
As cabozantinib may promote an immune-permissive environment to enhance the efficacy of immunotherapy, cabozanitinb is being evaluated in combination with immunotherapy in multiple clinical contexts. Notably, the combination of cabozantinib with nivolumab has been shown to be superior with regards to progression-free and overall survival to sunitinib as first line therapy for advanced clear cell RCC (CheckMate 9ER, ESMO 2020). In this poster, Dr. McGregor and colleagues present the study design and initial results of cohort 10 of the phase 1b COSMIC-021 trial, the combination of cabozantinib and the anti-PD-L1 agent atezolizumab in patients with non-clear cell RCC. The study schema is shown below.
The primary endpoint of the study was investigator-assessed objective response rate, with secondary and exploratory objectives of safety, duration of response, progression free survival, overall survival, and biomarker analyses. Patients with non clear-cell RCC, including those with sarcomatoid component, were eligible for trial if they had measurable disease. One prior therapy with a VEGFR TKI was permitted, but prior MET TKI therapy or immune checkpoint blockade was not allowed. Treatment was administered with 40 mg of cabozantinib daily and 1200 mg atezolizumab every three weeks. The maximum reduction in cabozantinib based on adverse events was to 20 mg QOD. Tumor assessment was performed every 6 weeks for the first 12 months, then every 13 weeks. PD-L1 was assessed by immunohistochemistry with the SP142 anti-PD-L1 assay (Ventana), with positive expression defined as combined positive score >= 1%. Immunophenotyping of whole blood by flow cytometry was performed prior to and after 21 days of treatment for biomarker correlative analysis.
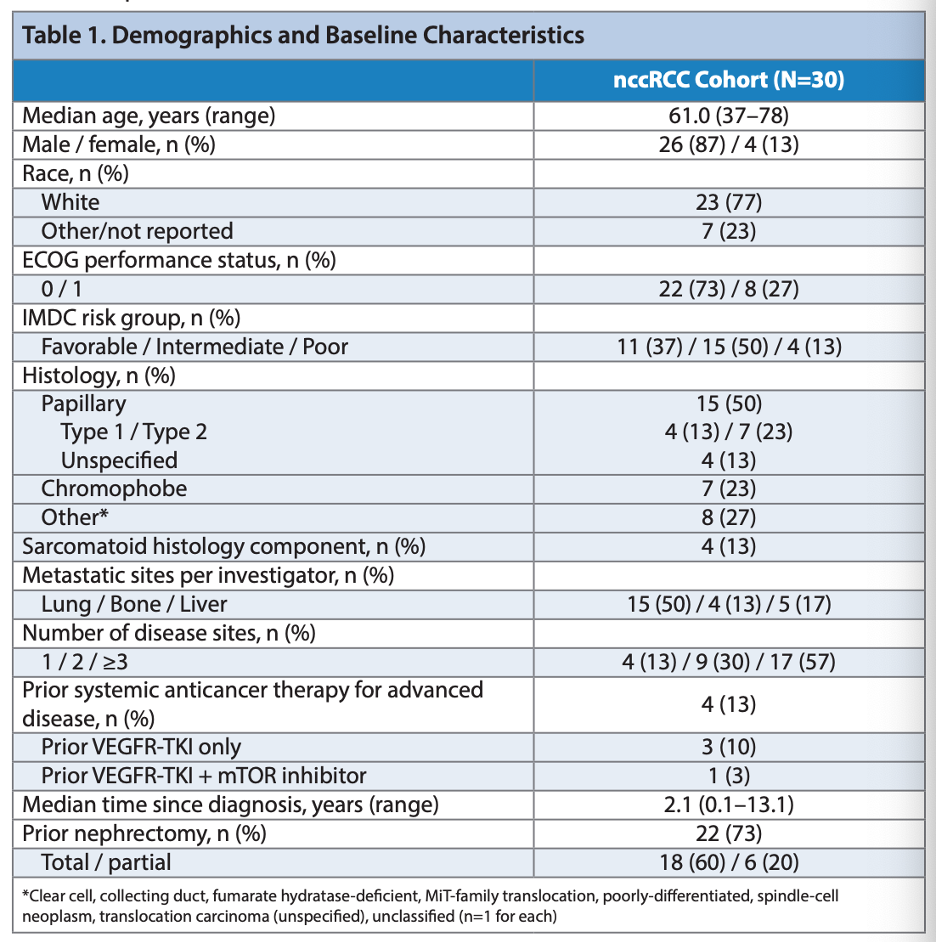
As of the data cutoff, 30 patients were enrolled. Results were reported with a median follow-up of 13 months. 16 patients remained on treatment at the data cutoff. The patient demographics are shown below.
Treatment resulted in an objective response rate of 33%, with 28 of 30 patients have disease control while on treatment. Responses occurred relatively quickly, with the median time to response of 2.7 months. Responses were seen across the various histologies enrolled. The median progression-free survival was 9.5 months.
Regarding safety, 11 patients suffered grade 3 or 4 treatment related adverse events, and 4 patients sustained a grade 3 or 4 immune related event. Four patients had TrAEs from cabozantinib leading to discontinuation, and 2 patients had IrAEs related to atezolizumab leading to discontinuation. The most common adverse events was diarrhea (60% of patients), followed by dysgeusia, fatigue, nausea, and palmar-plantar erythrodysthesia. The most common grade 3 or 4 toxicity was hypophosphatemia. The most common IrAE was rash, and grade 3 or 4 IrAEs included rash, hyperthyroidism, myocarditis and pancreatitis in 1 patient each. To patients required high-dose corticosteroids to manage immune related adverse events.
Correlative flow cytometry before and after 21 days of treatment showed increases in the concentration of cytotoxic cells (lymphocytes and NK cells), decreases in myeloid and myeloid derived suppressor cells, and an increased ratio in NK/mono cells. PD-L1 positivity did not associate with response.
In summary, cabozantinib plus atezolizumab demonstrated clinical activity in non-clear cell RCC across various histologies and induced changes in peripheral immune cell numbers. This drug combination is being further evaluated in the CONTACT-03 trial in RCC patients previously treated with immune checkpoint blockade, including non-clear cell RCCs.
Presented by: Bradley McGregor, MD, Clinical Director of the Lank Center for Genitourinary Oncology and Senior Physician, Dana-Farber Cancer Institute, Boston, MA
Written by: Alok Tewari, MD, PhD, Medical Oncologist at the Dana-Farber Cancer Institute, at the 2020 European Society for Medical Oncology Virtual Congress (#ESMO20), September 19th-September 21st, 2020.Related Content:
ESMO Virtual Congress 2020: Cabozantinib in Combination with Atezolizumab in Non-Clear Cell Renal Cell Carcinoma: Results from Cohort 10 of the COSMIC-021 Study