(UroToday.com) The European Society of Medical Oncology (ESMO) 2021 annual meeting’s non-prostate cancer proffered paper session included a presentation by Dr. Janet Brown discussing results of the phase II/III STAR trial assessing standard first-line therapy comparing cessation of treatment versus allowing continuation in the treatment of metastatic renal cell carcinoma (RCC). There is increasing interest in using treatment breaks in oncology, to reduce toxicity without compromising efficacy. The STAR trial opened in 2012 in the UK, after sunitinib was approved as the first TKI, and was designed to determine if a tyrosine kinase inhibitor drug-free interval strategy was non-inferior to a conventional continuation strategy in the first line treatment of advanced RCC.
STAR is a UK Phase II/III multicenter, randomized controlled trial. Patients were randomized (1:1) to drug-free interval strategy or conventional continuation strategy. After 24 weeks of sunitinib/pazopanib treatment, drug-free interval strategy patients took a treatment break, until disease progression, with additional breaks dependent on disease response and patient/clinician choice. The trial strategy continued until intolerance, progression on treatment or death. Both co-primary endpoints (OS and QALYs) must demonstrate pre-defined non-inferiority (≤7.5% OS; ≤ 10% QALYs) in intention-to-treat and per-protocol analyses for non-inferiority to be concluded. The trial schema for STAR is as follows:

There were 920 patients randomized (461 conventional continuation strategy vs 459 drug-free interval strategy) at 60 centers in the UK. Intention-to-treat and per-protocol analyses included 461 vs 458 and 453 vs 418 patients, respectively. The median follow-up in the intention-to-treat population was 58 months (IQR 46-73), and 13,147 out of 16,726 (78.6%) of quality of life booklets were returned. Overall, 488 (53.0%) patients (240 (52.1%) vs 248 (54.0%)) continued on the trial post-week 24. At least one treatment break was mandated, with a median treatment break length of 87 days (IQR 84-119). The total number of breaks are listed as follows:

There was a difference in conclusion in the OS analysis precluding confirmation of non-inferiority (HR intention-to-treat: 0.97 (95% CI 0.83, 1.12); per-protocol: HR 0.94 (95% CI 0.80, 1.09) non-inferiority margin: 95% CI ≥ 0.812):

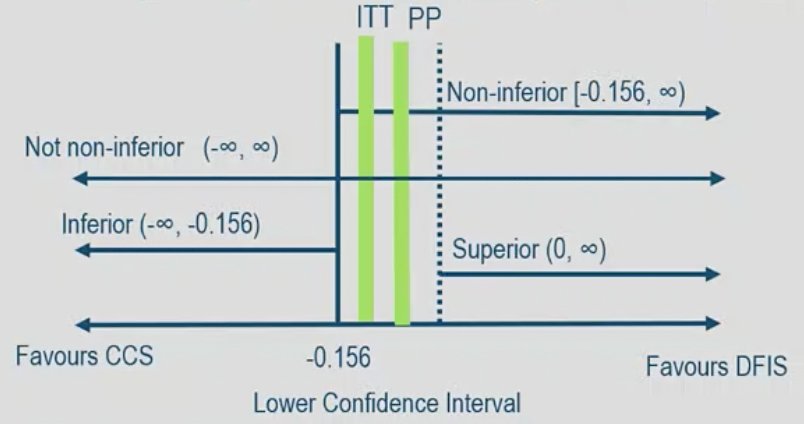
However consistent non-inferiority conclusions were found for QALYs (marginal effect, intention-to-treat: -0.05 (95% CI -0.15, 0.05); per-protocol: 0.04 (95% CI -0.14, 0.21) non-inferiority margin: 95% CI ≥ -0.156). At two years, the drug-free interval strategy was associated with cost savings of £6,954 per-participant:
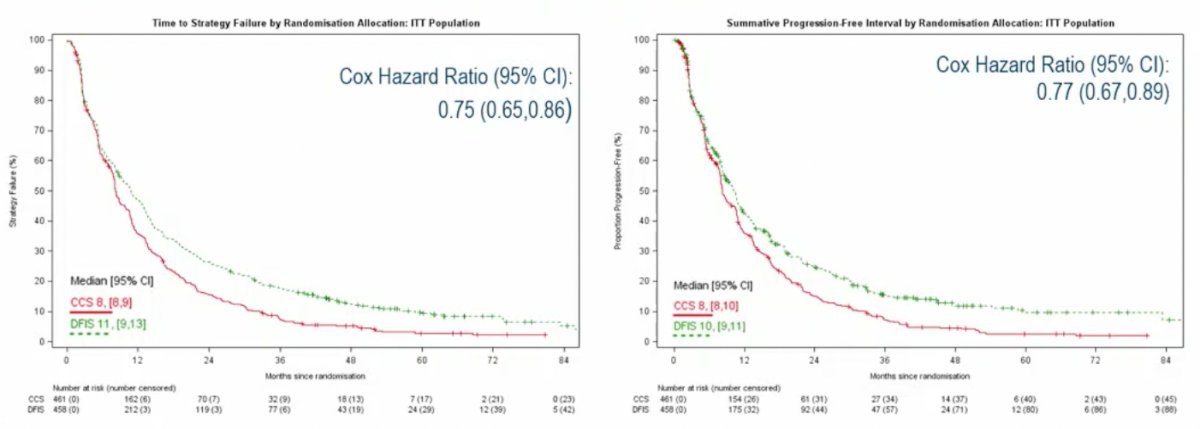
Both time to strategy failure (time to death, disease progression, new systemic treatment) and summative progression-free interval (total time progression-free accounting for disease response following a treatment break in the drug-free interval strategy arm) showed significant differences in favor of the drug-free interval strategy arm when considered in an adjusted Cox proportional hazards model:
Considering serious adverse events, deemed to be related to TKI treatment, a small proportion of participants in the drug-free interval strategy arm experienced an event, and participants in the drug-free interval strategy arm accounted for fewer of the overall events compared to the conventional continuation strategy.
Dr. Brown concluded her presentation of the STAR trial with the following take-home messages:
- Treatment breaks were acceptable to patients and clinicians, were not detrimental to overall survival or quality of life, and had significant cost savings
- 42.7% of patients in the drug-free interval strategy arm who continued post-week-24 had multiple treatment breaks. Further exploratory analysis will consider the characteristics of patients who benefited from a treatment break
- Although immunotherapy is now first-line therapy for many patients, TKIs remain the most appropriate treatment for some patients in the first-line setting, and many others in the second-line setting
Presented by: Janet E. Brown, MD, Oncology and Metabolism, University of Sheffield, Leeds, UK
Written by: Zachary Klaassen, MD, MSc – Urologic Oncologist, Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia, @zklaassen_md on Twitter during the 2021 European Society for Medical Oncology (ESMO) Annual Congress 2021, Thursday, Sep 16, 2021 – Tuesday, Sep 21, 2021.