICALS-HD is an academic, pragmatic effort including a large number of patients that addresses large, unanswered questions. However, given its scope, it is a complex trial design with multiple questions and many comparisons across two different settings (adjuvant and salvage). Further, it was begun 15 years ago and standards of care have evolved during that time (including particularly the imaging approaches employed). Additionally, hormonal treatments were not standardized and patients and investigators could choose which of the randomizations to participate in. As expected based on this, patients in the none-vs-short randomization were less likely to have T3b/4 disease or Gleason 8-10 histology. Rates of 2 or 3 risk factors were much lower as well (16% vs 35%).

Thus, given these differences in patient characteristics, Dr. Gillessen suggested that we may well consider the two comparisons as two different trials. Correspondingly, the adjuvant therapy setting was somewhat more common in the short-vs-long comparison. In both comparisons, most patients (84%) received LHRH agonists while the remainder received bicalutamide.
The study was designed with the primary endpoint of metastasis-free survival, after revision from cause-specific survival. Dr. Gillessen righted that MFS has been shown to be a valid surrogate for overall survival in patients ith localized prostate cancer.
In the none-vs-short randomization, two prior trials have addressed a similar question: RTOG 0534 and GETUG-AFU-16. Comparing between the trials, Dr. Gillessen noted that this RADICALS-HD comparison includes a meaningful proportion of patients receiving adjuvant therapy, and thus the median PSA is lower. Comparing across trials, Dr. Gillessen noted that there are mixed results assessing the benefit of short-term ADT.
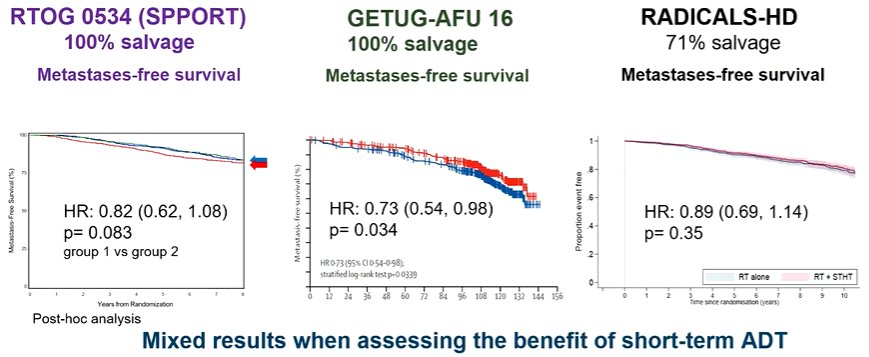
Only GETUG-AFU-16 has demonstrated a significant survival benefit. However, the DADSPORT meta-analysis which was presented yesterday at ESMO demonstrated, in a pooled analysis, a significant benefit (HR 0.82, 95% CI 0.70-0.96) to the use of 6 months of ADT compared to no ADT. At 5 years, this translates to an overall absolute benefit of 2%. She further noted that many patients in this setting will do very well with radiotherapy alone (6-year MFS exceeds 80%).
Moving to the second randomization of short-versus-long ADT, she noted that the RTOG 9601 trial has previously assessed this and showed an overall survival benefit to the use of 2 years of ADT. She noted that this trial was restricted to patients in the later salvage setting, with higher PSA levels, and lower doses of radiotherapy administered. Notably, subgroup analyses suggested that most of the benefit to this approach was from patients with baseline PSA exceeding 1.5 ng/mL at the time of radiotherapy. However, RADICALS-HD showed a statistically significant improvement in metastasis-free survival for patients receiving longer durations of ADT, both compared to shorter durations of therapy and compared to none). Again, however, she noted that the vast majority of patients treated with short-durations of ADT are also doing well in the short term.
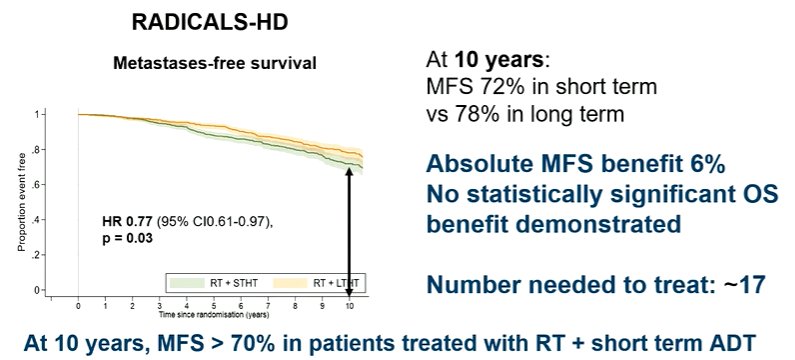
Summarizing these results, she noted that adding short-term ADT to salvage RT in a better-risk population results in small incremental improvements in MFS. However, many patients appear to do well with radiotherapy alone. Thus, longer-term follow-up is needed to better understand these outcomes and help guide patient selection. In patients with higher risk disease, the prolongation of ADT treatment from 6 months to 2 years resulted in improvements in MFS. However, many patients in the short-term arm did very well. Thus, quality of life data may be important when considering the toxicity of ADT.
Moving forward, she noted that next-generation imaging is increasingly used in the post-operative setting. Further, there is increasing utilization of pelvic nodal radiotherapy as well as of radical prostatectomy in high-risk patients.
Concluding, she noted that there is evidence that some patients will benefit with intensification from none to short-term ADT and others with intensification from short-term to long-term ADT. However, we need better approaches to select these patients. One such approach is genomic classifiers: prior work has shown that there is a greater benefit from the addition of ADT among those with high-risk GC. An alternative may be based on artificial intelligence-based assessment of histology slides. Until such time as these are validated, standard clinicopathologic characteristics will continue to inform treatment choice including age, comorbidity, Gleason score, PSA doubling time, pre-salvage RT PSA, and margin status, all in the context of patient preferences. Further, meta-analysis of subgroup data may allow better identification of subgroups with particular benefit. Additionally, she noted that some patients with particularly high risk may benefit from further systemic treatment intensification with the use of novel androgen receptor pathway inhibitors. Thus, she noted that our goal should be optimal treatment intensification, in those patients who most need it.
Presented by: Prof. Dr. Med. Silke Gillessen, Medical and Scientific Director, L'Istituto Oncologico della Svizzera Italiana (IOSI), and Co-founder of the Advanced Prostate Cancer Consensus Conference (APCCC).Written by: Christopher J.D. Wallis, University of Toronto Twitter: @WallisCJD during the 2022 European Society for Medical Oncology (ESMO) Annual Congress, 9-13 September 2022.