- Abstract 904PD Pre-operative ipilimumab and nivolumab in locoregionally advanced, stage III, urothelial cancer (NABUCCO)
- Abstract 905PD Multiple-cohort analysis investigating FGFR3 alteration as a predictor of non-response to neoadjuvant pembrolizumab in muscle-invasive bladder cancer
- Abstract 906PD Phase 3 trial of adjuvant sunitinib in patients with high-risk renal cell carcinoma: comprehensive tumor genomic and transcriptomic analyses.
Dr. Bellmunt notes that there are other ongoing nivolumab/ipilimumab neoadjuvant trials ongoing:
-
CA209-9DJ: A pilot study evaluating the safety of neoadjuvant nivolumab alone or in combination with ipilimumab for cisplatin ineligible patients with MIBC
-
CA017-078: Peri-surgical phase III trial of nivolumab +/- BMS-986205 (IDO inhibitor) + chemotherapy in MIBC
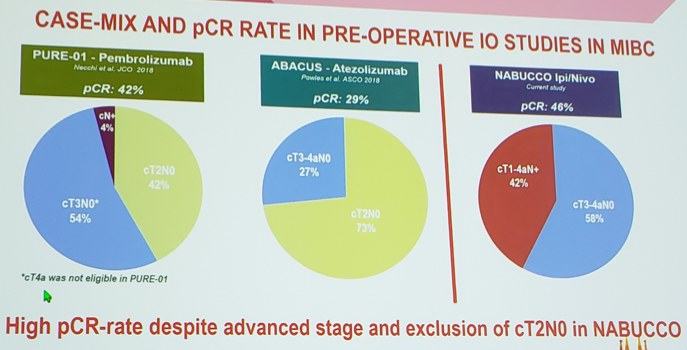
Dr. Bellmunt highlighted the following comments for the NABUCCO trial:
- This is a different population than those in the PURE-01 and ABACUS trials
- This highlights an unmet clinical need: Surgically incurable/resectable after treatment didn’t have a different outcome than M1, despite surgery (EORTC 30987 [1])
- Long-term follow-up is needed, specifically regarding the patients with a better response in the primary than in the lymph nodes
- Other schedules are begin explored in order to minimize toxicity
The subset analysis of the PURE-01 study investigated FGFR3 alteration as a predictor of non-response to neoadjuvant pembrolizumab for patients with muscle-invasive bladder cancer. The PURE-01 protocol was amended to include a more heterogeneous population (n=136) and focused on potential predictive markers. Necchi and colleagues found that FGFR3 alterations are not associated with pathologic response to pembrolizumab: 29.5% of patients harbored ESCAT tier >=1-2 genomic alterations suggesting benefit from approved or investigational targeted therapies. Tier 1B was represented by FGFR3 genomic alteration (n=17, 15.2%). Furthermore, there were no significant differences in the frequency of genomic alterations between the pathologic response categories, including FGFR3 genomic alteration. The Immune190 score is an expression of immune genes inversely correlated with PPAR-gamma expression. The RNA immune signatures are statistically significantly associated to pathological response to neoadjuvant pembrolizumab but not neoadjuvant chemotherapy. Dr. Bellmunt notes that genetic alteration is a vague term and we need to better define SNV or mRNA expression. Additionally, he notes that there is conflicting evidence as to what FGFR alteration tumors response best to: in 22 patients previously treated with immunotherapy, the ORR was 59% for erdafitinib. Further work assessing how best to treat FGFR alteration patients is required.
The phase 3 trial of adjuvant sunitinib for patients with high-risk RCC (S-TRAC) assessed comprehensive tumor genomic and transcriptomic analyses. Overall, there were 171 patients (sunitinib, n = 91; placebo, n = 80) were genotyped and 133 (sunitinib, n = 72; placebo, n = 61) were included in the gene expression signature analyses. Patients in the placebo arm with mutations in WDFY4 or CSPG4 had shorter DFS compared with sunitinib treated patients who had no mutation detected in either gene. Low tumor mutational burden was associated with a longer DFS in patients in the placebo arm (HR 0.289, 95% CI 1.405-5.932), but did not influence DFS in the sunitinib arm. Ultimately, different effects on DFS were observed between treatment groups according to the expression of specific genes. When assessed by various gene expression signatures, low-angiogenesis gene expression signature showed a modest association with shorter DFS vs high- angiogenesis gene expression signature in placebo (HR 1.912; 95% CI 0.829-4.409) but did not differentiate DFS in sunitinib. Patients with low-Minf gene expression signature in sunitinib had longer DFS vs those with high-Minf gene expression signature (HR 0.304; 95% CI 0.132-0.702). Using the new JAVELIN Renal 101 signature, high expression of the signature showed a modest association with prolonged DFS vs low expression in the placebo (HR 0.42; 95% CI 0.18-0.98) and in the sunitinib arm (HR 0.51; 95% CI 0.24-1.08). Dr. Bellmunt concluded that genomic analysis of high-risk RCC can help identify patients who may benefit from adjuvant sunitinib.
Presented by: Joaquim Bellmunt, MD, Associate Professor of Medicine, Beth Israel, Boston, MA
Written by: Zachary Klaassen, MD, MSc – Assistant Professor of Urology, Georgia Cancer Center, Augusta University/Medical College of Georgia Twitter: @zklaassen_md at the 2019 European Society for Medical Oncology annual meeting, ESMO 2019 #ESMO19, 27 Sept - 1 Oct 2019 in Barcelona, Spain
Reference: